Apples vs Figs – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apples to figs, we picked the figs.
Why?
These two fruits are both known for being quite rich in sugar (but also rich in fiber, which offsets it metabolically), and indeed their macros are quite similar. That said, figs have slightly more protein, fiber, and carbs. Both are considered low glycemic index foods. We can consider this category a tie, or perhaps a nominal win for apples, whose glycemic index is the lower of the two. But since figs’ GI is also low, it’s really not a deciding factor.
In terms of vitamins, apples have more of vitamins C and E, while figs have more of vitamins A, B1, B2, B3, B5, B6, B9, and choline, with noteworthy margins of difference. A clear for figs here.
When it comes to minerals, apples are not higher in any minerals, while figs are several times higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. An overwhelming win for figs.
Of course, enjoy either or both, but if you want nutritional density, apples simply cannot compete with figs.
Want to learn more?
You might like to read:
Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Ice Baths: To Dip Or Not To Dip?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

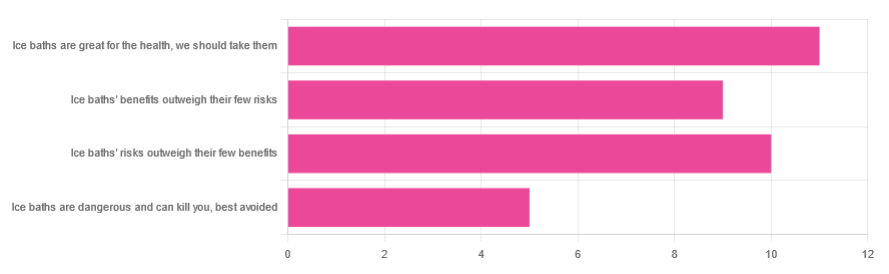
We asked you for your (health-related) view of ice baths, and got the above-depicted, below-described, set of responses:
- About 31% said “ice baths are great for the health; we should take them”
- About 29% said “ice baths’ risks outweigh their few benefits”
- About 26% said “ice baths’ benefits outweigh their few risks”
- About 14% said “ice baths are dangerous and can kill you; best avoided”
So what does the science say?
Freezing water is very dangerous: True or False?
True! Water close to freezing point is indeed very dangerous, and can most certainly kill you.
Fun fact, though: many such people are still saveable with timely medical intervention, in part because the same hypothermia that is killing them also slows down the process* of death
Source (and science) for both parts of that:
Cold water immersion: sudden death and prolonged survival
*and biologically speaking, death is a process, not an event, by the way. But we don’t have room for that today!
(unless you die in some sudden violent way, such as a powerful explosion that destroys your brain instantly; then it’s an event)
Ice baths are thus also very dangerous: True or False?
False! Assuming that they are undertaken responsibly and you have no chronic diseases that make it more dangerous for you.
What does “undertaken responsibly” mean?
Firstly, the temperature should not be near freezing. It should be 10–15℃, which for Americans is 50–59℉.
You can get a bath thermometer to check this, by the way. Here’s an example product on Amazon.
Secondly, your ice bath should last no more than 10–15 minutes. This is not a place to go to sleep.
What chronic diseases would make it dangerous?
Do check with your doctor if you have any doubts, as no list we make can be exhaustive and we don’t know your personal medical history, but the main culprits are:
- Cardiovascular disease
- Hypertension
- Diabetes (any type)
The first two are for heart attack risk; the latter is because diabetes can affect core temperature regulation.
Ice baths are good for the heart: True or False?
True or False depending on how they’re done, and your health before starting.
For most people, undertaking ice baths responsibly, repeated ice bath use causes the cardiovascular system to adapt to better maintain homeostasis when subjected to thermal shock (i.e. sudden rapid changes in temperature).
For example: Respiratory and cardiovascular responses to cold stress following repeated cold water immersion
And because that was a small study, here’s a big research review with a lot of data; just scroll to where it has the heading“Specific thermoregulative adaptations to regular exposure to cold air and/or cold water exposure“ for many examples and much discussion:
Health effects of voluntary exposure to cold water: a continuing subject of debate
Ice baths are good against inflammation: True or False?
True! Here’s one example:
Uric acid and glutathione levels (important markers of chronic inflammation) are also significantly affected:
Uric acid and glutathione levels during short-term whole body cold exposure
Want to know more?
That’s all we have room for today, but check out our previous “Expert Insights” main feature looking at Wim Hof’s work in cryotherapy:
A Cold Shower A Day Keeps The Doctor Away?
Enjoy!
Share This Post
-

Track Your Blood Sugars For Better Personalized Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There Will Be Blood
Are you counting steps? Counting calories? Monitoring your sleep? Heart rate zones? These all have their merits:
- Steps: One More Resource Against Osteoporosis!
- Calories: Is Cutting Calories The Key To Healthy Long Life?
- Sleep: A Head-To-Head Of Google and Apple’s Top Apps For Getting Your Head Down
- Heart Rate Zones: Heart Rate Zones, Oxalates, & More
About calories: this writer (it’s me, hi) opines that intermittent fasting has the same benefits as caloric restriction, without the hassle of counting, and is therefore superior. I also personally find fasting psychologically more pleasant. However, our goal here is to be informative, not prescriptive, and some people may have reasons to prefer CR to IF!
Examples that come to mind include ease of adherence in the case of diabetes management, especially Type 1, or if one’s schedule (and/or one’s “medications that need to be taken with food” schedule) does not suit IF.
And now for the blood…
A rising trend in health enthusiasts presently is the use of Continuous Glucose Monitors (CGMs), which do exactly what is sounds like they do: they continually monitor glucose. Specifically, the amount of it in your blood.
Of course, these have been in use in diabetes management for years; the technology is not new, but the application of the technology is.
A good example of what benefits a non-diabetic person can gain from the use of a CGM is Jessie Inchauspé, the food scientist of “Glucose Revolution” and “The Glucose Goddess Method” fame.
By wearing a CGM, she was able to notice what things did and didn’t spike her blood sugars, and found that a lot of the things were not stuff that people knew/advised about!
For example, much of diabetes management (including avoiding diabetes in the first place) is based around paying attention to carbs and little else, but she found that it made a huge difference what she ate (or didn’t) with the carbs. By taking many notes over the course of her daily life, she was eventually able to isolate these patterns, showed her working-out in The Glucose Revolution (there’s a lot of science in that book), and distilled that information into bite-size (heh) advice such as:
10 Ways To Balance Blood Sugars
That’s great, but since people like Inchauspé have done the work, I don’t have to, right?
You indeed don’t have to! But you can still benefit from it. For example, fastidious as her work was, it’s a sample size of one. If you’re not a slim white 32-year-old French woman, there may be some factors that are different for you.
All this to say: glucose responses, much like nutrition in general, are not a one-size-fits-all affair.
With a CGM, you can start building up your own picture of what your responses to various foods are like, rather than merely what they “should” be like.
This, by the way, is also one of the main aims of personalized health company ZOE, which crowdsourced a lot of scientific data about personalized metabolic responses to standardized meals:
Not knowing these things can be dangerous
We don’t like to scaremonger here, but we do like to point out potential dangers, and in this case, blindly following standardized diet advice, if your physiology is not standard, can have harmful effects, see for example:
Diabetic-level glucose spikes seen in non-diabetic people
Where can I get a CGM?
We don’t sell them, and neither does Amazon, but you can check out some options here:
The 4 Best CGM Devices For Measuring Blood Sugar in 2024
…and if your doctor is not obliging with a prescription, note that the device that came out top in the above comparisons, will be available OTC soon:
The First OTC Continuous Glucose Monitor Will Be Available Summer 2024
Take care!
Share This Post
-

Why Some Friendships Last And Others Don’t
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Friendships matter a lot, playing a significant role in our wellbeing, physical as well as mental. They bring additional meaning to our lives, help us cope with setbacks, and hopefully will be at our side through the highs and lows of life. And yet, for something that’s in principle good for everyone involved, there can be problems:
Friend to the end?
Firstly, some people find it harder to make (and then further deepen) friendships with others, which can be for a whole host of reasons.
Approaching new people can feel intimidating, but it’s a common struggle. Research shows that people often underestimate how much others enjoy their company, a phenomenon known as the “liking gap.” By reminding ourselves that others are likely to appreciate our presence and expecting to be well-received (the “acceptance prophecy”), we can approach social interactions with greater confidence.
As relationships grow, they often deepen through companionship and closeness:
- Companionship arises from shared hobbies, interests, or values, and it builds rapport.
- Closeness involves sharing thoughts, feelings, and experiences, which can build intimacy together.
An important key to these is consistency, which—whether through regular chats, honoring plans, or showing support—helps strengthen bonds, even in long-distance friendships (something often considered a barrier to closeness).
Even the strongest friendships can face challenges, of course. Conflicts may arise from a lack of support during difficult moments, or worse, betrayal. Or it could all be a misunderstanding. These situations are best addressed through honest, non-judgmental conversations. Avoiding defensiveness or accusations, and instead focusing on sharing feelings and understanding the other person’s perspective, can turn these tough discussions into opportunities for growth and stronger connections.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
How To Beat Loneliness & Isolation
Take care!
Share This Post


Related Posts
-

Being Mortal – by Dr. Atul Gawande
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Maybe you want to “live forever or die trying”, and that’s an understandable goal… But are you prepared for “or die trying” being the outcome?
This is not a cheerful book, if you’re anything like this reviewer, you will need a little towel or something to mop up the tears while you read. But it’s worth it.
Dying is one thing; fighting for life is even generally considered a noble endeavor. Suffering alone isn’t fun, losing independence can feel humiliating, and seeing someone who was always a tower of strength, now a frail shadow of their former self, reduced to begging for something that they’re “not allowed”, can be worse.
Do we want that for ourselves? For our loved ones? Can there be a happy medium between that, and the alternative to indeed “go gentle into that good night”?
Dr. Gawande, a surgeon well-acquainted with death and dying, thinks so. But it involves work on our part, and being prepared for hard decisions.
- What is most important to us, and what tradeoffs are we willing to make for it?
- What, even, is actually an option to us with the resources available?
- Can we make peace with a potentially bad lot? And… Should we?
- When is fighting important, and when is it self-destructive?
These (and others) are all difficult questions posed by Dr. Gawande, but critical ones.
We don’t usually quote other people’s reviews when reviewing books here, but let’s consider the following words from the end of a long review on Amazon:
❝If “dying as we lived” is some kind of standard for how we should go, then maybe alone and medicalized makes some sense right now after all.❞
Bottom line: we all deserve better than that. And if we don’t take the time to think about what’s most important, then time will take it from us. This very insightful book may not have all the answers, but it has the questions, and it can help a lot in exploring them and deciding what matters most to us in the end, really.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Clean Your Brain (Glymphatic Health Primer)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
That’s not a typo! The name “glymphatic system” was coined by the Danish neuroscientist Dr. Maiken Nedergaard, and is a nod to its use of glial cells to do a similar job to that of the peripheral lymphatic system—but this time, in the CNS. Today, we have Dr. Jin Sung to tell us more:
Brainwashing (but not like that)
The glymphatic system may sound like a boring job, but so does “sanitation worker” in a city—yet the city would grind to a messy halt very very quickly without them. Same goes for your brain.
Diseases that are prevalent when this doesn’t happen the way it should include Alzheimer’s (beta-amyloid clearance) and Parkinson’s (alpha-synuclein clearance) amongst others.
Things Dr. Sung recommends for optimal glymphatic function include: sleep (7–9 hours), exercise (30–45 minutes daily), hydration (half your bodyweight in pounds, in ounces, so if your body weighs 150 lbs, that means 75 oz of water), good posture (including the use of good ergonomics, e.g. computer monitor at right height, car seat correct, etc), stress reduction (reduces inflammatory cytokines), getting enough omega-3 (the brain needs certain fats to work properly, and this is the one most likely to see a deficit), vagal stimulation (methods include humming, gargling, and gagging—please note we said vagal stimulation; easy to misread at a glance!), LED light therapy, and fasting (intermittent or prolonged).
For more on each of these, including specific tips, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Ask Not What Your Lymphatic System Can Do For You…
- The Vagus Nerve (And How You Can Make Use Of It)
- Casting Yourself In A Healthier Light
- Intermittent Fasting: How Does It Work?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Osteoporosis Breakthrough – by Dr. Doug Lucas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Osteoporosis” and “break” often don’t go well together, but here they do. So, what’s the breakthrough here?
There isn’t one, honestly. But if we overlook the marketing choices and focus on the book itself, the content here is genuinely good:
The book offers a comprehensive multivector approach to combatting osteoporosis, e.g:
- Diet
- Exercise
- Other lifestyle considerations
- Supplements
- Hormones
- Drugs
The author considers drugs a good and important tool for some people with osteoporosis, but not most. The majority of people, he considers, will do better without drugs—by tackling things more holistically.
The advice here is sound and covers all reasonable angles without getting hung up on the idea of there being a single magical solution for all.
Bottom line: if you’re looking for a book that’s a one-stop-shop for strategies against osteoporosis, this is a good option.
Click here to check out The Osteoporosis Breakthrough, and keep your bones strong!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: