The Meds That Impair Decision-Making
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Impairment to cognitive function is often comorbid with Parkinson’s disease. That is to say: it’s not a symptom of Parkinson’s, but it often occurs in the same people. This may seem natural: after all, both are strongly associated with aging.
However, recent (last month, at time of writing) research has brought to light a very specific way in which medication for Parkinson’s may impair the ability to make sound decisions.
Obviously, this is a big deal, because it can affect healthcare decisions, financial decisions, and more—greatly impacting quality of life.
See also: Age-related differences in financial decision-making and social influence
(in which older people were found more likely to be influenced by the impulsive financial preferences of others than their younger counterparts, when other factors are controlled for)
As for how this pans out when it comes to Parkinson’s meds…
Pramipexole (PPX)
This drug can, due to an overlap in molecular shape, mimic dopamine in the brains of people who don’t have enough—such as those with Parkinson’s disease. This (as you might expect) helps alleviate Parkinson’s symptoms.
However, researchers found that mice treated with PPX and given a touch-screen based gambling game picked the high-risk, high reward option much more often. In the hopes of winning strawberry milkshake (the reward), they got themselves subjected to a lot of blindingly-bright flashing lights (the risk, to which untreated mice were much more averse, as this is very stressful for a mouse).
You may be wondering: did the mice have Parkinson’s?
The answer: kind of; they had been subjected to injections with 6-hydroxydopamine, which damages dopamine-producing neurons similarly to Parkinson’s.
This result was somewhat surprising, because one would expect that a mouse whose depleted dopamine was being mimicked by a stand-in (thus, doing much of the job of dopamine) would be less swayed by the allure of gambling (a high-dopamine activity), since gambling is typically most attractive to those who are desperate to find a crumb of dopamine somewhere.
They did find out why this happened, by the way, the PPX hyperactivated the external globus pallidus (also called GPe, and notwithstanding the name, this is located deep inside the brain). Chemically inhibiting this area of the brain reduced the risk-taking activity of the mice.
This has important implications for Parkinson’s patients, because:
- on an individual level, it means this is a side effect of PPX to be aware of
- on a research-and-development level, it means drugs need to be developed that specifically target the GPe, to avoid/mitigate this side effect.
You can read the study in full here:
Don’t want to get Parkinson’s in the first place?
While nothing is a magic bullet, there are things that can greatly increase or decrease Parkinson’s risk. Here’s a big one, as found recently (last week, at the time of writing):
Air Pollution and Parkinson’s Disease in a Population-Based Study
Also: knowing about its onset sooner rather than later is scary, but beneficial. So, with that in mind…
Recognize The Early Symptoms Of Parkinson’s Disease
Finally, because Parkinson’s disease is theorized to be caused by a dysfunction of alpha-synuclein clearance (much like the dysfunction of beta-amyloid clearance, in the case of Alzheimer’s disease), this means that having a healthy glymphatic system (glial cells doing the same clean-up job as the lymphatic system, but in the brain) is critical:
How To Clean Your Brain (Glymphatic Health Primer)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Rise And (Really) Shine!

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Q&A with 10almonds Subscribers!
Q: Would love to hear more ideas about effective first thing in the morning time management to get a great start on your day.
A: There are a lot of schools of thought about what’s best in this regard! Maybe we’ll do a main feature sometime. But some things that are almost universally agreed upon are:
- Prepare your to-do list the night before
- Have some sort of buffer between waking up and getting to productivity.
- For me (hi, your writer here) it’s my first coffee of the day. It’s not even about the caffeine, it’s about the ritual of it, it’s a marker that separates my night from the day and tells my brain what gear to get into.
- Others may like to exercise first thing in the morning
- For still yet others, it could be a shower, cold or otherwise
- Some people like a tall glass of lemon water to rehydrate after sleeping!
- If you take drinkable morning supplements such as this pretty awesome nootropic stack, it’s a great time for that and an excellent way to get the brain-juices flowing!
- When you do get to productivity: eat the frog first! What this means is: if eating a frog is the hardest thing you’ll have to do all day, do that first. Basically, tackle the most intimidating task first. That way, you won’t spend your day stressed/anxious and/or subconsciously wasting time in order to procrastinate and avoid it.
- Counterpart to the above: a great idea is to also plan something to look forward to when your working day is done. It doesn’t matter much what it is, provided it’s rewarding to you, that makes you keen to finish your tasks to get to it.
Have a question you’d like to see answered here? Hit reply to this email, or use the feedback widget at the bottom! We always love to hear from you
Share This Post
-

Do We Simply Not Care About Old People?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The covid-19 pandemic would be a wake-up call for America, advocates for the elderly predicted: incontrovertible proof that the nation wasn’t doing enough to care for vulnerable older adults.
The death toll was shocking, as were reports of chaos in nursing homes and seniors suffering from isolation, depression, untreated illness, and neglect. Around 900,000 older adults have died of covid-19 to date, accounting for 3 of every 4 Americans who have perished in the pandemic.
But decisive actions that advocates had hoped for haven’t materialized. Today, most people — and government officials — appear to accept covid as a part of ordinary life. Many seniors at high risk aren’t getting antiviral therapies for covid, and most older adults in nursing homes aren’t getting updated vaccines. Efforts to strengthen care quality in nursing homes and assisted living centers have stalled amid debate over costs and the availability of staff. And only a small percentage of people are masking or taking other precautions in public despite a new wave of covid, flu, and respiratory syncytial virus infections hospitalizing and killing seniors.
In the last week of 2023 and the first two weeks of 2024 alone, 4,810 people 65 and older lost their lives to covid — a group that would fill more than 10 large airliners — according to data provided by the CDC. But the alarm that would attend plane crashes is notably absent. (During the same period, the flu killed an additional 1,201 seniors, and RSV killed 126.)
“It boggles my mind that there isn’t more outrage,” said Alice Bonner, 66, senior adviser for aging at the Institute for Healthcare Improvement. “I’m at the point where I want to say, ‘What the heck? Why aren’t people responding and doing more for older adults?’”
It’s a good question. Do we simply not care?
I put this big-picture question, which rarely gets asked amid debates over budgets and policies, to health care professionals, researchers, and policymakers who are older themselves and have spent many years working in the aging field. Here are some of their responses.
The pandemic made things worse. Prejudice against older adults is nothing new, but “it feels more intense, more hostile” now than previously, said Karl Pillemer, 69, a professor of psychology and gerontology at Cornell University.
“I think the pandemic helped reinforce images of older people as sick, frail, and isolated — as people who aren’t like the rest of us,” he said. “And human nature being what it is, we tend to like people who are similar to us and be less well disposed to ‘the others.’”
“A lot of us felt isolated and threatened during the pandemic. It made us sit there and think, ‘What I really care about is protecting myself, my wife, my brother, my kids, and screw everybody else,’” said W. Andrew Achenbaum, 76, the author of nine books on aging and a professor emeritus at Texas Medical Center in Houston.
In an environment of “us against them,” where everybody wants to blame somebody, Achenbaum continued, “who’s expendable? Older people who aren’t seen as productive, who consume resources believed to be in short supply. It’s really hard to give old people their due when you’re terrified about your own existence.”
Although covid continues to circulate, disproportionately affecting older adults, “people now think the crisis is over, and we have a deep desire to return to normal,” said Edwin Walker, 67, who leads the Administration on Aging at the Department of Health and Human Services. He spoke as an individual, not a government representative.
The upshot is “we didn’t learn the lessons we should have,” and the ageism that surfaced during the pandemic hasn’t abated, he observed.
Ageism is pervasive. “Everyone loves their own parents. But as a society, we don’t value older adults or the people who care for them,” said Robert Kramer, 74, co-founder and strategic adviser at the National Investment Center for Seniors Housing & Care.
Kramer thinks boomers are reaping what they have sown. “We have chased youth and glorified youth. When you spend billions of dollars trying to stay young, look young, act young, you build in an automatic fear and prejudice of the opposite.”
Combine the fear of diminishment, decline, and death that can accompany growing older with the trauma and fear that arose during the pandemic, and “I think covid has pushed us back in whatever progress we were making in addressing the needs of our rapidly aging society. It has further stigmatized aging,” said John Rowe, 79, professor of health policy and aging at Columbia University’s Mailman School of Public Health.
“The message to older adults is: ‘Your time has passed, give up your seat at the table, stop consuming resources, fall in line,’” said Anne Montgomery, 65, a health policy expert at the National Committee to Preserve Social Security and Medicare. She believes, however, that baby boomers can “rewrite and flip that script if we want to and if we work to change systems that embody the values of a deeply ageist society.”
Integration, not separation, is needed. The best way to overcome stigma is “to get to know the people you are stigmatizing,” said G. Allen Power, 70, a geriatrician and the chair in aging and dementia innovation at the Schlegel-University of Waterloo Research Institute for Aging in Canada. “But we separate ourselves from older people so we don’t have to think about our own aging and our own mortality.”
The solution: “We have to find ways to better integrate older adults in the community as opposed to moving them to campuses where they are apart from the rest of us,” Power said. “We need to stop seeing older people only through the lens of what services they might need and think instead of all they have to offer society.”
That point is a core precept of the National Academy of Medicine’s 2022 report Global Roadmap for Healthy Longevity. Older people are a “natural resource” who “make substantial contributions to their families and communities,” the report’s authors write in introducing their findings.
Those contributions include financial support to families, caregiving assistance, volunteering, and ongoing participation in the workforce, among other things.
“When older people thrive, all people thrive,” the report concludes.
Future generations will get their turn. That’s a message Kramer conveys in classes he teaches at the University of Southern California, Cornell, and other institutions. “You have far more at stake in changing the way we approach aging than I do,” he tells his students. “You are far more likely, statistically, to live past 100 than I am. If you don’t change society’s attitudes about aging, you will be condemned to lead the last third of your life in social, economic, and cultural irrelevance.”
As for himself and the baby boom generation, Kramer thinks it’s “too late” to effect the meaningful changes he hopes the future will bring.
“I suspect things for people in my generation could get a lot worse in the years ahead,” Pillemer said. “People are greatly underestimating what the cost of caring for the older population is going to be over the next 10 to 20 years, and I think that’s going to cause increased conflict.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
USE OUR CONTENT
This story can be republished for free (details).
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

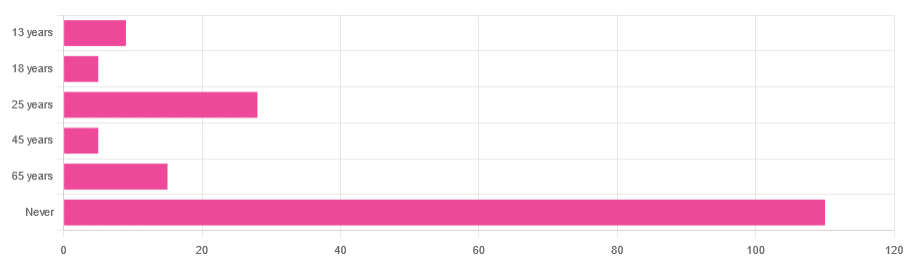
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Share This Post
-

Are You Taking PIMs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Getting Off The Overmedication Train
The older we get, the more likely we are to be on more medications. It’s easy to assume that this is because, much like the ailments they treat, we accumulate them over time. And superficially at least, that’s what happens.
And yet, almost half of people over 65 in Canada are taking “potentially inappropriate medications”, or PIMs—in other words, medications that are not needed and perhaps harmful. This categorization includes medications where the iatrogenic harms (side effects, risks) outweigh the benefits, and/or there’s a safer more effective medication available to do the job.
You may be wondering: what does this mean for the US?
Well, we don’t have the figures for the US because we’re working from Canadian research today, but given the differences between the two country’s healthcare systems (mostly socialized in Canada and mostly private in the US), it seems a fair hypothesis that if it’s almost half in Canada, it’s probably more than half in the US. Socialized healthcare systems are generally quite thrifty and seek to spend less on healthcare, while private healthcare systems are generally keen to upsell to new products/services.
The three top categories of PIMs according to the above study:
- Gabapentinoids (anticonvulsants also used to treat neuropathic pain)
- Proton pump inhibitors (PPIs)
- Antipsychotics (especially, to people without psychosis)
…but those are just the top of the list; there are many many more.
The list continues: opioids, anticholinergics, sulfonlyurea, NSAIDs, benzodiazepines and related rugs, and cholinesterase inhibitors. That’s where the Canadian study cuts off (although it also includes “others” just before NSAIDs), but still, you guessed it, there are more (we’re willing to bet statins weigh heavily in the “others” section, for a start).
There are two likely main causes of overmedication:
The side effect train
This is where a patient has a condition and is prescribed drug A, which has some undesired side effects, so the patient is prescribed drug B to treat those. However, that drug also has some unwanted side effects of its own, so the patient is prescribed drug C to treat those. And so on.
For a real-life rundown of how this can play out, check out the case study in:
The Hidden Complexities of Statins and Cardiovascular Disease (CVD)
The convenience factor
No, not convenient for you. Convenient for others. Convenient for the doctor if it gets you out of their office (socialized healthcare) or because it was easy to sell (private healthcare). Convenient for the staff in a hospital or other care facility.
This latter is what happens when, for example, a patient is being too much trouble, so the staff give them promazine “to help them settle down”, notwithstanding that promazine is, besides being a sedative, also an antipsychotic whose common side effects include amenorrhea, arrhythmias, constipation, drowsiness and dizziness, dry mouth, impotence, tiredness, galactorrhoea, gynecomastia, hyperglycemia, insomnia, hypotension, seizures, tremor, vomiting and weight gain.
This kind of thing (and worse) happens more often towards the end of a patient’s life; indeed, sometimes precipitating that end, whether you want it or not:
Mortality, Palliative Care, & Euthanasia
How to avoid it
Good practice is to be “open-mindedly skeptical” about any medication. By this we mean, don’t reject it out of hand, but do ask questions about it.
Ask your prescriber not only what it’s for and what it’ll do, but also what the side effects and risks are, and an important question that many people don’t think to ask, and for which doctors thus don’t often have a well-prepared smooth-selling reply, “what will happen if I don’t take this?”
And look up unbiased neutral information about it, from reliable sources (Drugs.com and The BNF are good reference guides for this—and if it’s important to you, check both, in case of any disagreement, as they function under completely different regulatory bodies, the former being American and the latter being British. So if they both agree, it’s surely accurate, according to best current science).
Also: when you are on a medication, keep a journal of your symptoms, as well as a log of your vitals (heart rate, blood pressure, weight, sleep etc) so you know what the medication seems to be helping or harming, and be sure to have a regular meds review with your doctor to check everything’s still right for you. And don’t be afraid to seek a second opinion if you still have doubts.
Want to know more?
For a more in-depth exploration than we have room for here, check out this book that we reviewed not long back:
To Medicate or Not? That is the Question! – by Dr. Asha Bohannon
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
4 ways to cut down on meat when dining out – and still make healthy choices
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us are looking for ways to eat a healthier and more sustainable diet. And one way to do this is by reducing the amount of meat we eat.
That doesn’t mean you need to become a vegan or vegetarian. Our recent research shows even small changes to cut down on meat consumption could help improve health and wellbeing.
But not all plant-based options are created equal and some are ultra-processed. Navigating what’s available when eating out – including options like tofu and fake meats – can be a challenge.
So what are your best options at a cafe or restaurant? Here are some guiding principles to keep in mind when cutting down on meat.

Mikhaylovskiy/Shutterstock Health benefits to cutting down
Small amounts of lean meat can be part of a healthy, balanced diet. But the majority of Australians still eat more meat than recommended.
Only a small percentage of Australians (10%) are vegetarian or vegan. But an increasing number opt for a flexitarian diet. Flexitarians eat a diet rich in fruits and vegetables, while still enjoying small amounts of meat, dairy, eggs and fish.
Our recent research looked at whether the average Australian diet would improve if we swapped meat and dairy for plant-based alternatives, and the results were promising.
The study found health benefits when people halved the amount of meat and dairy they ate and replaced them with healthy plant-based foods, like tofu or legumes. On average, their dietary fibre intake – which helps with feeling fuller for longer and digestive health – went up. Saturated fats – which increase our blood cholesterol levels, a risk factor for heart disease – went down.
Including more fibre and less saturated fat helps reduce the risk of heart disease.
Achieving these health benefits may be as simple as swapping ham for baked beans in a toastie for lunch, or substituting half of the mince in your bolognese for lentils at dinner.
Filling your plate with fibre-rich foods can help lower cholesterol. Wally Pruss/Shutterstock How it’s made matters
For a long time we’ve known processed meats – such as ham, bacon and sausages – are bad for your health. Eating high amounts of these foods is associated with poor heart health and some forms of cancer.
But the same can be true of many processed meat alternatives.
Plant-based alternatives designed to mimic meat, such as sausages and burgers, have become readily available in supermarkets, cafes and restaurants. These products are ultra-processed and can be high in salt and saturated fat.
Our study found when people replaced meat and dairy with ultra-processed meat alternatives – such as plant-based burgers or sausages – they ate more salt and less calcium, compared to eating meat or healthy plant-based options.
So if you’re cutting down on meat for health reasons, it’s important to think about what you’re replacing it with. The Australian Dietary Guidelines recommend eggs, legumes/beans, tofu, nuts and seeds.
Tofu can be a great option. But we recommend flavouring plain tofu with herbs and spices yourself, as pre-marinated products are often ultra-processed and can be high in salt.
What about when dining out?
When you’re making your own food, it’s easier to adapt recipes or reduce the amount of meat. But when faced with a menu, it can be difficult to work out what is the best option.
Eating a range of colours is one way to ensure variety. Mikhail Nilov/Pexels Here are our four ways to make healthy choices when you eat out:
1. Fill half your plate with vegetables
When cutting down on meat, aim for half your plate to be vegetables. Try to also eat a variety of colours, such as leafy green spinach, red capsicum and pumpkin.
When you’re out, this might look like choosing a vegetable-based entree, a stir-fry or ordering a side salad to have with your meal.
2. Avoid the deep fryer
The Australian Dietary Guidelines recommend limiting deep fried foods to once a week or less. When dining out, choose plant-based options that are sautéed, grilled, baked, steamed, boiled or poached – instead of those that are crumbed or battered before deep frying.
This could mean choosing vegetarian dumplings that are steamed not fried, or poached eggs at brunch instead of fried. Ordering a side of roast vegetables instead of hot chips is also a great option.
3. Pick wholegrains
Scan the menu for wholegrain options such as brown rice, wholemeal pizza or pasta, barley, quinoa or wholemeal burger buns. Not only are they good sources of protein, but they also provide more dietary fibre than refined grains, which help keep you fuller for longer.
4. If you do pick meat – choose less processed kinds
You may not always want, or be able, to make a vegetarian choice when eating out and with other people. If you do opt for meat, it’s better to steer clear of processed options like bacon or sausages.
If sharing dishes with other people, you could try adding unprocessed plant-based options into the mix. For example, a curry with lentils or chickpeas, or a vegetable-based pizza instead of one with ham or salami. If that’s not an option, try choose meat that’s a lean cut, such as chicken breast, or options which are grilled rather than fried.
Laura Marchese, PhD candidate at the Institute for Physical Activity and Nutrition, Deakin University and Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

See what other 10almonds subscribers are asking!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Q: I would be interested in learning more about collagen and especially collagen supplements/powders and of course if needed, what is the best collagen product to take. What is collagen? Why do we need to supplement the collagen in our body? Thank you PS love the information I am receiving in the news letters. Keep it up
We’re glad you’re enjoying them! Your request prompted us to do our recent Research Review Monday main feature on collagen supplementation—we hope it helped, and if you’ve any more specific (or other) question, go ahead and let us know! We love questions and requests
Q: Great article about the health risks of salt to organs other than the heart! Is pink Himalayan sea salt, the pink kind, healthier?
Thank you! And, no, sorry. Any salt that is sodium chloride has the exact same effect because it’s chemically the same substance, even if impurities (however pretty) make it look different.
If you want a lower-sodium salt, we recommend the kind that says “low sodium” or “reduced sodium” or similar. Check the ingredients, it’ll probably be sodium chloride cut with potassium chloride. Potassium chloride is not only not a source of sodium, but also, it’s a source of potassium, which (unlike sodium) most of us could stand to get a little more of.
For your convenience: here’s an example on Amazon!
Bonus: you can get a reduced sodium version of pink Himalayan salt too!
Q: Can you let us know about more studies that have been done on statins? Are they really worth taking?
That is a great question! We imagine it might have been our recent book recommendation that prompted it? It’s quite a broad question though, so we’ll do that as a main feature in the near future!
Q: Is MSG healthier than salt in terms of sodium content or is it the same or worse?
Great question, and for that matter, MSG itself is a great topic for another day. But your actual question, we can readily answer here and now:
- Firstly, by “salt” we’re assuming from context that you mean sodium chloride.
- Both salt and MSG do contain sodium. However…
- MSG contains only about a third of the sodium that salt does, gram-for-gram.
- It’s still wise to be mindful of it, though. Same with sodium in other ingredients!
- Baking soda contains about twice as much sodium, gram for gram, as MSG.
Wondering why this happens?
Salt (sodium chloride, NaCl) is equal parts sodium and chlorine, by atom count, but sodium’s atomic mass is lower than chlorine’s, so 100g of salt contains only 39.34g of sodium.
Baking soda (sodium bicarbonate, NaHCO₃) is one part sodium for one part hydrogen, one part carbon, and three parts oxygen. Taking each of their diverse atomic masses into account, we see that 100g of baking soda contains 27.4g sodium.
MSG (monosodium glutamate, C₅H₈NO₄Na) is only one part sodium for 5 parts carbon, 8 parts hydrogen, 1 part nitrogen, and 4 parts oxygen… And all those other atoms put together weigh a lot (comparatively), so 100g of MSG contains only 12.28g sodium.
Q: Thanks for the info about dairy. As a vegan, I look forward to a future comment about milk alternatives
Thanks for bringing it up! What we research and write about is heavily driven by subscriber feedback, so notes like this really help us know there’s an audience for a given topic!
We’ll do a main feature on it, to do it justice. Watch out for Research Review Monday!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: