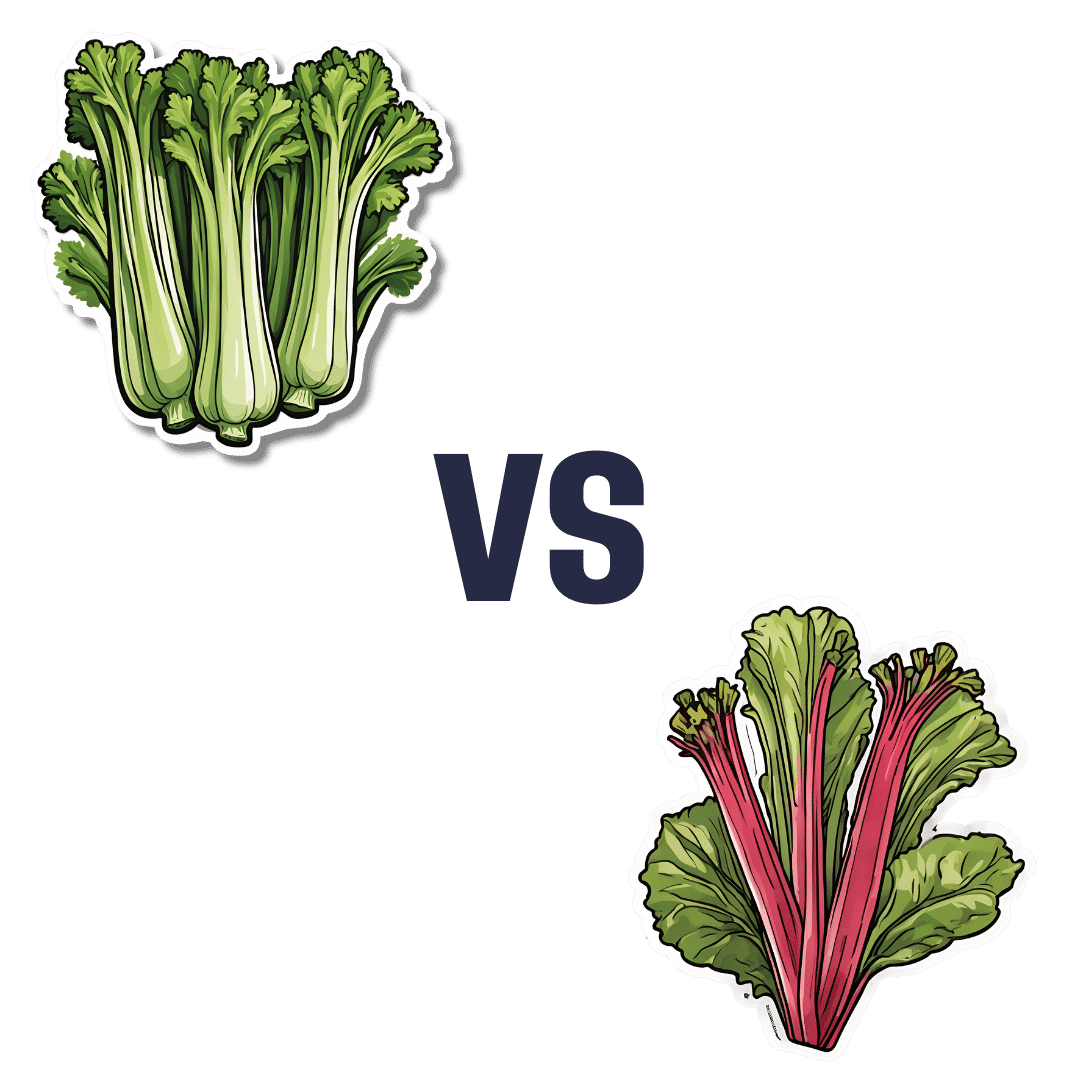
Celery vs Rhubarb – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing celery to rhubarb, we picked the rhubarb.
Why?
In terms of macros, rhubarb has more carbs and fiber, the ratio of which give it the lower glycemic index, though both are low glycemic index foods. This means this category is a very marginal win for rhubarb.
When it comes to vitamins, rhubarb has more vitamin C, while celery has more of vitamins A, B5, B6, and B9. A win for celery, this time.
In the category of minerals, rhubarb has more calcium, iron, magnesium, manganese, potassium, and selenium, while celery has more copper and phosphorus. This one’s a win for rhubarb.
Let’s give a quick nod also to polyphenols; rhubarb has more by overall quantity, and more in terms of “more useful to humans” too, being rich in an assortment of flavanols while celery must make do with some furanocoumarins.
In short, enjoy either or both, but nutritional density is a great reason to get some rhubarb in!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

10 Ways To Delay Aging

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Colin Rose; he is a Senior Associate of the Royal Society of Medicine. He’s also a main contributor to EduScience, a program funded by the E.U. which is designed to enhance the teaching and learning of science in schools in Europe.
His most recent work has been about aging—and how to delay it. We also reviewed his latest book, here:
Delay Ageing – by Dr. Colin Rose
So, what does he want us to know? The key lies in his compilation of ten ways in which we age on a cellular level, and what we can to do slow each one of those:
Damage to DNA accumulates
While DNA can get damaged without any external stimulus to cause that, there are a lot of modifiable factors that we can do to reduce DNA damage. The list is easy: if it causes cancer, it causes aging.
Thus, check out: Stop Cancer 20 Years Ago
Cells become senescent
Our cells are replaced all the time; some sooner than others, but all of them at some point. The problem occurs when cells are outliving their usefulness. If a cell becomes completely immortal, that is cancer, but happily most don’t. Nevertheless, having senescent (aging) cells in the body means that those senescent cells are what get copied forwards by mitosis, and our DNA becomes like a photocopy of a tattered old photocopy of a tattered old photocopy. Which, needless to say, is not good for our health. So, the best thing to do is to kill them earlier:
Yes, really: Fisetin: The Anti-Aging Assassin
Mitochondria become dysfunctional
Without properly functional mitochondria, no living human cell can do its job properly.
Options: 7 Ways To Boost Mitochondrial Health To Fight Disease
Beneficial genes are switched off, harmful genes are on
It’s easy to think of our genes as being immutable, but epigenetics means that our environment (amongst other factors) can mean that our gene expression changes.
Imagine it this way: your genes are a set of instructions for your body. However, your body will act or not on those instructions, depending on other factors. Hormones often play a big part in this; for example sex hormones tell the body which set of genetic instructions to read (and thus what kind of body to build/rebuild), and cortisol or oxytocin can tell the body which set of contingency plans to activate or suppress (respectively). A milder example is gray hair; genes have the program for it, but many other factors inform the body when, if, and how to do it.
Of more concern when it comes to aging is what goes on with more critical systems, such as the brain, in which the aforementioned DNA damage can cause unhelpful instructions to get interpreted, resulting in epigenetic changes that in turn facilitate age-related degeneration.
As to what can be done, see : Klotho: Unzipping The Genes Of Aging?
Stem cells become exhausted
Stem cells can become different kinds of cells, and thus they’re very useful for maintaining a healthy body. However, they get depleted with age. We can slow down the rate of loss, though; for example, intermittent fasting can help:
Per Dr. Li’s 5 Ways To Beat Cancer (And Other Diseases)
And for more detail, see:
Doctor’s Tip: Regeneration (stem cells) — one of your body’s five defense systems
(complete with lists of foods to eat or avoid for stem cell health)
Cells fail to communicate properly
Cells need to talk to each other constantly, to continue doing their jobs. We are one big organism, after all, and not a haphazard colony of the countless cells that constitute such. However, cell signalling gets worse with age, which in turn precipitates others age-related problems. Fortunately, there are nutrients that can improve cellular communication.
For example: PS, We Love You ← this is about phosphatidylserine, also called “PS”
Telomeres become shorter
These protective caps on our DNA suffer the wear-and-tear so that our DNA doesn’t have to. However, as they get shorter, the DNA can start suffering damage. For this reason, telomere length is considered one of the most “Gold Standard” markers of cellular aging.
Here’s what can be done for that: The Stress Prescription (Against Aging!)
The body fails to sense nutritional intake properly
This is mostly about insulin signalling (though problems can occur in other systems too, but we only have so much room here), so it’s important to take care of that.
See: Turn Back The Clock On Insulin Resistance
Proteins accumulate errors
This is due to DNA damage, of course, but there are specific things that can reduce protein error accumulation; see for example:
A quick fix – preventing protein errors extends lifespan
See also: Rapamycin Can Slow Aging By 20% (But Watch Out)
The microbiome becomes unbalanced
We at 10almonds often mention that gut health affects pretty much every other kind of health, and it’s true for aging as well. So, take care of that microbiome!
Here’s a primer: Gut Health 101
Want to know more about delaying aging beyond the cellular level?
Check out: Age & Aging: What Can (And Can’t) We Do About It?
Take care!
Share This Post
-

How To Beat Loneliness & Isolation
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Overcoming Loneliness & Isolation
One of the biggest mental health threats that faces many of us as we get older is growing isolation, and the loneliness that can come with it. Family and friends thin out over the years, and getting out and about isn’t always as easy as it used to be for everyone.
Nor is youth a guaranteed protection against this—in today’s world of urban sprawl and nothing-is-walkable cities, in which access to social spaces such as cafés and the like means paying the rising costs with money that young people often don’t have… And that’s without getting started on how much the pandemic impacted an entire generation’s social environments (or lack thereof).
Why is this a problem?
Humans are, by evolution, social creatures. As individuals we may have something of a spectrum from introvert to extrovert, but as a species, we thrive in community. And we suffer, when we don’t have that.
What can we do about it?
We can start by recognizing our needs, such as they are, and identifying to what extent they are being met (or not).
- Some of us may be very comfortable with a lot of alone time—but need someone to talk to sometimes.
- Some of us may need near-constant company to feel at our best—and that’s fine too! We just need to plan accordingly.
In the former case, it’s important to remember that needing someone to talk to is not being a burden to them. Not only will our company probably enrich them too, but also, we are evolved to care for one another, and that itself can bring fulfilment to them as much as to you. But what if you don’t a friend to talk to?
- You might be surprised at who would be glad of you reaching out. Have a think through whom you know, and give it a go. This can be scary, because what if they reject us, or worse, they don’t reject us but silently resent us instead? Again, they probably won’t. Human connection requires taking risks and being vulnerable sometimes.
- If that’s not an option, there are services that can fill your need. For some, therapy might serve a dual purpose in this regard. For others, you might want to check out the list of (mostly free) resources at the bottom of this article
In the second case (that we need near-constant company to feel at our best) we probably need to look more at our overall lifestyle, and find ways to be part of a community. That can include:
- Living in a close-knit community (places with a lot of retirees in one place often have this; or younger folk might look at communal living/working spaces, for example)
- Getting involved in local groups (you can check out NextDoor.com or MeetUp.com for this)
- Volunteering for a charity (not only are acts of service generally fulfilling in and of themselves, but also, you will probably be working with other people of a charitable nature, and such people tend to make for good company!)
Need a little help?
There are many, many organizations that will love to help you (or anyone else) overcome loneliness and isolation.
Rather than list them all here and make this email very long by describing how each of them works, here’s a great compilation of resources:
Share This Post
-
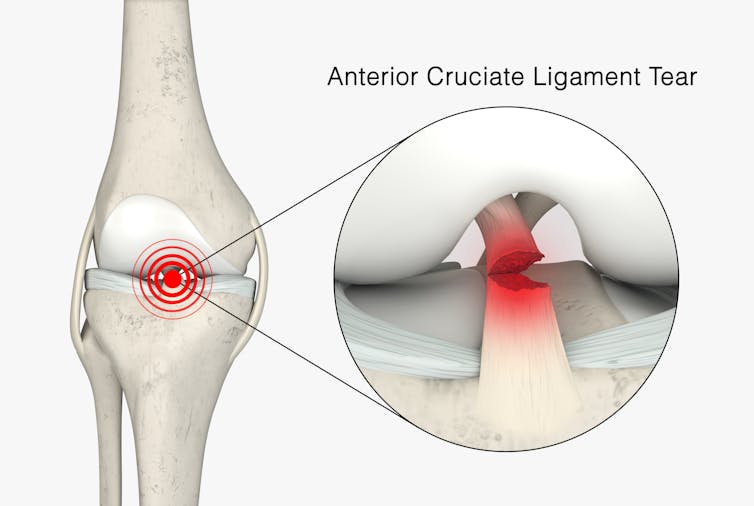
Surgery is the default treatment for ACL injuries in Australia. But it’s not the only way
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The anterior cruciate ligament (ACL) is an important ligament in the knee. It runs from the thigh bone (femur) to the shin bone (tibia) and helps stabilise the knee joint.
Injuries to the ACL, often called a “tear” or a “rupture”, are common in sport. While a ruptured ACL has just sidelined another Matildas star, people who play sport recreationally are also at risk of this injury.
For decades, surgical repair of an ACL injury, called a reconstruction, has been the primary treatment in Australia. In fact, Australia has among the highest rates of ACL surgery in the world. Reports indicate 90% of people who rupture their ACL go under the knife.
Although surgery is common – around one million are performed worldwide each year – and seems to be the default treatment for ACL injuries in Australia, it may not be required for everyone.

PeopleImages.com – Yuri A/Shutterstock What does the research say?
We know ACL ruptures can be treated using reconstructive surgery, but research continues to suggest they can also be treated with rehabilitation alone for many people.
Almost 15 years ago a randomised clinical trial published in the New England Journal of Medicine compared early surgery to rehabilitation with the option of delayed surgery in young active adults with an ACL injury. Over half of people in the rehabilitation group did not end up having surgery. After five years, knee function did not differ between treatment groups.
The findings of this initial trial have been supported by more research since. A review of three trials published in 2022 found delaying surgery and trialling rehabilitation leads to similar outcomes to early surgery.
A 2023 study followed up patients who received rehabilitation without surgery. It showed one in three had evidence of ACL healing on an MRI after two years. There was also evidence of improved knee-related quality of life in those with signs of ACL healing compared to those whose ACL did not show signs of healing.
Experts used to think an ACL tear couldn’t heal without surgery – now there’s evidence it can. SKYKIDKID/Shutterstock Regardless of treatment choice the rehabilitation process following ACL rupture is lengthy. It usually involves a minimum of nine months of progressive rehabilitation performed a few days per week. The length of time for rehabilitation may be slightly shorter in those not undergoing surgery, but more research is needed in this area.
Rehabilitation starts with a physiotherapist overseeing simple exercises right through to resistance exercises and dynamic movements such as jumping, hopping and agility drills.
A person can start rehabilitation with the option of having surgery later if the knee remains unstable. A common sign of instability is the knee giving way when changing direction while running or playing sports.
To rehab and wait, or to go straight under the knife?
There are a number of reasons patients and clinicians may opt for early surgical reconstruction.
For elite athletes, a key consideration is returning to sport as soon as possible. As surgery is a well established method, athletes (such as Matilda Sam Kerr) often opt for early surgical reconstruction as this gives them a more predictable timeline for recovery.
At the same time, there are risks to consider when rushing back to sport after ACL reconstruction. Re-injury of the ACL is very common. For every month return to sport is delayed until nine months after ACL reconstruction, the rate of knee re-injury is reduced by 51%.
For people who opt to try rehabilitation, the option of having surgery later is still there. PeopleImages.com – Yuri A/Shutterstock Historically, another reason for having early surgical reconstruction was to reduce the risk of future knee osteoarthritis, which increases following an ACL injury. But a review showed ACL reconstruction doesn’t reduce the risk of knee osteoarthritis in the long term compared with non-surgical treatment.
That said, there’s a need for more high-quality, long-term studies to give us a better understanding of how knee osteoarthritis risk is influenced by different treatments.
Rehab may not be the only non-surgical option
Last year, a study looking at 80 people fitted with a specialised knee brace for 12 weeks found 90% had evidence of ACL healing on their follow-up MRI.
People with more ACL healing on the three-month MRI reported better outcomes at 12 months, including higher rates of returning to their pre-injury level of sport and better knee function. Although promising, we now need comparative research to evaluate whether this method can achieve similar results to surgery.
What to do if you rupture your ACL
First, it’s important to seek a comprehensive medical assessment from either a sports physiotherapist, sports physician or orthopaedic surgeon. ACL injuries can also have associated injuries to surrounding ligaments and cartilage which may influence treatment decisions.
In terms of treatment, discuss with your clinician the pros and cons of management options and whether surgery is necessary. Often, patients don’t know not having surgery is an option.
Surgery appears to be necessary for some people to achieve a stable knee. But it may not be necessary in every case, so many patients may wish to try rehabilitation in the first instance where appropriate.
As always, prevention is key. Research has shown more than half of ACL injuries can be prevented by incorporating prevention strategies. This involves performing specific exercises to strengthen muscles in the legs, and improve movement control and landing technique.
Anthony Nasser, Senior Lecturer in Physiotherapy, University of Technology Sydney; Joshua Pate, Senior Lecturer in Physiotherapy, University of Technology Sydney, and Peter Stubbs, Senior Lecturer in Physiotherapy, University of Technology Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

How Likely Are You To Live To 100?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How much hope can we reasonably have of reaching 100?
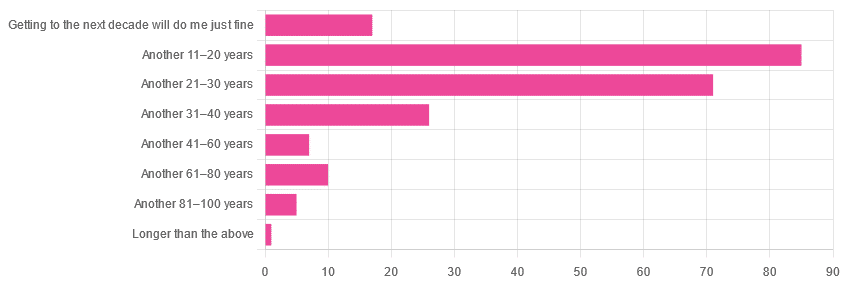
Yesterday, we asked you: assuming a good Health-Related Quality of Life (HRQoL), how much longer do you hope to live?

We got the above-depicted, below-described, set of responses:
- A little over 38% of respondents hope to live another 11–20 years
- A little over 31% hope to live another 31–40 years
- A little over 7% will be content to make it to the next decade
- One (1) respondent hopes to live longer than an additional 100 years
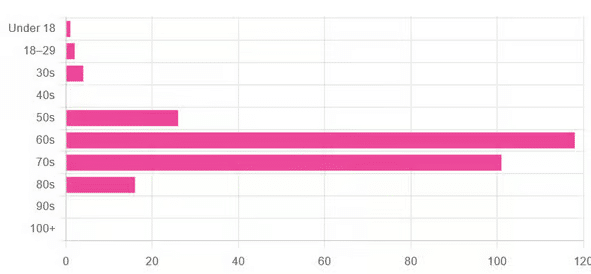
This is interesting when we put it against our graph of how old our subscribers are:

…because it corresponds inversely, right down to the gap/dent in the 40s. And—we may hypothesize—that one person under 18 who hopes to live to 120, perhaps.
This suggests that optimism remains more or less constant, with just a few wobbles that would probably be un-wobbled with a larger sample size.
In other words: most of our education-minded, health-conscious subscriber-base hope to make it to the age of 90-something, while for the most part feeling that 100+ is overly optimistic.
Writer’s anecdote: once upon a time, I was at a longevity conference in Brussels, and a speaker did a similar survey, but by show of hands. He started low by asking “put your hands up if you want to live at least a few more minutes”. I did so, with an urgency that made him laugh, and say “Don’t worry; I don’t have a gun hidden up here!”
Conjecture aside… What does the science say about our optimism?
First of all, a quick recap…
To not give you the same information twice, let’s note we did an “aging mythbusting” piece already covering:
- Aging is inevitable: True or False?
- Aging is, and always will be, unstoppable: True or False?
- We can slow aging: True or False?
- It’s too early to worry about… / It’s too late to do anything about… True or False?
- We can halt aging: True or False?
- We can reverse aging: True or False?
- But those aren’t really being younger, we’ll still die when our time is up: True or False?
You can read the answers to all of those here:
Age & Aging: What Can (And Can’t) We Do About It?
Now, onwards…
It is unreasonable to expect to live past 100: True or False?
True or False, depending on your own circumstances.
First, external circumstances: the modal average person in Hong Kong is currently in their 50s and can expect to live into their late 80s, while the modal average person in Gaza is 14 and may not expect to make it to 15 right now.
To avoid extremes, let’s look at the US, where the modal average person is currently in their 30s and can expect to live into their 70s:
United States Mortality Database
Now, before that unduly worries our many readers already in their 70s…
Next, personal circumstances: not just your health, but your socioeconomic standing. And in the US, one of the biggest factors is the kind of health insurance one has:
SOA Research Institute | Life Expectancy Calculator 2021
You may note that the above source puts all groups into a life expectancy in the 80s—whereas the previous source gave 70s.
Why is this? It’s because the SOA, whose primary job is calculating life insurance risks, is working from a sample of people who have, or are applying for, life insurance. So it misses out many people who die younger without such.
New advances in medical technology are helping people to live longer: True or False?
True, assuming access to those. Our subscribers are mostly in North America, and have an economic position that affords good access to healthcare. But beware…
On the one hand:
The number of people who live past the age of 100 has been on the rise for decades
On the other hand:
The average life expectancy in the U.S. has been on the decline for three consecutive years
COVID is, of course, largely to blame for that, though:
❝The decline of 1.8 years in life expectancy was primarily due to increases in mortality from COVID-19 (61.2% of the negative contribution).
The decline in life expectancy would have been even greater if not for the offsetting effects of decreases in mortality due to cancer (43.1%)❞
Source: National Vital Statistics Reports
The US stats are applicable to Canada, the UK, and Australia: True or False?
False: it’s not quite so universal. Differences in healthcare systems will account for a lot, but there are other factors too:
- Life expectancy in Canada fell for the 3rd year in a row. What’s happening?
- UK life expectancy lagging behind rest of G7 except the US
- Australians are living longer but what does it take to reach 100 years old?
Here’s an interesting (UK-based) tool that calculates not just your life expectancy, but also gives the odds of living to various ages (e.g. this writer was given odds of living to 87, 96, 100).
Check yours here:
Office of National Statistics | Life Expectancy Calculator
To finish on a cheery note…
Data from Italian centenarians suggests a “mortality plateau”:
❝The risk of dying leveled off in people 105 and older, the team reports online today in Science.
That means a 106-year-old has the same probability of living to 107 as a 111-year-old does of living to 112.
Furthermore, when the researchers broke down the data by the subjects’ year of birth, they noticed that over time, more people appear to be reaching age 105.❞
Pop-sci source: Once you hit this age, aging appears to stop
Actual paper: The plateau of human mortality: demography of longevity pioneers
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Live Long, Die Short – by Dr. Roger Landry
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First know: “die short” is not about your height—although on average, short people do live longer, partly because insulin-like growth factor (IGF-1) promotes both tallness and accelerated DNA damage (thus, aging and cancer), and partly because if someone is very tall, it can cause circulatory problems, and without a nice easy flow of blood through the brain, bad things happen (such as accumulation of harmful detritus in the brain, and increased stroke risk too).
Next know: “die short” is, in this book, actually about shortening the decline at the end of life. Sometimes people say “I don’t want to live 10 years longer; they’ll be the 10 most miserable years”, but in fact if we look after our health, we will be healthy for perhaps >9.5 of our last 10 years, while an unhealthy person may just get their expected “10 most miserable years” 10 or 20 years earlier (and then die).
So, in short (so to speak), it’s about increasing healthspan.
To enjoy the longest and healthiest healthspan, Dr. Landry offers 10 tips. We’ll not keep them a secret; they are:
- Use it or lose it
- Keep moving
- Challenge your brain
- Stay connected
- Lower your risks
- Never act your age
- Wherever you are, be fully there
- Find your purpose
- Have children in your life
- Laugh to a better life
Each of these has a chapter devoted to them, in section 2 of the book (section 1 is about what we know about healthy aging, and section 3 is about where we go from here).
You’ll notice that one item not generally found on such lists is “have children in your life”; to be clear, they don’t have to be your children, and/but they do have to be actual current children; any now-grown-up progeny aren’t what’s being talked about here (wonderful as they may be, any support role they may play gets filed under “stay connected” instead).
The style is mostly impersonal pop-science with occasional personal anecdotes, and the book’s formatting (many subheadings within chapters) makes it easy to read a bit at a time, if that’s your preference. There’s a modest, but extant, bibliography.
Bottom line: if you’d like to stay younger as you get older, this book goes into a lot of detail about 10 ways to do just that.
Click here to check out Live Long, Die Short, and live long, die short!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
If You’re Poor, Fertility Treatment Can Be Out of Reach
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Mary Delgado’s first pregnancy went according to plan, but when she tried to get pregnant again seven years later, nothing happened. After 10 months, Delgado, now 34, and her partner, Joaquin Rodriguez, went to see an OB-GYN. Tests showed she had endometriosis, which was interfering with conception. Delgado’s only option, the doctor said, was in vitro fertilization.
“When she told me that, she broke me inside,” Delgado said, “because I knew it was so expensive.”
Delgado, who lives in New York City, is enrolled in Medicaid, the federal-state health program for low-income and disabled people. The roughly $20,000 price tag for a round of IVF would be a financial stretch for lots of people, but for someone on Medicaid — for which the maximum annual income for a two-person household in New York is just over $26,000 — the treatment can be unattainable.
Expansions of work-based insurance plans to cover fertility treatments, including free egg freezing and unlimited IVF cycles, are often touted by large companies as a boon for their employees. But people with lower incomes, often minorities, are more likely to be covered by Medicaid or skimpier commercial plans with no such coverage. That raises the question of whether medical assistance to create a family is only for the well-to-do or people with generous benefit packages.
“In American health care, they don’t want the poor people to reproduce,” Delgado said. She was caring full-time for their son, who was born with a rare genetic disorder that required several surgeries before he was 5. Her partner, who works for a company that maintains the city’s yellow cabs, has an individual plan through the state insurance marketplace, but it does not include fertility coverage.
Some medical experts whose patients have faced these issues say they can understand why people in Delgado’s situation think the system is stacked against them.
“It feels a little like that,” said Elizabeth Ginsburg, a professor of obstetrics and gynecology at Harvard Medical School who is president-elect of the American Society for Reproductive Medicine, a research and advocacy group.
Whether or not it’s intended, many say the inequity reflects poorly on the U.S.
“This is really sort of standing out as a sore thumb in a nation that would like to claim that it cares for the less fortunate and it seeks to do anything it can for them,” said Eli Adashi, a professor of medical science at Brown University and former president of the Society for Reproductive Endocrinologists.
Yet efforts to add coverage for fertility care to Medicaid face a lot of pushback, Ginsburg said.
Over the years, Barbara Collura, president and CEO of the advocacy group Resolve: The National Infertility Association, has heard many explanations for why it doesn’t make sense to cover fertility treatment for Medicaid recipients. Legislators have asked, “If they can’t pay for fertility treatment, do they have any idea how much it costs to raise a child?” she said.
“So right there, as a country we’re making judgments about who gets to have children,” Collura said.
The legacy of the eugenics movement of the early 20th century, when states passed laws that permitted poor, nonwhite, and disabled people to be sterilized against their will, lingers as well.
“As a reproductive justice person, I believe it’s a human right to have a child, and it’s a larger ethical issue to provide support,” said Regina Davis Moss, president and CEO of In Our Own Voice: National Black Women’s Reproductive Justice Agenda, an advocacy group.
But such coverage decisions — especially when the health care safety net is involved — sometimes require difficult choices, because resources are limited.
Even if state Medicaid programs wanted to cover fertility treatment, for instance, they would have to weigh the benefit against investing in other types of care, including maternity care, said Kate McEvoy, executive director of the National Association of Medicaid Directors. “There is a recognition about the primacy and urgency of maternity care,” she said.
Medicaid pays for about 40% of births in the United States. And since 2022, 46 states and the District of Columbia have elected to extend Medicaid postpartum coverage to 12 months, up from 60 days.
Fertility problems are relatively common, affecting roughly 10% of women and men of childbearing age, according to the National Institute of Child Health and Human Development.
Traditionally, a couple is considered infertile if they’ve been trying to get pregnant unsuccessfully for 12 months. Last year, the ASRM broadened the definition of infertility to incorporate would-be parents beyond heterosexual couples, including people who can’t get pregnant for medical, sexual, or other reasons, as well as those who need medical interventions such as donor eggs or sperm to get pregnant.
The World Health Organization defined infertility as a disease of the reproductive system characterized by failing to get pregnant after a year of unprotected intercourse. It terms the high cost of fertility treatment a major equity issue and has called for better policies and public financing to improve access.
No matter how the condition is defined, private health plans often decline to cover fertility treatments because they don’t consider them “medically necessary.” Twenty states and Washington, D.C., have laws requiring health plans to provide some fertility coverage, but those laws vary greatly and apply only to companies whose plans are regulated by the state.
In recent years, many companies have begun offering fertility treatment in a bid to recruit and retain top-notch talent. In 2023, 45% of companies with 500 or more workers covered IVF and/or drug therapy, according to the benefits consultant Mercer.
But that doesn’t help people on Medicaid. Only two states’ Medicaid programs provide any fertility treatment: New York covers some oral ovulation-enhancing medications, and Illinois covers costs for fertility preservation, to freeze the eggs or sperm of people who need medical treatment that will likely make them infertile, such as for cancer. Several other states also are considering adding fertility preservation services.
In Delgado’s case, Medicaid covered the tests to diagnose her endometriosis, but nothing more. She was searching the internet for fertility treatment options when she came upon a clinic group called CNY Fertility that seemed significantly less expensive than other clinics, and also offered in-house financing. Based in Syracuse, New York, the company has a handful of clinics in upstate New York cities and four other U.S. locations.
Though Delgado and her partner had to travel more than 300 miles round trip to Albany for the procedures, the savings made it worthwhile. They were able do an entire IVF cycle, including medications, egg retrieval, genetic testing, and transferring the egg to her uterus, for $14,000. To pay for it, they took $7,000 of the cash they’d been saving to buy a home and financed the other half through the fertility clinic.
She got pregnant on the first try, and their daughter, Emiliana, is now almost a year old.
Delgado doesn’t resent people with more resources or better insurance coverage, but she wishes the system were more equitable.
“I have a medical problem,” she said. “It’s not like I did IVF because I wanted to choose the gender.”
One reason CNY is less expensive than other clinics is simply that the privately owned company chooses to charge less, said William Kiltz, its vice president of marketing and business development. Since the company’s beginning in 1997, it has become a large practice with a large volume of IVF cycles, which helps keep prices low.
At this point, more than half its clients come from out of state, and many earn significantly less than a typical patient at another clinic. Twenty percent earn less than $50,000, and “we treat a good number who are on Medicaid,” Kiltz said.
Now that their son, Joaquin, is settled in a good school, Delgado has started working for an agency that provides home health services. After putting in 30 hours a week for 90 days, she’ll be eligible for health insurance.
One of the benefits: fertility coverage.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: