Our blood-brain barrier stops bugs and toxins getting to our brain. Here’s how it works
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
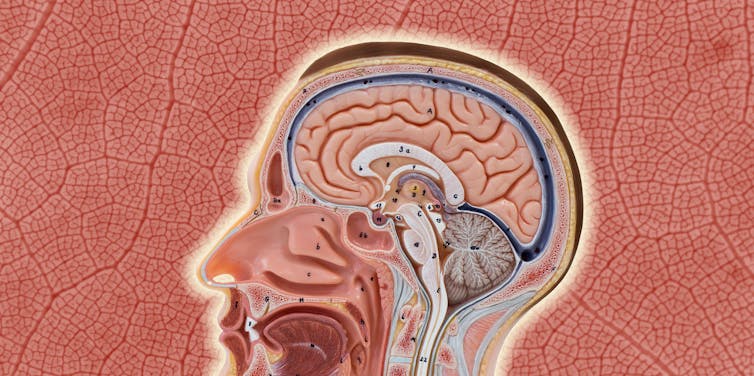
Our brain is an extremely complex and delicate organ. Our body fiercely protects it by holding onto things that help it and keeping harmful things out, such as bugs that can cause infection and toxins.
It does that though a protective layer called the blood-brain barrier. Here’s how it works, and what it means for drug design.
First, let’s look at the circulatory system
Adults have roughly 30 trillion cells in their body. Every cell needs a variety of nutrients and oxygen, and they produce waste, which needs to be taken away.
Our circulatory system provides this service, delivering nutrients and removing waste.
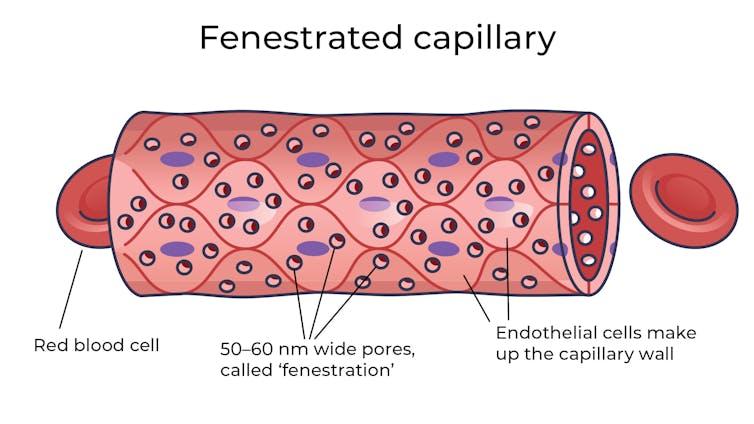
Where the circulatory system meets your cells, it branches down to tiny tubes called capillaries. These tiny tubes, about one-tenth the width of a human hair, are also made of cells.
But in most capillaries, there are some special features (known as fenestrations) that allow relatively free exchange of nutrients and waste between the blood and the cells of your tissues.
It’s kind of like pizza delivery
One way to think about the way the circulation works is like a pizza delivery person in a big city. On the really big roads (vessels) there are walls and you can’t walk up to the door of the house and pass someone the pizza.
But once you get down to the little suburban streets (capillaries), the design of the streets means you can stop, get off your scooter and walk up to the door to deliver the pizza (nutrients).
We often think of the brain as a spongy mass without much blood in it. In reality, the average brain has about 600 kilometres of blood vessels.
The difference between the capillaries in most of the brain and those elsewhere is that these capillaries are made of specialised cells that are very tightly joined together and limit the free exchange of anything dissolved in your blood. These are sometimes called continuous capillaries.

This is the blood brain barrier. It’s not so much a bag around your brain stopping things from getting in and out but more like walls on all the streets, even the very small ones.
The only way pizza can get in is through special slots and these are just the right shape for the pizza box.
The blood brain barrier is set up so there are specialised transporters (like pizza box slots) for all the required nutrients. So mostly, the only things that can get in are things that there are transporters for or things that look very similar (on a molecular scale).
The analogy does fall down a little bit because the pizza box slot applies to nutrients that dissolve in water. Things that are highly soluble in fat can often bypass the slots in the wall.
Why do we have a blood-brain barrier?
The blood brain barrier is thought to exist for a few reasons.
First, it protects the brain from toxins you might eat (think chemicals that plants make) and viruses that often can infect the rest of your body but usually don’t make it to your brain.
It also provides protection by tightly regulating the movement of nutrients and waste in and out, providing a more stable environment than in the rest of the body.
Lastly, it serves to regulate passage of immune cells, preventing unnecessary inflammation which could damage cells in the brain.
What it means for medicines
One consequence of this tight regulation across the blood brain barrier is that if you want a medicine that gets to the brain, you need to consider how it will get in.
There are a few approaches. Highly fat-soluble molecules can often pass into the brain, so you might design your drug so it is a bit greasy.

Another option is to link your medicine to another molecule that is normally taken up into the brain so it can hitch a ride, or a “pro-drug”, which looks like a molecule that is normally transported.
Using it to our advantage
You can also take advantage of the blood brain barrier.
Opioids used for pain relief often cause constipation. They do this because their target (opioid receptors) are also present in the nervous system of the intestines, where they act to slow movement of the intestinal contents.
Imodium (Loperamide), which is used to treat diarrhoea, is actually an opioid, but it has been specifically designed so it can’t cross the blood brain barrier.
This design means it can act on opioid receptors in the gastrointestinal tract, slowing down the movement of contents, but does not act on brain opioid receptors.
In contrast to Imodium, Ozempic and Victoza (originally designed for type 2 diabetes, but now popular for weight-loss) both have a long fat attached, to improve the length of time they stay in the body.
A consequence of having this long fat attached is that they can cross the blood-brain barrier, where they act to suppress appetite. This is part of the reason they are so effective as weight-loss drugs.
So while the blood brain barrier is important for protecting the brain it presents both a challenge and an opportunity for development of new medicines.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Joy Of Missing Out

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What this is not going to be: a sour grapes thing.
What this is going to be: an exploration of how the grass is greener
on the other side of the fencewherever you water itIt’s easy to feel lonely and isolated, even in today’s increasingly-connected world. We’ve tackled that topic before:
How To Beat Loneliness & Isolation
One of the more passive (but still reasonable) ways of reducing isolation is to simply say “yes” more, which we discussed (along with other more active strategies) here:
When The World Moves Without Us… Can We Side-Step Age-Related Alienation?
But, is there any benefit to be gained from not being in the thick of things?
Sometimes some things associated with isolation are not, in reality, necessarily isolating. See for example:
But, the implications of embracing the “joy of missing out” are much more wide-reaching:
Wherever you are, there you are
You’ve probably read before the phrase “wherever you go, there you are”, but this phrasing brings attention to the fact that you already are where you are.
There are quite possibly aspects of your current life/situation that are not ideal, but take a moment to appreciate where you are in life. At the very least, you are probably in a safe warm dry house with plenty of food available; chances are you have plenty of luxuries too.
See also: How To Get Your Brain On A More Positive Track (Without Toxic Positivity)
And yet, it’s easy to have a fear of missing out. Even billionaires fear they do not have enough and must acquire more in order to be truly secure and fulfilled.
As it goes for material wealth, so it also goes for social wealth—in other words, we may worry about such questions as: on whom can we rely, and who will be there for us if we need them? Do we, ultimately, have enough social capital to be secure?
- For social media influencers, it’ll be follower counts and engagement.
- For the family-oriented, it might be the question of whose house a given holiday gets celebrated at, and who attends, and who does it best.
- In more somber matters, think about funerals, and those where “there was such a huge turnout” vs “almost nobody attended”.
It sure sounds a lot like a dog-eat-dog world in which missing out sucks! But it doesn’t have to.
So let’s recap: your current situation is probably, all things considered, not bad. There is probably much in life to enjoy. If people do not come to your holiday event, then those are not people who would have improved things for you. If people do not attend your funeral even, then well, you yourself will be late, so hey.
Right now though, you are alive, so…
Enjoy the moment; enjoy your life for you.
Invest in yourself. Better yourself. Improve your environment for yourself little by little.
We spend a lot of time in life living up to everyone’s expectations, often without stopping to question whether it is what we want, or sometimes putting aside what we want in favor of what is wanted of us.
- Sometimes, such ostensible altruism is laudable and good (the point of today’s article is not “be a selfish jerk”; sometimes we should indeed shelve our self-interest in favour of doing something for the common good)
- Sometimes, it’s just pointless sacrifice that benefits nobody (the point of today’s article is “there is no point in playing stressful, stacked games when you could have a better time not doing that”)
If you are about to embark on an endeavor that you don’t really want to, take a moment to seriously consider which of the above two situations this is, and then act accordingly.
For a deeper dive into that, you might like this book that we reviewed a while back:
The Joy of Saying No – by Natalie Lue
Enjoy!
Share This Post
-

Solitary Fitness – by Charles Bronson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes it can seem that every new diet and/or exercise regime you want to try will change your life, if just you first max out your credit card on restocking your kitchen and refurbishing your home gym, not to mention buying all the best supplements, enjoying the latest medical gadgets, and so on and so forth.
And often… Most of those things genuinely are good! And it’s great that such things are becoming more accessible and available.
But… Wouldn’t it be nice to know how to have excellent strength and fitness without any of that, even if just as a “bare bones” protocol to fall back on? That’s what Manson provides in this book.
The writing style is casual and friendly; Manson is not exactly an academic, but he knows his stuff when it comes to what works. And a good general rule of thumb is: if it’s something that he can do in his jail cell, we can surely do it in the comfort of our homes.
Bottom line: if you want functional strength and fitness with zero gimmicks, this is the book for you (as an aside, it’s also simply an interesting and recommendable read, sociologically speaking, but that’s another matter entirely).
Share This Post
-

Your Brain on Art – by Susan Magsamen & Ivy Ross
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The notion of art therapy is popularly considered a little wishy-washy. As it turns out, however, there are thousands of studies showing its effectiveness.
Nor is this just a matter of self-expression. As authors Magsamen and Ross explore, different kinds of engagement with art can convey different benefits.
That’s one of the greatest strengths of this book: “this form of engagement with art will give these benefits, according to these studies”
With benefits ranging from reducing stress and anxiety, to overcoming psychological trauma or physical pain, there’s a lot to be said for art!
And because the book covers many kinds of art, if you can’t imagine yourself taking paintbrush to canvas, that’s fine too. We learn of the very specific cognitive benefits of coloring in mandalas (yes, really), of sculpting something terrible in clay, or even just of repainting the kitchen, and more. Each thing has its set of benefits.
The book’s main goal is to encourage the reader to cultivate what the authors call an aesthetic mindset, which involves four key attributes:
- a high level of curiosity
- a love of playful, open-ended exploration
- a keen sensory awareness
- a drive to engage in creative activities
And, that latter? It’s as a maker and/or a beholder. We learn about what we can gain just by engaging with art that someone else made, too.
Bottom line: come for the evidence-based cognitive benefits; stay for the childlike wonder of the universe. If you already love art, or have thought it’s just “not for you”, then this book is for you.
Click here to check out Your Brain On Art, and open up whole new worlds of experience!
Share This Post
-

Allen Carr’s Easy Way to Quit Emotional Eating – by Allen Carr
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed books before on quitting drinking; is this book about emotional eating so different?
There are overlaps, but important points of contrast, too. After all, alcohol and junk food are both often unhealthy coping mechanisms for other things, though:
- Alcohol has in principle the stronger grip (making it harder to give up)
- Junk food is so much easier to justify (making it harder to give up)
Author Allen Carr is of course most well-known for his debut book about quitting smoking, and he brings a lot of that expertise to bear on the slightly different beast that is emotional eating.
Focused on reframing quitting as being less about self-denial and more about self-liberation, he helps readers to understand that giving up a substance (in this case, junk food) does not mean giving up happiness—rather, it means finding happiness beyond it.
If this book has a downside, it’s that some parts can be a little repetitive, and it can sometimes seem like one of those “this book could have been an article” situations.
On the other hand, many people benefit from repeated messages to truly inculcate an idea, so this could be a positive for a lot of readers.
Bottom line: if you’ve tried to eat more healthily but find that you keep reaching for an unhealthy comfort food, then this book may make a difference that other methods didn’t.
Click here to check out The Easy Way To Quit Emotional Eating, and find your own freedom!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How can I stop overthinking everything? A clinical psychologist offers solutions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As a clinical psychologist, I often have clients say they are having trouble with thoughts “on a loop” in their head, which they find difficult to manage.
While rumination and overthinking are often considered the same thing, they are slightly different (though linked). Rumination is having thoughts on repeat in our minds. This can lead to overthinking – analysing those thoughts without finding solutions or solving the problem.
It’s like a vinyl record playing the same part of the song over and over. With a record, this is usually because of a scratch. Why we overthink is a little more complicated.
We’re on the lookout for threats
Our brains are hardwired to look for threats, to make a plan to address those threats and keep us safe. Those perceived threats may be based on past experiences, or may be the “what ifs” we imagine could happen in the future.
Our “what ifs” are usually negative outcomes. These are what we call “hot thoughts” – they bring up a lot of emotion (particularly sadness, worry or anger), which means we can easily get stuck on those thoughts and keep going over them.
However, because they are about things that have either already happened or might happen in the future (but are not happening now), we cannot fix the problem, so we keep going over the same thoughts.
Who overthinks?
Most people find themselves in situations at one time or another when they overthink.
Some people are more likely to ruminate. People who have had prior challenges or experienced trauma may have come to expect threats and look for them more than people who have not had adversities.
Deep thinkers, people who are prone to anxiety or low mood, and those who are sensitive or feel emotions deeply are also more likely to ruminate and overthink.

We all overthink from time to time, but some people are more prone to rumination.
BĀBI/UnsplashAlso, when we are stressed, our emotions tend to be stronger and last longer, and our thoughts can be less accurate, which means we can get stuck on thoughts more than we would usually.
Being run down or physically unwell can also mean our thoughts are harder to tackle and manage.
Acknowledge your feelings
When thoughts go on repeat, it is helpful to use both emotion-focused and problem-focused strategies.
Being emotion-focused means figuring out how we feel about something and addressing those feelings. For example, we might feel regret, anger or sadness about something that has happened, or worry about something that might happen.
Acknowledging those emotions, using self-care techniques and accessing social support to talk about and manage your feelings will be helpful.
The second part is being problem-focused. Looking at what you would do differently (if the thoughts are about something from your past) and making a plan for dealing with future possibilities your thoughts are raising.
But it is difficult to plan for all eventualities, so this strategy has limited usefulness.
What is more helpful is to make a plan for one or two of the more likely possibilities and accept there may be things that happen you haven’t thought of.
Think about why these thoughts are showing up
Our feelings and experiences are information; it is important to ask what this information is telling you and why these thoughts are showing up now.
For example, university has just started again. Parents of high school leavers might be lying awake at night (which is when rumination and overthinking is common) worrying about their young person.
Think of what the information is telling you.
TheVisualsYouNeed/ShutterstockKnowing how you would respond to some more likely possibilities (such as they will need money, they might be lonely or homesick) might be helpful.
But overthinking is also a sign of a new stage in both your lives, and needing to accept less control over your child’s choices and lives, while wanting the best for them. Recognising this means you can also talk about those feelings with others.
Let the thoughts go
A useful way to manage rumination or overthinking is “change, accept, and let go”.
Challenge and change aspects of your thoughts where you can. For example, the chance that your young person will run out of money and have no food and starve (overthinking tends to lead to your brain coming up with catastrophic outcomes!) is not likely.
You could plan to check in with your child regularly about how they are coping financially and encourage them to access budgeting support from university services.
Your thoughts are just ideas. They are not necessarily true or accurate, but when we overthink and have them on repeat, they can start to feel true because they become familiar. Coming up with a more realistic thought can help stop the loop of the unhelpful thought.
Accepting your emotions and finding ways to manage those (good self-care, social support, communication with those close to you) will also be helpful. As will accepting that life inevitably involves a lack of complete control over outcomes and possibilities life may throw at us. What we do have control over is our reactions and behaviours.
Remember, you have a 100% success rate of getting through challenges up until this point. You might have wanted to do things differently (and can plan to do that) but nevertheless, you coped and got through.
So, the last part is letting go of the need to know exactly how things will turn out, and believing in your ability (and sometimes others’) to cope.
What else can you do?
A stressed out and tired brain will be more likely to overthink, leading to more stress and creating a cycle that can affect your wellbeing.
So it’s important to manage your stress levels by eating and sleeping well, moving your body, doing things you enjoy, seeing people you care about, and doing things that fuel your soul and spirit.
Find ways to manage your stress levels.
antoniodiaz/ShutterstockDistraction – with pleasurable activities and people who bring you joy – can also get your thoughts off repeat.
If you do find overthinking is affecting your life, and your levels of anxiety are rising or your mood is dropping (your sleep, appetite and enjoyment of life and people is being negatively affected), it might be time to talk to someone and get some strategies to manage.
When things become too difficult to manage yourself (or with the help of those close to you), a therapist can provide tools that have been proven to be helpful. Some helpful tools to manage worry and your thoughts can also be found here.
When you find yourself overthinking, think about why you are having “hot thoughts”, acknowledge your feelings and do some future-focused problem solving. But also accept life can be unpredictable and focus on having faith in your ability to cope.

Kirsty Ross, Associate Professor and Senior Clinical Psychologist, Massey University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Apple Cider Vinegar vs Balsamic Vinegar – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing apple cider vinegar to balsamic vinegar, we picked the apple cider vinegar.
Why?
It’s close! And it’s a simple one today and they’re both great. Taking either for blood-sugar-balancing benefits is fine, as it’s the acidity that has this effect. But:
- Of the two, balsamic vinegar is the one more likely to contain more sugars, especially if it’s been treated in any fashion, and not by you, e.g. made into a glaze or even a reduction (the latter has no need to add sugar, but sometimes companies do because it is cheaper—so we recommend making your own balsamic vinegar reduction at home)
- Of the two, apple cider vinegar is the one more likely to contain “the mother”, that is to say, the part with extra probiotic benefits (but if the vinegar has been filtered, it won’t have this—it’s just more common to be able to find unfiltered apple cider vinegar, since it has more popular attention for its health benefits than balsamic vinegar does)
So, two wins for apple cider vinegar there.
Want to learn more?
You might like to read:
- 10 Ways To Balance Your Blood Sugars
- An Apple (Cider Vinegar) A Day…
- Apple Cider Vinegar vs Apple Cider Vinegar Gummies – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: