Relationships: When To Stick It Out & When To Call It Quits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Like A Ship Loves An Anchor?
Today’s article may seem a little bit of a downer to start with, but don’t worry, it picks up again too. Simply put, we’ve written before about many of the good parts of relationships, e.g:
Only One Kind Of Relationship Promotes Longevity This Much!
…but what if that’s not what we have?
Note: if you have a very happy, secure, fulfilling, joyous relationship, then, great! Or if you’re single and happy, then, also great! Hopefully you will still find today’s feature of use if you find yourself advising a friend or family member one day. So without further ado, let’s get to it…
You may be familiar with the “sunk cost fallacy”; if not: it’s what happens when a person or group has already invested into a given thing, such that even though the thing is not going at all the way they hoped, they now want to continue trying to make that thing work, lest their previous investment be lost. But the truth is: if it’s not going to work, then the initial investment is already lost, and pouring out extra won’t help—it’ll just lose more.
That “investment” in a given thing could be money, time, energy, or (often the case) a combination of the above.
In the field of romance, the “sunk cost fallacy” keeps a lot of bad relationships going for longer than perhaps they should, and looking back (perhaps after a short adjustment period), the newly-single person says “why did I let that go on?” and vows to not make the same mistake again.
But that prompts the question: how can we know when it’s right to “keep working on it, because relationships do involve work”, as perfectly reasonable relationship advice often goes, and when it’s right to call it quits?
Should I stay or should I go?
Some questions for you (or perhaps a friend you might find yourself advising) to consider:
- What qualities do you consider the most important for a partner to have—and does your partner have them?
- If you described the worst of your relationship to a close friend, would that friend feel bad for you?
- Do you miss your partner when they’re away, or are you glad of the break? When they return, are they still glad to see you?
- If you weren’t already in this relationship, would you seek to enter it now? (This takes away sunk cost and allows a more neutral assessment)
- Do you feel completely safe with your partner (emotionally as well as physically), or must you tread carefully to avoid conflict?
- If your partner decided tomorrow that they didn’t want to be with you anymore and left, would that be just a heartbreak, or an exciting beginning of a new chapter in your life?
- What things would you generally consider dealbreakers in a relationship—and has your partner done any of them?
The last one can be surprising, by the way. We often see or hear of other people’s adverse relationship situations and think “I would never allow…” yet when we are in a relationship and in love, there’s a good chance that we might indeed allow—or rather, excuse, overlook, and forgive.
And, patience and forgiveness certainly aren’t inherently bad traits to have—it’s just good to deploy them consciously, and not merely be a doormat.
Either way, reflect (or advise your friend/family member to reflect, as applicable) on the “score” from the above questions.
- If the score is good, then maybe it really is just a rough patch, and the tools we link at the top and bottom of this article might help.
- If the score is bad, the relationship is bad, and no amount of historic love or miles clocked up together will change that. Sometimes it’s not even anyone’s fault; sometimes a relationship just ran its course, and now it’s time to accept that and turn to a new chapter.
“At my age…”
As we get older, it’s easy for that sunk cost fallacy to loom large. Inertia is heavy, the mutual entanglement of lives is far-reaching, and we might not feel we have the same energy for dating that we did when we were younger.
And there may sometimes be a statistical argument for “sticking it out” at least for a while, depending on where we are in the relationship, per this study (with 165,039 participants aged 20–76), which found:
❝Results on mean levels indicated that relationship satisfaction decreased from age 20 to 40, reached a low point at age 40, then increased until age 65, and plateaued in late adulthood.
As regards the metric of relationship duration, relationship satisfaction decreased during the first 10 years of the relationship, reached a low point at 10 years, increased until 20 years, and then decreased again.❞
Source: Development of Relationship Satisfaction Across the Life Span: A Systematic Review and Meta-Analysis
And yet, when it comes to prospects for a new relationship…
- If our remaining life is growing shorter, then it’s definitely too short to spend in an unhappy relationship
- Maybe we really won’t find romance again… And maybe that’s ok, if w’re comfortable making our peace with that and finding joy in the rest of life (this widowed writer (hi, it’s me) plans to remain single now by preference, and her life is very full of purpose and beauty and joy and yes, even love—for family, friends, etc, plus the memory of my wonderful late beloved)
- Nevertheless, the simple fact is: many people do find what they go on to describe as their best relationship yet, late in life ← this study is with a small sample size, but in this case, even anecdotal evidence seems sufficient to make the claim reasonable; probably you personally know someone who has done so. If they can, so can you, if you so wish.
- Adding on to that last point… Later life relationships can also offer numerous significant advantages unique to such (albeit some different challenges too—but with the right person, those challenges are just a fun thing to tackle together). See for example:
An exploratory investigation into dating among later‐life women
And about those later-life relationships that do work? They look like this:
this one looks like the title says it all, but it really doesn’t, and it’s very much worth at least reading the abstract, if not the entire paper—because it talks a lot about the characteristics that make for happy or unhappy relationships, and the effect that those things have on people. It really is very good, and quite an easy read.
See again: Healthy Relationship, Healthy Life
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Carrot vs Sweet Potato – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing carrot to sweet potato, we picked the sweet potato.
Why?
Both are great! But there’s a winner in the end:
Looking at the macros first, sweet potato has more protein carbs, and fiber, and is thus the “more food per food” item. If they are both cooked the same, then the glycemic index is comparable, despite the carrot’s carbs having more sucrose and the sweet potato’s carbs having more starch. We’ll call this category a tie.
In terms of vitamins, carrots have more of vitamins B9 and K, while sweet potatoes have more of vitamins B1, B2, B3, B5, B6. B7, C, E, and choline. Both are equally high in vitamin A. Thus, the vitamins category is an overwhelming win for sweet potato.
When it comes to minerals, carrots are not higher in any minerals (unless we count that they are slightly higher in sodium, but that is not generally considered a plus for most people in most places most of the time), while sweet potato is higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for sweet potato.
Adding up the sections makes for a clear win for the sweet potato as the more nutritionally dense option, but as ever, enjoy either or both!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Share This Post
-
How To Get Your First Pull-Up
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Pull-ups are a great compound exercise that works most of the upper body. However, it can be frustrating for many, if unable to do more than dangle and struggle while not going anywhere. That’s not actually bad, by the way! Of course it’s not great athletic performance, but in terms of exercise, “dangling and struggling while not going anywhere” is an isometric exercise that has plenty of benefits of its own. However, for those who would rather go up in the world, personal trainer Meg Gallagher shows the way:
The Only Way Is Up?
Gallagher offers a few methods; the first is simply an improvement on the “dangling and struggling while not going anywhere” method, but doing it with good form. It’s called the…
Hollow body hold:
- Hang from the bar with legs and feet together.
- Maintain a posterior pelvic tilt (i.e. don’t let your hips roll forwards, and don’t let your butt stick out more than is necessary by mere virtue of having a butt)
- Engage your core by shortening the space between your ribs and pelvis.
- Turn on your abs and lats, with your head slightly behind the bar.
- Practice the hollow body hang instead of dead hangs to build grip and core strength.
Another method is now moving on from the hollow body hold, and shows that in fact, up is not the only way. It’s called…
Negative pull-ups:
- Jump up to get your chin over the bar, then slowly lower yourself in a controlled manner.
- Prioritize negative pull-ups over other exercises to build strength.
- You can use modifications like resistance bands or feet assistance if necessary to extend the duration of your negative pull-up, but these are “crutches”, so try to move on from them as soon as you reasonably can—same if your gym has an “assisted pull-up” machine, consisting of a moving platform with a variable counterweight, mimicking how a pull-up would feel if your body were lighter.
- Practice resisting throughout the entire range of motion.
To give a sense of direction, Gallagher offers the following program:
- On day 1, test how long you can resist the negative pull-up (e.g., 10 seconds).
- For each session, multiply your time by 2 (e.g., 10 seconds × 2 = 20 seconds total).
- Break the total volume into as many sets as needed (e.g., 2 sets of 10 seconds or 4 sets of 5 seconds).
- After each session, add 2 seconds to the total volume for the next session.
- Aim for 3 sessions per week for 3–4 weeks, increasing by 2 seconds each session.
- When you reach about 25 seconds, you should be close to performing your first pull-up.
For more on all of this, plus a few other things to try, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post
-

The Intelligence Trap – by David Robson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’re including this one under the umbrella of “general wellness”, because it happens that a lot of very intelligent people make stunningly unfortunate choices sometimes, for reasons that may baffle others.
The author outlines for us the various reasons that this happens, and how. From the famous trope of “specialized intelligence in one area”, to the tendency of people who are better at acquiring knowledge and understanding to also be better at acquiring biases along the way, to the hubris of “I am intelligent and therefore right as a matter of principle” thinking, and many other reasons.
Perhaps the greatest value of the book is the focus on how we can avoid these traps, narrow our bias blind spots, and play to our strengths while paying full attention to our weaknesses.
The style is very readable, despite having a lot of complex ideas discussed along the way. This is entirely to be expected of this author, an award-winning science writer.
Bottom line: if you’d like to better understand the array of traps that disproportionately catch out the most intelligent people (and how to spot such), then this is a great book for you.
Click here to check out The Intelligence Trap, and be more wary!
Share This Post
Related Posts
-
Passion Fruit vs Pomegranate – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing passion fruit to pomegranate, we picked the passion fruit.
Why?
Both of these fruits have beaten a lot of other contenders, so it’s time to pit them against each other:
In terms of macros, passion fruit has more protein, carbs, and fiber, the ratio of which meaning also that passion fruit has the lower glycemic index. So, we say passion fruit wins on macros.
In the category of vitamins, things are more even; passion fruit has more of vitamins A, B2, B3, B6, and C, while pomegranate has more of vitamins B1, B5, B9, E, and K. In light of this 5:5 tie, and since passion fruit’s overall vitamin coverage is better (in terms of meeting RDA needs) but pomegranate’s vitamins are often in shorter supply in diet, we’re calling it a tie on vitamins.
When it comes to minerals, passion fruit has more calcium, iron, magnesium, phosphorus, potassium, and selenium, while pomegranate has more copper, manganese, and zinc. That’s already an easy 6:3 win for passion fruit, before we even consider the fact that passion fruit’s minerals’ margin of difference is greater too.
Adding it up makes for a clear win for passion fruit. As ever when it comes to plants, enjoy both if you can, though!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Kimchi Fried Rice
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fried rice is not something that leaps to many people’s minds when one says “health food”. But it can be! Today’s recipe is great for many aspects of health, but especially the gut, because of its star ingredient, the kimchi—as well as the fiber in the rest of the dish, which is mostly a variety of vegetables, as well as the rice, which we are assuming you got wholegrain. An optional egg per person adds more healthy fats too!
You will need
- Avocado oil, for frying. We picked avocado oil for its healthy fats profile, neutral taste, and high smoke point (we’ll be working at very high temperatures today that might make olive oil or coconut oil smoke). We also recommend against seed oils (e.g. sunflower or canola) for health reasons.
- 1lb cooked and cooled rice—here’s our recipe for Tasty Versatile Rice if you don’t have leftovers you want to use
- 7oz kimchi, roughly chopped
- 4 spring onions, finely chopped
- 4oz white cabbage, finely shredded
- 3oz frozen peas, defrosted
- 1 bulb garlic, thinly sliced
- 1 carrot, grated
- ½ red pepper, finely diced
- 2 tbsp chili oil (or 2 tbsp extra virgin olive oil and 1 red chili, very finely chopped) ← don’t worry about the smoke point of this; it’s going to be for drizzling
- 1 tbsp dark soy sauce
- 2 tsp black pepper, coarse ground
- Optional: 1 egg per person
- Note: we didn’t forget to include salt; there’s simply enough already in the dish because of the kimchi and soy sauce.
Method
(we suggest you read everything at least once before doing anything)
1) Lightly oil a wok (or similar) and crank up the heat as high as your stove can muster. Add the garlic and spring onions; keep them moving. When they’re turning golden, add the cabbage, carrot, and red pepper. Add them one by one, giving the wok a chance to get back to temperature each time before adding the next ingredient.
2) When the vegetables are beginning to caramelize (if the temperature is good, this should only be a couple of minutes at most), add the rice, as well as the kimchi, peas, soy sauce, and black pepper. Toss everything ensure it’s all well-combined and evenly cooked. When it’s done (probably only another minute or two), take it off the heat.
3) Optional: if you’re adding eggs, fry them now. Serve a bowl of kimchi-fried rice per person, adding 1 fried egg on top of each.
4) Drizzle the chili oil as a colorful, tasty garnish that’s full of healthful polyphenols too.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Making Friends With Your Gut (You Can Thank Us Later)
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Tasty Polyphenols ← this is about how foods that are pungent, bitter, spicy, etc tend to have the highest polyphenol contents
- Eggs: All Things In Moderation?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sleep wrinkles are real. Here’s how they leave their mark
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You wake up, stagger to the bathroom and gaze into the mirror. No, you’re not imagining it. You’ve developed face wrinkles overnight. They’re sleep wrinkles.
Sleep wrinkles are temporary. But as your skin loses its elasticity as you age, they can set in.
Here’s what you can do to minimise the chance of them forming in the first place.
How side-sleeping affects your face
Your skin wrinkles for a number of reasons, including ageing, sun damage, smoking, poor hydration, habitual facial expressions (such as grinning, pouting, frowning, squinting) and sleeping positions.
When you sleep on your side or stomach, your face skin is squeezed and crushed a lot more than if you sleep on your back. When you sleep on your side or stomach, gravity presses your face against the pillow. Your face skin is distorted as your skin is stretched, compressed and pulled in all directions as you move about in your sleep.
You can reduce these external forces acting on the face by sleeping on your back or changing positions frequently.
Doctors can tell which side you sleep on by looking at your face
In a young face, sleep wrinkles are transient and disappear after waking.
Temporary sleep wrinkles can become persistent with time and repetition. As we age, our skin loses elasticity (recoil) and extensibility (stretch), creating ideal conditions for sleep wrinkles or lines to set in and last longer.
The time spent in each sleeping position, the magnitude of external forces applied to each area of the face, as well as the surface area of contact with the pillow surface, also affects the pattern and rate of sleep wrinkle formation.
Skin specialists can often recognise this. People who favour sleeping on one side of their body tend to have a flatter face on their sleeping side and more visible sleep lines.
Can a night skincare routine avoid sleep wrinkles?
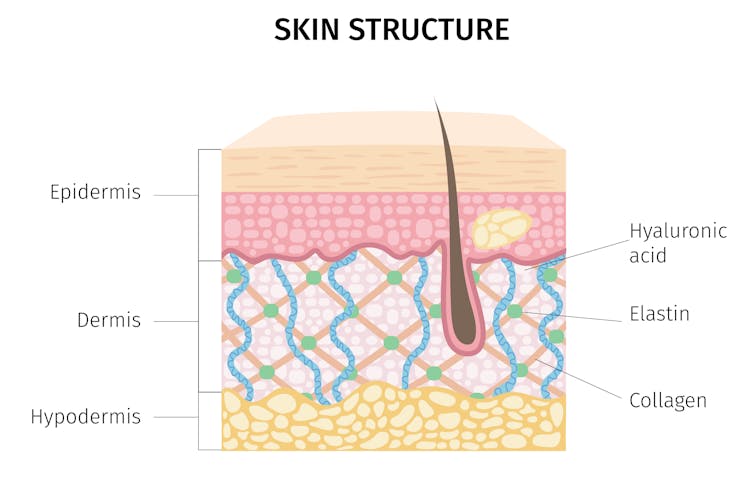
Collagen and elastin are two primary components of the dermis (inner layer) of skin. They form the skin structure and maintain the elasticity of skin.
The dermis is the inner layer of skin. mermaid3/Shutterstock Supplementing collagen through skincare routines to enhance skin elasticity can help reduce wrinkle formation.
Hyaluronic acid is a naturally occurring molecule in human bodies. It holds our skin’s collagen and elastin in a proper configuration, stimulates the production of collagen and adds hydration, which can help slow down wrinkle formation. Hyaluronic acid is one of the most common active ingredients in skincare creams, gels and lotions.
Moisturisers can hydrate the skin in different ways. “Occlusive” substances produce a thin layer of oil on the skin that prevents water loss due to evaporation. “Humectants” attract and hold water in the skin, and they can differ in their capacity to bind with water, which influences the degree of skin hydration.
Do silk pillowcases actually make a difference?
Can they help? New Africa/Shutterstock Silk pillowcases can make a difference in wrinkle formation, if they let your skin glide and move, rather than adding friction and pressure on a single spot. If you can, use silk sheets and silk pillows.
Studies have also shown pillows designed to reduce mechanical stress during sleep can prevent skin deformations. Such a pillow could be useful in slowing down and preventing the formation of certain facial wrinkles.
Sleeping on your back can reduce the risk of sleep lines, as can a nighttime routine of moisturising before sleep.
Otherwise, lifestyle choices and habits, such quitting smoking, drinking plenty of water, a healthy diet (eating enough vegetables, fruits, nuts, seeds, healthy fats, yogurt and other fermented foods) and regular use of sunscreens can help improve the appearance of the skin on our face.
Yousuf Mohammed, Dermatology researcher, The University of Queensland; Khanh Phan, Postdoctoral Research Fellow, Frazer Institute, The University of Queensland, and Vania Rodrigues Leite E. Silva, Honorary Associate Professor, Frazer Institute, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: