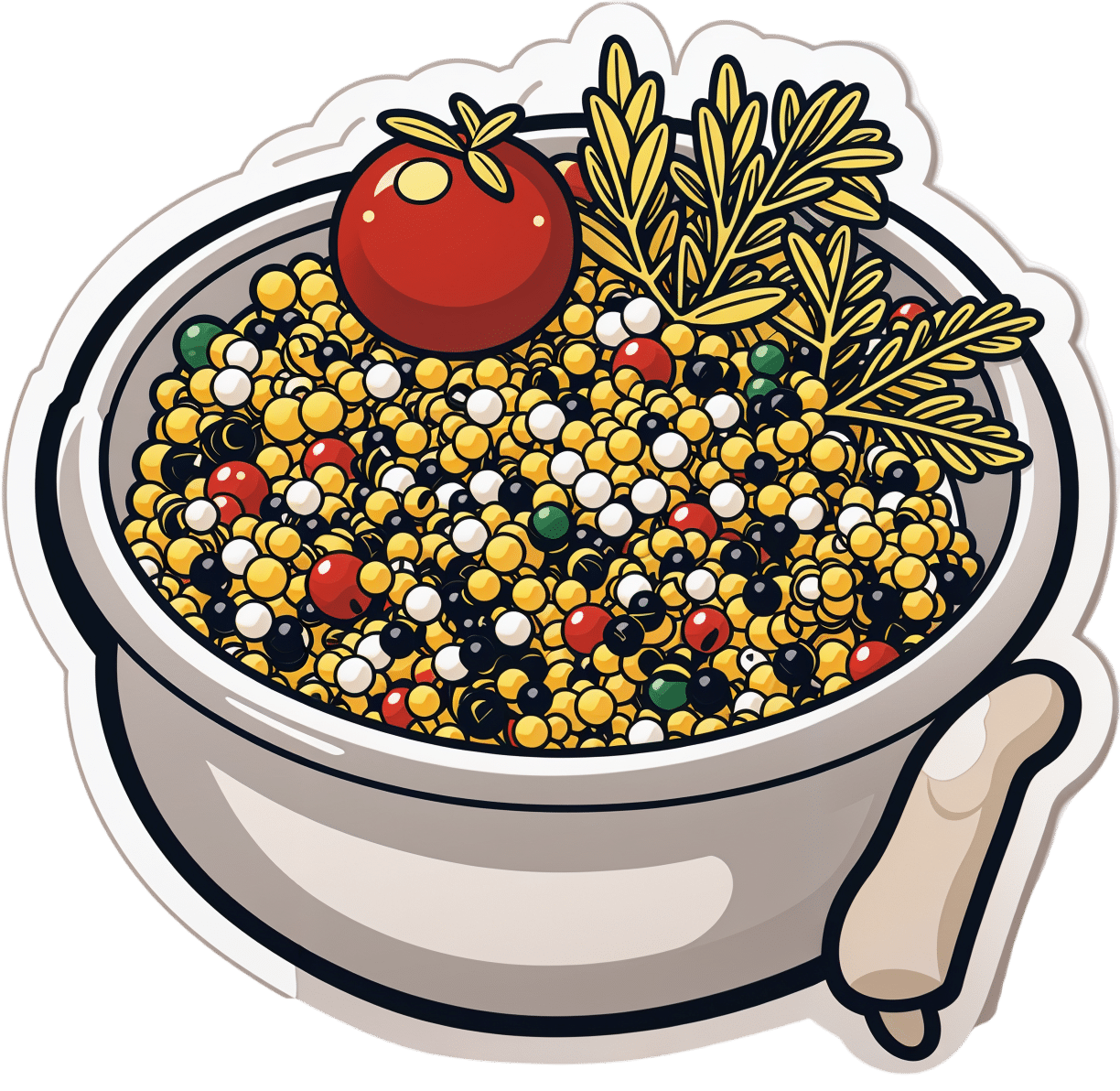
Omega-3 Mushroom Spaghetti
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The omega-3 is not the only healthy fat in here; we’re also going to have medium-chain triglycerides, as well as monounsaturates. Add in the ergothioneine from the mushrooms and a stack of polyphenols from, well, most of the ingredients, not to mention the fiber, and this comes together as a very healthy dish. There’s also about 64g protein in the entire recipe, so you do the math for how much that is per serving, depending on how big you want the servings to be.
You will need
- 1lb wholewheat spaghetti (or gluten-free equivalent, such as a legume-based pasta, if avoiding gluten/wheat)
- 12oz mushrooms, sliced (any non-poisonous edible variety)
- ½ cup coconut milk
- ½ onion, finely chopped
- ¼ cup chia seeds
- ¼ bulb garlic, minced (or more, if you like)
- 2 tbsp extra virgin olive oil
- 1 tbsp black pepper, coarse ground
- 1 tbsp lime juice
Method
(we suggest you read everything at least once before doing anything)
1) Cook the spaghetti according to packet instructions, or your own good sense, aiming for al dente. When it’s done, drain it, and lastly rinse it (with cold water), and set it aside.
2) Heat the olive oil in a skillet and add the onion, cooking for 5 minutes
3) Add the garlic, mushrooms, and black pepper, cooking for another 8 minutes.
4) Add the coconut milk, lime juice, and chia seeds, stirring well and cooking for a further two minutes
5) Reheat the spaghetti by passing boiling water through it in a colander (the time it spent cold was good for it; it lowered the glycemic index)
6) Serve, adding the mushroom sauce to the spaghetti:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The Magic of Mushrooms: “The Longevity Vitamin” (That’s Not A Vitamin)
- The Many Health Benefits of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- If You’re Not Taking Chia, You’re Missing Out
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Cavolo Nero & Sweet Potato Hash

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
🎶 Sweet potato hash? It’s a seasonal smash… Catches on in a flash… Let’s do the hash 🎶
You will need
- 6 oz cavolo nero, tough stems removed, chopped
- 1 large sweet potato, diced
- 1 large red onion, finely chopped
- 1 parsnip, grated
- 1 small red pepper, chopped
- 4 oz baby portobello mushrooms, chopped
- ½ cup fresh or thawed peas
- ¼ bulb garlic, thinly sliced
- 1 tbsp nutritional yeast
- 2 tsp black pepper, coarse ground
- 1 tsp dried rosemary
- 1 tsp dried thyme (dried for convenience; fresh is also fine if you have it)
- 1 tsp red chili flakes (dried for convenience; fresh is also fine if you have it)
- 1 tsp ground turmeric
- ½ tsp MSG or 1 tsp low-sodium salt
- Extra virgin olive oil
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 425℉ / 220℃.
2) Toss the diced sweet potato in 1 tbsp olive oil, as well as the nutritional yeast, ground turmeric, black pepper, and MSG/salt, ensuring an even distribution. Roast in the oven on a lined baking tray, for 30 minutes, turning at least once to get all sides of the potato. When it is done, remove from the oven and set aside.
3) Heat a little oil in a sauté pan or large skillet (either is fine; we’re not adding liquids today), and fry the onion, parsnip, and pepper until softened, which should take about 5 minutes (this is one reason why we grated the parsnip; the other is for the variation in texture).
4) Add the garlic, mushrooms, herbs, and chili flakes, and cook for a further 1 minute, while stirring.
5) Add the cavolo nero and peas, stir until the cavolo nero begins to wilt, and then…
6) Add the roasted sweet potato; cook for about 5 more minutes, pressing down with the spatula here and there to mash the ingredients together.
7) Turn the hash over when it begins to brown on the bottom, to lightly brown the other side too.
8) Serve hot.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Brain Food? The Eyes Have It!
- Which Bell Peppers To Pick?
- Ergothioneine: “The Longevity Vitamin” (That’s Not A Vitamin)
- Our Top 5 Spices: How Much Is Enough For Benefits?
- What’s Your Plant Diversity Score?
Take care!
Share This Post
-

The Uses of Delusion – by Dr. Stuart Vyse
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most of us try to live rational lives. We try to make the best decisions we can based on the information we have… And if we’re thoughtful, we even try to be aware of common logical fallacies, and overcome our personal biases too. But is self-delusion ever useful?
Dr. Stuart Vyse, psychologist and Fellow for the Committee for Skeptical Inquiry, argues that it can be.
From self-fulfilling prophecies of optimism and pessimism, to the role of delusion in love and loss, Dr. Vyse explores what separates useful delusion from dangerous irrationality.
We also read about such questions as (and proposed answers to):
- Why is placebo effect stronger if we attach a ritual to it?
- Why are negative superstitions harder to shake than positive ones?
- Why do we tend to hold to the notion of free will, despite so much evidence for determinism?
The style of the book is conversational, and captivating from the start; a highly compelling read.
Bottom line: if you’ve ever felt yourself wondering if you are deluding yourself and if so, whether that’s useful or counterproductive, this is the book for you!
Click here to check out The Uses of Delusion, and optimize yours!
Share This Post
-

The Mind-Gut Connection – by Dr. Emeran Mayer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed books about the mind-gut connection before, so what makes this one stand out?
Firstly, it’s a lot more comprehensive than the usual “please, we’re begging you, eat some fiber”.
And yes, of course that’s part of it. Prebiotics, probiotics, reduce fried and processed foods, reduce sugar/alcohol, reduce meat, and again, eat some greenery.
But where this book really comes into its own is looking more thoroughly at the gut microbiota and their function. Dr. Mayer goes well beyond “there are good and bad bacteria” and looks at the relationship each of them have with the body’s many hormones, and especially neurotransmitters like serotonin and dopamine.
He also looks at the two-way connection between brain and gut. Yes, our gut gives us “gut feelings”, but 10% of communication between the brain and gut is in the other direction; he explores what that means for us, too.
Finally, he does give a lot of practical advice, not just dietary but also behavioral, to make the most of our mind-gut connection and make it work for our health, rather than against it.
Bottom line: this is the best book on the brain-gut connection that this reviewer has read so far, and certainly the most useful if you already know about gut-healthy nutrition, and are looking to take your understanding to the next level.
Click here to check out The Mind-Gut Connection, and start making yours work for your benefit!
Share This Post

Related Posts
-

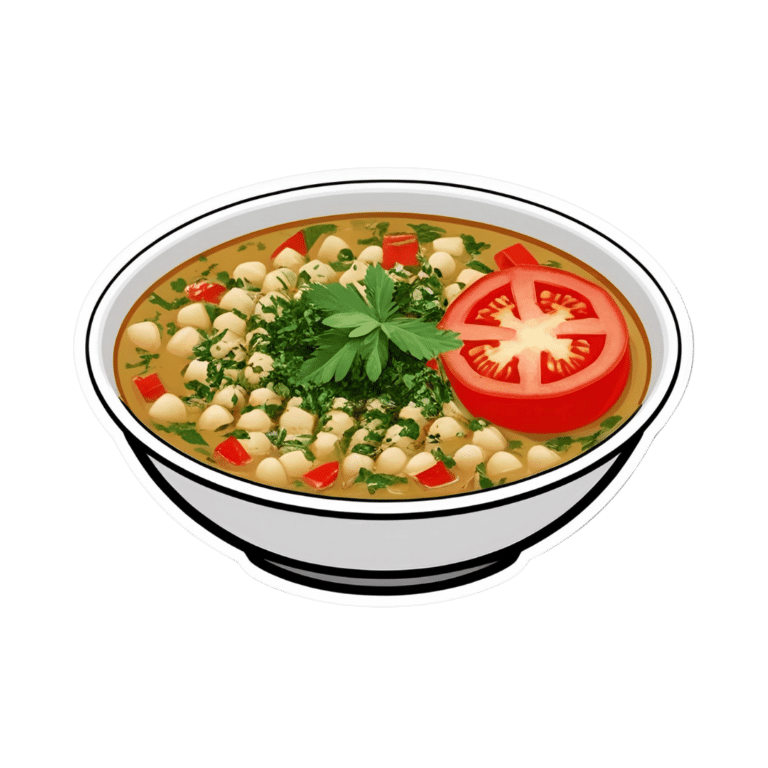
Tasty Tabbouleh with Tahini
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Tabbouleh is a salad, but it’s not “just a salad”. It’s a special kind of salad that’s as exciting for the tastebuds as it is healthy for the body and brain. Its core ingredients have been traditional for about a dozen generations, and seasonings are always a personal matter (not to mention that Lebanese tabbouleh-makers centuries ago might not have used miso and nooch, as we will today), but the overall feel of the Gestalt of tabbouleh seasonings remains the same, and this recipe is true to that.
You will need
For the tabbouleh:
- 1 cup bulgur wheat
- 1 cup plum tomatoes, chopped
- 1 cucumber, peeled and chopped (add the peel to a jug of water and put it in the fridge; this will be refreshing cucumber water later!)
- 1 cup chickpeas, cooked without salt
- 1/2 cup parsley, chopped
- 1/2 cup mint, chopped
- 2 spring onions, finely chopped
- 2oz fresh lemon juice
- 1 tsp white miso paste
- 1 tsp garlic powder
- 1 tsp ground cumin
- 1 tsp ground celery seeds
- 1 tsp ground nigella seeds
- 1 tsp ground black pepper
- 1 tsp MSG, or 1/2 tsp low sodium salt (you can find it in supermarkets, the sodium chloride is cut with potassium chloride to make it have less sodium and more potassium)
- 1 tbsp nutritional yeast (nooch), ground (it comes in flakes; you will have to grind it in a spice grinder or with a pestle and mortar)
For the tahini sauce:
- 3 garlic cloves, crushed
- 3 tbsp tahini
- 1 tbsp fresh lemon juice
- 1 tbsp white miso paste
- 1 tsp ground cumin
To serve:
- A generous helping of leafy greens; we recommend collard greens, but whatever works for you is good; just remember that dark green is best. Consider cavolo nero, or even kale if that’s your thing, but to be honest this writer doesn’t love kale
- 1 tsp coarsely ground nigella seeds
- Balsamic vinegar, ideally aged balsamic vinegar (this is thicker and sweeter, but unlike most balsamic vinegar reductions, doesn’t have added sugar).
Method
(we suggest you read everything at least once before doing anything)
1) Rinse the bulgur wheat and then soak it in warm water. There is no need to boil it; the warm water is enough to soften it and you don’t need to cook it (bulgur wheat has already been parboiled before it got to you).
2) While you wait, take a small bowl and mix the rest of the ingredients from the tabbouleh section (so, the lemon juice, miso paste, and all those ground spices and MSG/salt and ground nutritional yeast); you’re making a dressing out of all the ingredients here.
3) When the bulgur wheat is soft (expect it to take under 15 minutes), drain it and put it in a big bowl. Add the tomatoes, cucumber, chickpeas, parsley, mint, and spring onions. This now technically qualifies as tabbouleh already, but we’re not done.
4) Add the dressing to the tabbouleh and mix thoroughly but gently (you don’t want to squash the tomatoes, cucumber, etc). Leave it be for at least 15 minutes while the flavors blend.
5) Take the “For the tahini sauce” ingredients (all of them) and blend them with 4 oz water, until smooth. You’re going to want to drizzle this sauce, so if the consistency is too thick for drizzling, add a little more water and/or lemon juice (per your preference), 1 tbsp at a time.
6) Roughly chop the leafy greens and put them in a bowl big enough for the tabbouleh to join them there. The greens will serve as a bed for the tabbouleh itself.
7) Drizzle the tahini over the tabbouleh, and drizzle a little of the aged balsamic vinegar too.
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Castor Oil: All-Purpose Life-Changer, Or Snake Oil?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As “trending” health products go, castor oil is enjoying a lot of popularity presently, lauded as a life-changing miracle-worker, and social media is abuzz with advice to put it everywhere from your eyes to your vagina.
But:
- what things does science actually say it’s good for,
- what things lack evidence, and
- what things go into the category of “wow definitely do not do that”?
We don’t have the space to go into all of its proposed uses (there are simply far too many), but we’ll examine some common ones:
To heal/improve the skin barrier
Like most oils, it’s functional as a moisturizer. In particular, its high (90%!) ricinoleic fatty acid content does indeed make it good at that, and furthermore, has properties that can help reduce skin inflammation and promote wound healing:
Bioactive polymeric formulations for wound healing ← there isn’t a conveniently quotable summary we can just grab here, but you can see the data and results, from which we can conclude:
- formulations with ricinoleic acid (such as with castor oil) performed very well for topical anti-inflammatory purposes
- they avoided the unwanted side effects associated with some other contenders
- they consistently beat other preparations in the category of wound-healing
To support hair growth and scalp health
There is no evidence that it helps. We’d love to provide a citation for this, but it’s simply not there. There’s also no evidence that it doesn’t help. For whatever reason, despite its popularity, peer-reviewed science has simply not been done for this, or if it has, it wasn’t anywhere publicly accessible.
It’s possible that if a person is suffering hair loss specifically as a result of prostaglandin D2 levels, that ricinoleic acid will inhibit the PGD2, reversing the hair loss, but even this is hypothetical so far, as the science is currently only at the step before that:
However, due to some interesting chemistry, the combination of castor oil and warm water can result in acute (and irreversible) hair felting, in other words, the strands of hair suddenly glue together to become one mass which then has to be cut off:
“Castor Oil” – The Culprit of Acute Hair Felting
👆 this is a case study, which is generally considered a low standard of evidence (compared to high-quality Randomized Controlled Trials as the highest standard of evidence), but let’s just say, this writer (hi, it’s me) isn’t risking her butt-length hair on the off-chance, and doesn’t advise you to, either. There are other hair-oils out there; argan oil is great, coconut oil is totally fine too.
As a laxative
This time, there’s a lot of evidence, and it’s even approved for this purpose by the FDA, but it can be a bit too good, insofar as taking too much can result in diarrhea and uncomfortable cramping (the cramps are a feature not a bug; the mechanism of action is stimulatory, i.e. it gets the intestines squeezing, but again, it can result in doing that too much for comfort):
Castor Oil: FDA-Approved Indications
To soothe dry eyes
While putting oil in your eyes may seem dubious, this is another one where it actually works:
❝Castor oil is deemed safe and tolerable, with strong anti-microbial, anti-inflammatory, anti-nociceptive, analgesic, antioxidant, wound healing and vasoconstrictive properties.
These can supplement deficient physiological tear film lipids, enabling enhanced lipid spreading characteristics and reducing aqueous tear evaporation.
Studies reveal that castor oil applied topically to the ocular surface has a prolonged residence time, facilitating increased tear film lipid layer thickness, stability, improved ocular surface staining and symptoms.❞
Source: Therapeutic potential of castor oil in managing blepharitis, meibomian gland dysfunction and dry eye
Against candidiasis (thrush)
We couldn’t find science for (or against) castor oil’s use against vaginal candidiasis, but here’s a study that investigated its use against oral candidiasis:
…in which castor oil was the only preparation that didn’t work against the yeast.
Summary
We left a lot unsaid today (so many proposed uses, it feels like a shame to skip them), but in few words: it’s good for skin (including wound healing) and eyes; but we’d give it a miss for hair, candidiasis, and digestive disorders.
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon 😎
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Healthiest Bread Recipe You’ll Probably Find
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝[About accidental scalding with water] Is cold water actually the best immediate treatment for a burn? Maybe there is something better, or something I should apply after the cold water.❞
If this is a case of spilled tea or similar—as in your story, which (apologies) we clipped for brevity—indeed, cold running water is best, and nothing else should be needed. It’s up to you whether you want to invest the time based on the extent of the scalding, but 10 minutes is recommended to minimize tissue damage.
If it’s a more severe scalding or burning, seek medical attention immediately. If it’s a burn to anywhere other than the airway, cold running water is still best for 10 minutes, but if you have to choose between that and professional medical attention, don’t delay the help.
If it’s a burn you’ve given 10 minutes of cold running water and it still hurts and/or has blistered, cover it in a sterile, non-adhesive dressing that extends well beyond the visible burn (because the actual damage probably extends further, and you don’t want to find this out the hard way later). If the burn is to the face, do still irrigate but not cover it; wait for help.
Do not apply any kind of cream, lotion, oil, etc. No matter how tempting, no matter where the burn is.
All of the above also goes for splashed oil, chemical burns, and electrical burns too (but obviously, make sure to get away from the electricity first).
Source: this ex-military writer was trained for this sort of thing and, suffice it to say, has dealt with more serious things than spilled tea before now.
Legal note: notwithstanding the above, we are a health science newsletter, not paramedics. Also, circumstances may differ, and best practices may change. In the case of serious injury, call emergency services first, and follow their instructions over ours.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: