What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.

Let’s start with some definitions
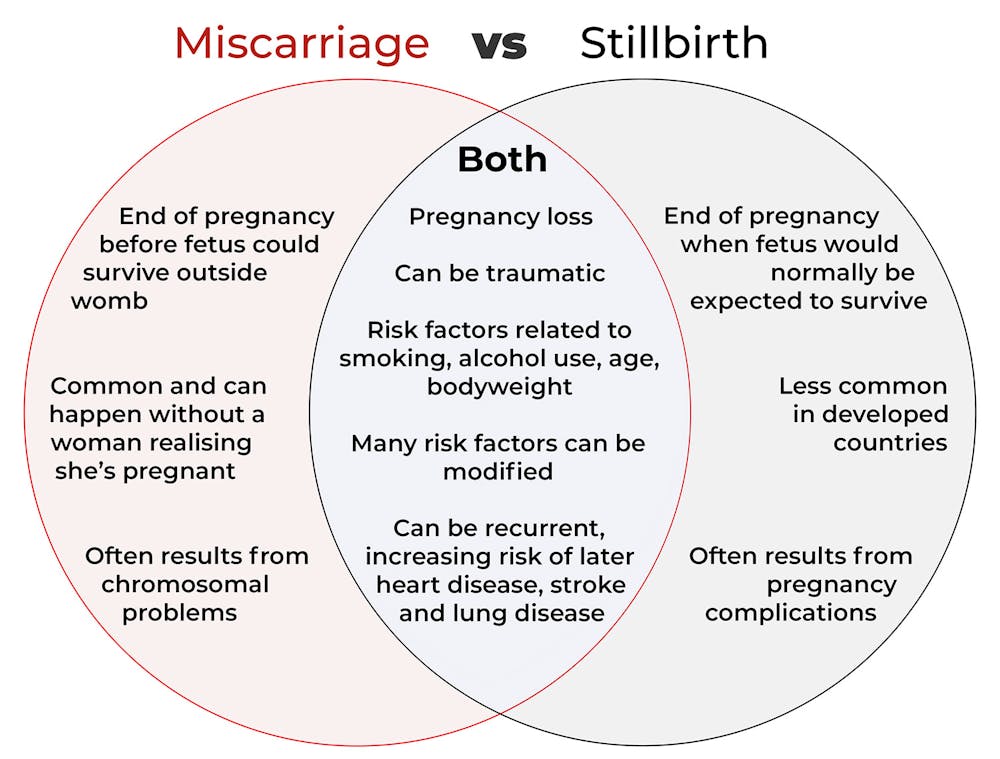
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.

Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.

Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is reformer pilates? And is it worth the cost?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Reformer pilates is steadily growing in popularity, with new studios opening regularly in major cities all over the world.
But what exactly is reformer pilates? And how does it compare with regular pilates and other types of exercise?
Classes aren’t cheap so let’s look at the potential benefits and drawbacks to help you decide if it’s right for you.

Ahmet Kurt/Unsplash Pilates with special equipment
Pilates is a mode of exercise that focuses on core stability and flexibility, while also addressing muscular strength and endurance, balance and general fitness. At first glance, it might look a bit like yoga, with some more traditional weight training components thrown in.
Reformer pilates uses a piece of equipment called a “reformer”. This looks like a narrow bed that slides along a carriage, has straps to hold onto, and has adjustable springs that add resistance to movement. You perform pilates on the reformer to target specific muscle groups and movement patterns.
The reformer was first designed to help people recover from injuries. However, it has now become common for general fitness and even sports performance.
Unlike normal pilates, also known as “mat pilates”, which only uses your body weight, the reformer adds resistance, meaning you can change the difficulty according to your current level of fitness.
This not only provides a way to overload your muscles, but can make the exercise session more aerobically demanding, which has been proposed to improve cardiovascular fitness.
Mat pilates uses your body weight. Kampus Productions/Pexels What are the benefits of reformer pilates?
Despite being around for decades, there is surprisingly little research looking at the benefits of reformer pilates. However, what we have seen so far suggests it has a similar effect to other modes of exercise.
Reformer pilates has been shown to help with weight loss, cause some small increases in muscle mass, and enhance cognitive function. All of these benefits are commonly seen when combining weight training and cardio into the same routine.
Similarly, among older adults, it has been shown to improve strength, enhance flexibility and may even reduce the risk of falling.
From a rehabilitation perspective, there is some evidence indicating reformer pilates can improve shoulder health and function, reduce lower back pain and increase flexibility.
Finally, there is some evidence suggesting a single session of reformer pilates can improve two key markers of cardiovascular health, being flow-mediated dilation and pulse wave velocity, while also improving cholesterol and insulin levels. This suggests reformer pilates could lead to long-term improvements in heart and metabolic health, although more research is needed to confirm this.
Reformer pilates was first designed to help people recover from injuries. Kampus Productions/Pexels However, there are some key things to consider when discussing these benefits. Most of this research is quite exploratory and comes from a very small number of studies. So we do not know whether these findings will apply to everyone.
Very few studies compared reformer pilates to other types of exercise. Therefore, while it can improve most aspects of health and function, it’s unlikely reformer pilates provides the optimal mode of exercise for each individual component of physical fitness.
Traditional weight training, for example, will likely cause larger improvements in strength than reformer pilates. Similarly, stretching will probably make you more flexible. And running or cycling will make you fitter.
However, if you want a type of exercise that gives you broad overall health benefits, it could be a good option.
What are the downsides of reformer pilates
Reformer pilates is not for everyone.
First and foremost, classes can be expensive compared to other fitness options. You need to be doing at least two to three sessions per week of any type of exercise to maximise the benefits. So even if you can find a class for A$20 or $30, paying for two or three classes a week (or buying a weekly or monthly subscription) is a significant outlay.
Second, it’s not as accessible as other exercise. Even if you can afford it, not every town or suburb has a reformer pilates studio.
Cost and access are major barriers. Or you might get better results with specific modes of exercises. Karolina Grabowska/Pexels Third, the effectiveness of your workout is likely to be impacted by how competent your instructor is. There are a host of different pilates qualifications you can get in Australia, and some take much less time than others. With this in mind, it might be best to look for accredited pilates instructors, although this will further reduce the number of options you have available.
Finally, there is a learning curve. While you will get better over time, the exercise will likely be less effective during those first few weeks (or months) when you are getting used to the machine and the movements.
Is it right for you?
Reformer pilates can be a great addition to your fitness routine, especially if you’re looking for a low-impact way to build strength and flexibility.
But if you have more specific goals, you might need a more specific mode of exercise. For example, if you need to get stronger to improve your ability to manage your daily life, then strength training is probably your best bet. Likewise, if your goal is to run a marathon, you will get more specific benefits from running.
The cost and availability of reformer pilates make it less accessible for some people. With this in mind, if you are after similar benefits at a lower price point, mat pilates might be a better option. Not only does it have evidence suggesting it can improve strength and fitness, but it is something you can do at home if you find a good resource (YouTube could be a good starting point here).
Hunter Bennett, Lecturer in Exercise Science, University of South Australia; Jacinta Brinsley, Exercise Physiologist and Postdoctoral Researcher in the Alliance for Research in Nutrition, Exercise and Activity, University of South Australia, and Lewis Ingram, Lecturer in Physiotherapy, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Ghanaian Red Bean & Sweet Potato Groundnut Stew
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a dish popular in principle throughout West Africa. We say “in principle” because that’s a big place, and there is a lot of regional variation. The archetypal peanut stew is from Senegal (as maafe) or Mali (as tigadèguèna), but for its more balanced nutritional profile we’ve chosen one from Ghana—and since there are regional variations within Ghana too, we should specify that this one is from the south.
If you are allergic to nuts, you can substitute a seed butter (or tahini) for the nut butter, and omit the nuts—this will work in culinary terms and be fine healthwise, but we can’t claim it would be the same dish, having lost its defining ingredient. If your allergy is solely to peanuts, then substituting with any oily nut would work. So, not almonds for example, but cashews or even walnuts would be fine.
You will need
- 1½ lbs sweet potatoes, peeled and cut into ½” cubes
- 2 cups low-sodium vegetable stock
- 2 cans kidney beans, drained, cooked, and rinsed (or 2 cups same; cooked, drained, and rinsed)
- 1 can chopped tomatoes
- ½ cup unsalted dry-roasted peanuts
- 1 onion, chopped
- 1 red bell pepper, deseeded and chopped
- ¼ bulb garlic, finely chopped
- 2 heaped tbsp unsalted peanut butter, minimal (ideally: no) additives
- 2 tsp white miso paste
- 2 tsp grated fresh ginger
- 1 tsp ground cumin
- 1 tsp cayenne pepper
- 1 tsp black pepper
- ½ tsp MSG or 1 tsp low-sodium salt
- ½ tsp coarsely ground nigella seeds
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Heat some oil in a sauté pan, or other pan suitable for both frying and fitting the entire stew in. Fry the onions until softened, turn the heat down low, and add the garlic, ginger, red bell pepper, cumin, cayenne, black pepper, and MSG/salt.
2) Add ¼ cup of the vegetable stock, and the sweet potato, and turn the heat back up, on high for about 30 seconds to get it to temperature, and then take it down to a simmer.
3) Stir in the miso paste and chopped tomatoes.
4) Add most of the rest of the vegetable stock, keeping ¼ cup aside. Simmer for about 20 minutes.
5) Stir in the kidney beans, and simmer for about 30 minutes more—the sweet potato should be soft now; if it isn’t, let it simmer a while longer until it is.
6) Combine the peanut butter with the remaining ¼ cup vegetable stock, and blend until smooth. Stir it into the stew.
7) If the stew is looking more like a soup than a stew, take out 1 cup and blend this 1 cup to a purée, adding it back in.
8) Add half the peanuts unto the stew. Taste, and adjust the seasonings if necessary.
9) Crush the remaining peanuts using a pestle and mortar; not too much though; you want them broken into bits, not pulverised.
10) Garnish with the crushed nuts and nigella seeds, and serve.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Eat More (Of This) For Lower Blood Pressure
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Our Top 5 Spices: How Much Is Enough For Benefits? ← we used 4/5 today!
Take care!
Share This Post
-

Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?

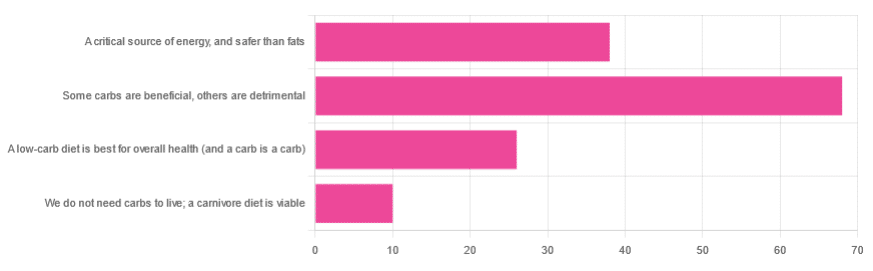
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Share This Post





-
What Do The Different Kinds Of Fiber Do? 30 Foods That Rank Highest
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve talked before about how important fiber is:
Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
And even how it’s arguably the most important dietary factor when it comes to avoiding heart disease:
What Matters Most For Your Heart? Eat More (Of This) For Lower Blood Pressure ← Spoiler: it’s fiber
And yes, that’s even when considered alongside other (also laudable) dietary interventions such as lowering intake of sodium, various kinds of saturated fat, and red meat.
So, what should we know about fiber, aside from “aim to get nearer 40g/day instead of the US average 16g/day”?
Soluble vs Insoluble
The first main way that dietary fibers can be categorized is soluble vs insoluble. Part of the difference is obvious, but bear with us, because there’s more to know about each:
- Soluble fiber dissolves (what a surprise) in water and, which part is important, forms a gel. This slows down things going through your intestines, which is important for proper digestion and absorption of nutrients (as well as avoiding diarrhea). Yes, you heard right: getting enough of the right kind of fiber helps you avoid diarrhea.
- Insoluble fiber does not dissolve (how shocking) in water and thus mostly passes through undigested by us (some will actually be digested by gut microbes who subsist on this, and in return for us feeding them daily, they make useful chemicals for us). This kind of fiber is also critical for healthy bowel movements, because without it, constipation can ensue.
Both kinds of fiber improve just about every metric related to blood, including improving triglycerides and improving insulin sensitivity and blood glucose levels. Thus, they help guard against various kinds of cardiovascular disease, diabetes, and metabolic disease in general. Do note that because whatever’s good for your heart/blood is good for your brain (which requires a healthy heart and bloodstream to nourish it and take away waste), likely this also has a knock-on effect against cognitive decline, but we don’t have hard science for that claim so we’re going to leave that last item as a “likely”.
However, one thing’s for sure: if you want a healthy gut, heart, and brain, you need a good balance of soluble and insoluble fibers.
10 of the best for soluble fiber
Food Soluble Fiber Type(s) Soluble Fiber (g per serving) Insoluble Fiber Type(s) Insoluble Fiber (g per serving) Total Fiber (g per serving) Kidney beans (1 cup cooked) Pectin, Resistant Starch 1.5–2 Hemicellulose, Cellulose 6 8 Lentils (1 cup cooked) Pectin, Resistant Starch 1.5–2 Cellulose 6 7.5 Barley (1 cup cooked) Beta-glucan 3–4 Hemicellulose 2 6 Brussels sprouts (1 cup cooked) Pectin 1–1.5 Cellulose, Hemicellulose 2 3.5 Oats (1 cup cooked) Beta-glucan 2–3 Cellulose 1 3 Apples (1 medium) Pectin 1–2 Cellulose, Hemicellulose 2 3 Carrots (1 cup raw) Pectin 1–1.5 Cellulose, Hemicellulose 2 3 Citrus fruits (orange, 1 medium) Pectin 1–1.5 Cellulose 1 2.5 Flaxseeds (2 tbsp) Mucilage, Lignin 1–1.5 Cellulose 1 2.5 Psyllium husk (1 tbsp) Mucilage 3–4 Trace amounts 0 3–4 10 of the best for insoluble fiber
Food Soluble Fiber Type(s) Soluble Fiber (g per serving) Insoluble Fiber Type(s) Insoluble Fiber (g per serving) Total Fiber (g per serving) Wheat bran (1 cup) Trace amounts 0 Cellulose, Lignin 6–8 6–8 Black beans (1 cup cooked) Pectin, Resistant Starch 1.5 Cellulose 6 7.5 Brown rice (1 cup cooked) Trace amounts 0.5 Hemicellulose, Lignin 2–3 2.5–3.5 Popcorn (3 cups popped) Trace amounts 0.5 Hemicellulose 3 3.5 Broccoli (1 cup cooked) Pectin 1 Cellulose, Hemicellulose 4 5 Green beans (1 cup cooked) Trace amounts 0.5 Cellulose, Hemicellulose 3 3.5 Sweet potatoes (1 cup cooked) Pectin 1–1.5 Cellulose 3 4.5 Whole wheat bread (1 slice) Trace amounts 0.5 Cellulose, Hemicellulose 1 1.5 Pears (1 medium) Pectin 1 Cellulose, Hemicellulose 4 5 Almonds (1 oz) Trace amounts 0.5 Cellulose, Hemicellulose 2 2.5 10 of the best for a balance of both
Food Soluble Fiber Type(s) Soluble Fiber (g per serving) Insoluble Fiber Type(s) Insoluble Fiber (g per serving) Total Fiber (g per serving) Raspberries (1 cup) Pectin 1 Cellulose 5 6 Edamame (1 cup cooked) Pectin 1 Cellulose 5 6 Chia seeds (2 tbsp) Mucilage, Pectin 2–3 Lignin, Cellulose 3 5.5 Artichokes (1 medium) Inulin 1 Cellulose, Hemicellulose 5 6 Avocado (1 medium) Pectin ~2 Cellulose 4 6 Black beans (1 cup cooked) Pectin, Resistant Starch 1.5 Cellulose 6 7.5 Quinoa (1 cup cooked) Pectin, Saponins 1 Cellulose, Hemicellulose 3 4 Spinach (1 cup cooked) Pectin 0.5 Cellulose, Lignin 3 3.5 Prunes (1/2 cup) Pectin, Sorbitol 2 Cellulose 4 6 Figs (3 medium) Pectin 1 Cellulose 2 3 You’ll notice that the above “balance” is not equal; that’s ok; we need greater quantities of insoluble than soluble anyway, so it is as well that nature provides such.
This is the same kind of balance when we talk about “balanced hormones” (does not mean all hormones are in equal amounts; means they are in the right proportions) or “balanced microbiome” (does not mean that pathogens and friendly bacteria are in equal numbers), etc.
Some notes on the above:
About those fiber types, some of the most important soluble ones to aim for are:
- Beta-glucan: found in oats and barley, it supports heart health.
- Pectin: found in fruits like apples, citrus, and pears, it helps with cholesterol control.
- Inulin: a type of prebiotic fiber found in artichokes.
- Lignin: found in seeds and wheat bran, it has antioxidant properties.
- Resistant starch: found in beans and lentils, it acts as a prebiotic for gut health.
See also: When Is A Fiber Not A Fiber? The Food Additive You Do Want
One fiber to rule them all
Well, not entirely (we still need the others) but there is a best all-rounder:
The Best Kind Of Fiber For Overall Health?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
‘It’s okay to poo at work’: new health campaign highlights a common source of anxiety
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For most people, the daily or near-daily ritual of having a bowel motion is not something we give a great deal of thought to. But for some people, the need to do a “number two” in a public toilet or at work can be beset with significant stress and anxiety.
In recognition of the discomfort people may feel around passing a bowel motion at work, the Queensland Department of Health recently launched a social media campaign with the message “It’s okay to poo at work”.
The campaign has gained significant traction on Instagram and Facebook. It has been praised by health and marketing experts for its humorous handling of a taboo topic.
A colourful Instagram post is accompanied by a caption warning of the health risks of “holding it in”, including haemorrhoids and other gastrointestinal problems. The caption also notes:
If you find it extremely difficult to poo around other people, you might have parcopresis.
Queensland Health/Instagram What is parcopresis?
Parcopresis, sometimes called “shy bowel”, occurs when people experience a difficulty or inability to poo in public toilets due to fear of perceived scrutiny by others.
People with parcopresis may find it difficult to go to the toilet in public places such as shopping centres, restaurants, at work or at school, or even at home when friends or family are around.
They may fear being judged by others about unpleasant smells or sounds when they have a bowel motion, or how long they take to go, for example.
Living with a gastrointestinal condition (at least four in ten Australians do) may contribute to parcopresis due to anxiety about the need to use a toilet frequently, and perceived judgment from others when doing so. Other factors, such as past negative experiences or accessibility challenges, may also play a role.
Some people may feel uncomfortable about using the toilet at work. Motortion Films/Shutterstock For sufferers, anxiety can present in the form of a faster heart rate, rapid breathing, sweating, muscle tension, blushing, nausea, trembling, or a combination of these symptoms. They may experience ongoing worry about situations where they may need to use a public toilet.
Living with parcopresis can affect multiple domains of life and quality of life overall. For example, sufferers may have difficulties relating to employment, relationships and social life. They might avoid travelling or attending certain events because of their symptoms.
How common is parcopresis?
We don’t really know how common parcopresis is, partly due to the difficulty of evaluating this behaviour. It’s not necessarily easy or appropriate to follow people around to track whether they use or avoid public toilets (and their reasons if they do). Also, observing individual bathroom activities may alter the person’s behaviour.
I conducted a study to try to better understand how common parcopresis is. The study involved 714 university students. I asked participants to respond to a series of vignettes, or scenarios.
In each vignette participants were advised they were at a local shopping centre and they needed to have a bowel motion. In the vignettes, the bathrooms (which had been recently cleaned) had configurations of either two or three toilet stalls. Each vignette differed by the configuration of stalls available.
The rate of avoidance was just over 14% overall. But participants were more likely to avoid using the toilet when the other stalls were occupied.
Around 10% avoided going when all toilets were available. This rose to around 25% when only the middle of three toilets was available. Men were significantly less likely to avoid going than women across all vignettes.
For those who avoided the toilet, many either said they would go home to poo, use an available disabled toilet, or come back when the bathroom was empty.
Parcopresis at work
In occupational settings, the rates of anxiety about using shared bathrooms may well be higher for a few reasons.
For example, people may feel more self-conscious about their bodily functions being heard or noticed by colleagues, compared to strangers in a public toilet.
People may also experience guilt, shame and fear about being judged by colleagues or supervisors if they need to make extended or frequent visits to the bathroom. This may particularly apply to people with a gastrointestinal condition.
Reducing restroom anxiety
Using a public toilet can understandably cause some anxiety or be unpleasant. But for a small minority of people it can be a real problem, causing severe distress and affecting their ability to engage in activities of daily living.
If doing a poo in a toilet at work or another public setting causes you anxiety, be kind to yourself. A number of strategies might help:
- identify and challenge negative thoughts about using public toilets and remind yourself that using the bathroom is normal, and that most people are not paying attention to others in the toilets
- try to manage stress through relaxation techniques such as deep breathing and progressive muscle relaxation, which involves tensing and relaxing different muscles around the body
- engaging in gradual exposure can be helpful, which means visiting public toilets at different times and locations, so you can develop greater confidence in using them
- use grounding or distraction techniques while going to the toilet. These might include listening to music, watching something on your phone, or focusing on your breathing.
If you feel parcopresis is having a significant impact on your life, talk to your GP or a psychologist who can help identify appropriate approaches to treatment. This might include cognitive behavioural therapy.
Simon Robert Knowles, Associate Professor and Clinical Psychologist, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stop Trying To Lose Weight (And Do This Instead)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Lose weight” is a common goal of many people, and it’s especially a common goal handed down from medical authority figures, often as a manner of “kicking the can down the road” with regard to the doctor actually having to do some work. “Lose 20 pounds and then we’ll talk”, etc.
The thing is, it’s often not a very good or helpful goal… Even if it would be healthy for a given person to lose weight. Instead, biochemist Jessie Inchauspé argues, one should set a directly health-giving goal instead, and let any weight loss, if the body agrees it is appropriate, be a by-product of that
She recommends focusing on metabolic health, specifically, her own specialism is blood glucose maintenance. This is something that diabetics deal with (to one degree or another) every day, but it’s something whose importance should not be underestimated for non-diabetics too.
Keep our blood sugar levels healthy, she says, and a lot of the rest of good health will fall into place by itself—precisely because we’re not constantly sabotaging our body (first the pancreas and liver, then the rest of the body like dominoes).
To that end, she offers a multitude of “hacks” that really work.
Her magnum opus, “Glucose Revolution“, explains the science in great detail and does it very well! Not to be mistaken for her shorter, simpler, and entirely pragmatic “do this, then this”-style book, “The Glucose Goddess Method”, which is also great, but doesn’t go into the science more than absolutely necessary; it’s more for the “I’ll trust you; just tell me what I need to know” crowd.
In her own words:
Click Here If The Embedded Video Doesn’t Load Automatically!
Prefer text?
We’ve covered Inchauspé’s top 10 recommended hacks here:
10 Ways To Balance Blood Sugars
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: