The Spectrum of Hope – by Dr. Gayatri Devi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about Dr. Devi’s work (See: “Alzheimer’s: The Bad News And The Good“) but she has plenty more to say than we could fit in an article.
The book is written for patients, family/carers, and clinicians—without getting deep into the science, which it is assumed clinicians will know. the general style of the book is pop-science, and it’s more about addressing the misconceptions around Alzheimer’s, rather than focusing on neurological features such as beta amyloid plaques and tau proteins and the like.
Dr. Devi explains a lot about the experience of Alzheimer’s—what to expect, or rather, what to know about in advance. Because, as she explains, there are a lot of different manifestations of Alzheimer’s that are all lumped under the same umbrella.
This means that a person could have negligible memory but perfect language and reasoning skills, or the other way around, or some other combination of symptoms showing up or not.
Which means that any plan for managing one’s Alzheimer’s needs to be adaptable and personalized, which is something Dr. Devi talks us through, too.
Bottom line: if you are a loved one has Alzheimer’s, or you just like to be prepared, this is a great book to prepare anybody for just that.
Click here to check out The Spectrum of Hope, and hold onto that hope!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Chronic Obstructive Pulmonary Disease (COPD) Is More Likely Than You Think

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chronic Obstructive Pulmonary Disease (COPD): More Likely Than You Think
COPD is not so much one disease, as rather a collection of similar (and often overlapping) diseases. The main defining characteristic is that they are progressive lung diseases. Historically the most common have been chronic bronchitis and emphysema, though Long COVID and related Post-COVID conditions appear to have been making inroads.
Lung cancer is generally considered separately, despite being a progressive lung disease, but there is crossover too:
COPD prevalence is increased in lung cancer, independent of age, sex and smoking history
COPD can be quite serious:
“But I don’t smoke”
Great! In fact we imagine our readership probably has disproportionately few smokers compared to the general population, being as we all are interested in our health.
But, it’s estimated that 30,000,000 Americans have COPD, and approximately half don’t know it. Bear in mind, the population of the US is a little over 340,000,000, so that’s a little under 9% of the population.
Click here to see a state-by-state breakdown (how does your state measure up?)
How would I know if I have it?
It typically starts like any mild respiratory illness. Likely shortness of breath, especially after exercise, a mild cough, and a frequent need to clear your throat.
Then it will get worse, as the lungs become more damaged; each of those symptoms might become stronger, as well as chest tightness and a general lack of energy.
Later stages, you guessed it, the same but worse, and—tellingly—weight loss.
The reason for the weight loss is because you are getting less oxygen per breath, making carrying your body around harder work, meaning you burn more calories.
What causes it?
Lots of things, with smoking being up at the top, or being exposed to a lot of second-hand smoke. Working in an environment with a lot of air pollution (for example, working around chemical fumes) can cause it, as can inhaling dust. New Yorkers: yes, that dust too. It can also develop from other respiratory illnesses, and some people even have a genetic predisposition to it:
Alpha-1 antitrypsin deficiency: a commonly overlooked cause of lung disease
Is it treatable?
Treatment varies depending on what form of it you have, and most of the medical interventions are beyond the scope of this article. Suffice it to say, there are medications that can be taken (including bronchodilators taken via an inhaler device), corticosteroids, antibiotics and antivirals of various kinds if appropriate. This is definitely a “see your doctor” item though, because there are is far too much individual variation for us to usefully advise here.
However!
There are habits we can do to a) make COPD less likely and b) make COPD at least a little less bad if we get it.
Avoiding COPD:
- Don’t smoke. Just don’t.
- Avoid second-hand smoke if you can
- Avoid inhaling other chemicals/dust that may be harmful
- Breathe through your nose, not your mouth; it filters the air in a whole bunch of ways
- Seriously, we know it seems like nostril hairs surely can’t do much against tiny particles, but tiny particles are attracted to them and get stuck in mucous and dealt with by our immune system, so it really does make a big difference
Managing COPD:
- Continue the above things, of course
- Exercise regularly, even just light walking helps; we realize it will be difficult
- Maintain a healthy weight if you can
- This means both ways; COPD causes weight loss and that needs to be held in check. But similarly, you don’t want to be carrying excessive weight either; that will tire you even more.
- Look after the rest of your health; everything else will now hit you harder, so even small things need to be taken seriously
- If you can, get someone to help / do your household cleaning for you, ideally while you are not in the room.
Where can I get more help/advice?
As ever, speak to your doctor if you are concerned this may be affecting you. You can also find a lot of resources via the COPD Foundation’s website.
Take care of yourself!
Share This Post
- Don’t smoke. Just don’t.
-

Dietary Changes for Artery Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝How does your diet change clean out your arteries of the bad cholesterol?❞
There’s good news and bad news here, and they can both be delivered with a one-word reply:
Slowly.
Or rather: what’s being cleaned out is mostly not the LDL (bad) cholesterol, but rather, the result of that.
When our diet is bad for cardiovascular health, our arteries get fatty deposits on their walls. Cholesterol gets stuck here too, but that’s not the main physical problem.
Our body’s natural defenses come into action and try to clean it up, but they (for example macrophages, a kind of white blood cell that consumes invaders and then dies, before being recycled by the next part of the system) often get stuck and become part of the buildup (called atheroma), which can lead to atherosclerosis and (if calcium levels are high) hardening of the arteries, which is the worst end of this.
This can then require medical attention, precisely because the body can’t remove it very well—especially if you are still maintaining a heart-unhealthy diet, thus continuing to add to the mess.
However, if it is not too bad yet, yes, a dietary change alone will reverse this process. Without new material being added to the arterial walls, the body’s continual process of rejuvenation will eventually fix it, given time (free from things making it worse) and resources.
In fact, your arteries can be one of the quickest places for your body to make something better or worse, because the blood is the means by which the body moves most things (good or bad) around the body.
All the more reason to take extra care of it, since everything else depends on it!
You might also like our previous main feature:
Share This Post
-

Overcome Front-Of-Hip Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Alyssa Kuhn, physiotherapist, demonstrates how:
One, two, three…
One kind of pain affects a lot of related things: hip pain has an impact on everything that’s connected to the pelvis, which is basically the rest of the body, but especially the spine itself. For this reason, it’s critical to keep it in as good condition as possible.
Two primary causes of hip stiffness and pain:
- Anterior pelvic tilt due to posture, weight distribution, or pain. This tightens the front muscles and weakens the back muscles.
- Prolonged sitting, which tightens the hip muscles due to inactivity.
Three exercises are recommended by Dr. Kuhn to relieve pain and stiffness:
- Bridge exercise:
- Lie on a firm surface with your knees bent.
- Push through your feet, engage your hamstrings, and flatten your lower back.
- Hold for 3–5 seconds, relax, and repeat (10–20 reps).
- Wall exercise with arms:
- Stand with your lower back against the wall, feet a step away.
- Tilt your hips backwards, keeping your lower back in contact with the wall.
- Alternate lifting one arm at a time while maintaining back contact with the wall (10–20 reps).
- Wall exercise with legs:
- Same stance as the previous exercise but wider now.
- Lift one heel at a time while keeping your hips stable and your back against the wall.
- Practice for 30–60 seconds, maintaining good form.
As ever, consistency is key for long-term relief. Dr. Kuhn recommends doing these regularly, especially before any expected periods of prolonged sitting (e.g. at desk, or driving, etc). And of course, do try to reduce, or at least break up, those sitting marathons if you can.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post
Related Posts
-
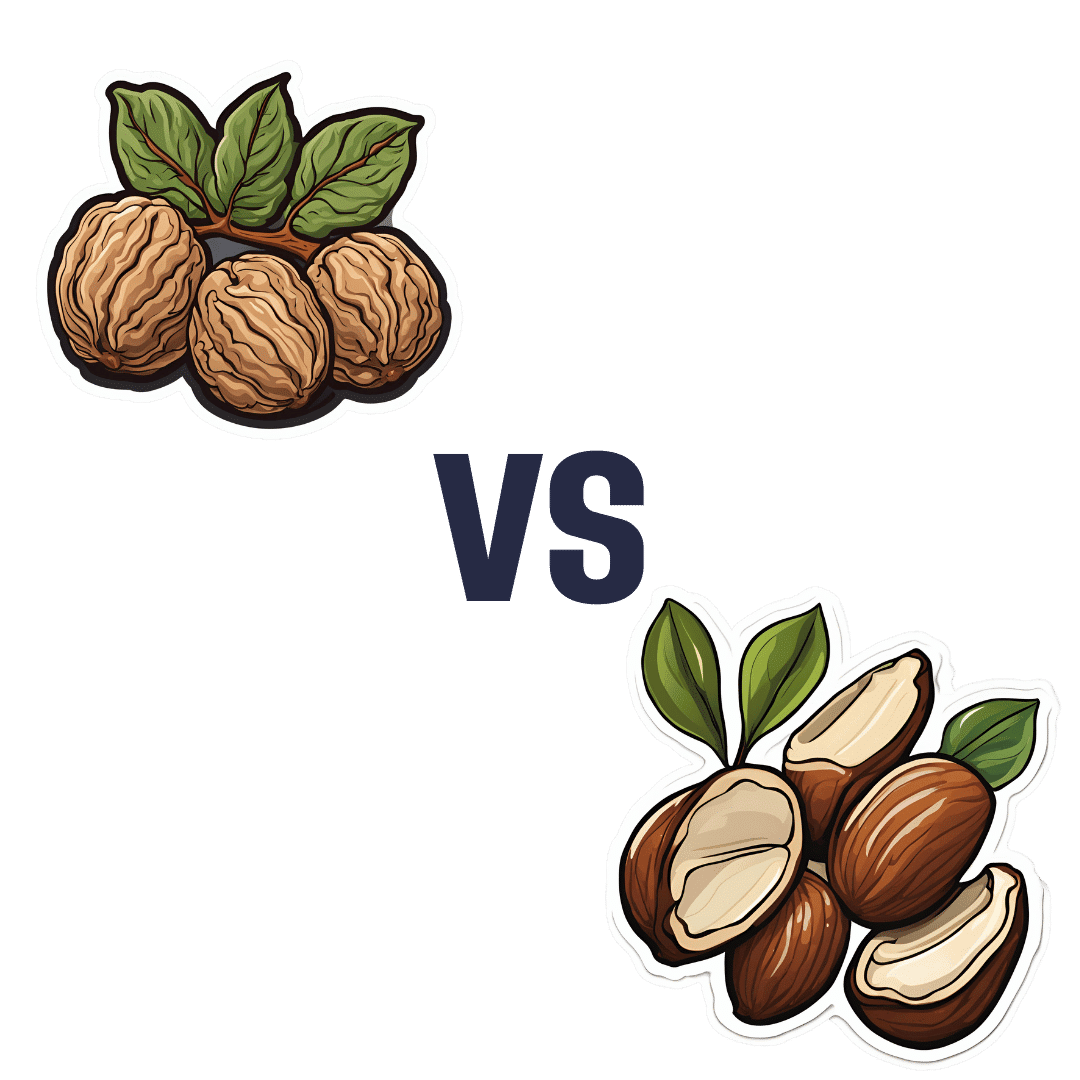
Walnuts vs Brazil Nuts – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing walnuts to Brazil nuts, we picked the walnuts.
Why?
Talking macros first, they are about equal in protein, carbs, fats, and fiber; their composition is almost identical in this regard. However, looking a little more closely at the fats, Brazil nuts have more than 2x the saturated fat, while walnuts have nearly 2x the polyunsaturated fat. So, we’ll declare the macros category a moderate win for walnuts.
The category of vitamins is not balanced; walnuts have more of vitamins A, B2, B3, B5, B6, B9, C, and choline, while Brazil nuts have more of vitamins B1 and E. A clear and easy win for walnuts.
The category of minerals is interesting, because of one mineral in particular. First let’s mention: walnuts have more iron and manganese, while Brazil nuts have more calcium, copper, magnesium, phosphorus, potassium, and selenium. Taken at face value, this is a clear win for Brazil nuts. However…
About that selenium… Specifically, it’s more than 391x higher, and a cup of Brazil nuts would give nearly 10,000x the recommended daily amount of selenium. Now, selenium is an essential mineral (needed for thyroid hormone production, for example), and at the RDA it’s good for good health. Your hair will be luscious and shiny. However, go much above that, and selenium toxicity becomes a thing, you may get sick, and it can cause your (luscious and shiny) hair to fall out. For this reason, it’s recommended to eat no more than 3–4 Brazil nuts per day.
There is one last consideration, and this is oxalates; walnuts are moderately high in oxalates (>50mg/100g) while Brazil nuts are very high in oxalates (>500mg/100g). This won’t affect most people at all, but if you have pre-existing kidney problems (including a history of kidney stones), you might want to go easy on oxalate-containing foods.
For most people, however, walnuts are a very healthy choice, and outshine Brazil nuts in most ways.
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Prolonged Grief: A New Mental Disorder?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The issue is not whether certain mental conditions are real—they are. It is how we conceptualize them and what we think treating them requires.
The latest edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) features a new diagnosis: prolonged grief disorder—used for those who, a year after a loss, still remain incapacitated by it. This addition follows more than a decade of debate. Supporters argued that the addition enables clinicians to provide much-needed help to those afflicted by what one might simply consider a too much of grief, whereas opponents insisted that one mustn’t unduly pathologize grief and reject an increasingly medicalized approach to a condition that they considered part of a normal process of dealing with loss—a process which in some simply takes longer than in others.
By including a condition in a professional classification system, we collectively recognize it as real. Recognizing hitherto unnamed conditions can help remove certain kinds of disadvantages. Miranda Fricker emphasizes this in her discussion of what she dubs hermeneutic injustice: a specific sort of epistemic injustice that affects persons in their capacity as knowers1. Creating terms like ‘post-natal depression’ and ‘sexual harassment’, Fricker argues, filled lacunae in the collectively available hermeneutic resources that existed where names for distinctive kinds of social experience should have been. The absence of such resources, Fricker holds, put those who suffered from such experiences at an epistemic disadvantage: they lacked the words to talk about them, understand them, and articulate how they were wronged. Simultaneously, such absences prevented wrong-doers from properly understanding and facing the harm they were inflicting—e.g. those who would ridicule or scold mothers of newborns for not being happier or those who would either actively engage in sexual harassment or (knowingly or not) support the societal structures that helped make it seem as if it was something women just had to put up with.
For Fricker, the hermeneutical disadvantage faced by those who suffer from an as-of-yet ill-understood and largely undiagnosed medical condition is not an epistemic injustice. Those so disadvantaged are not excluded from full participation in hermeneutic practices, or at least not through mechanisms of social coercion that arise due to some structural identity prejudice. They are not, in other words, hermeneutically marginalized, which for Fricker, is an essential characteristic of epistemic injustice. Instead, their situation is simply one of “circumstantial epistemic bad luck”2. Still, Fricker, too, can agree that providing labels for ill-understood conditions is valuable. Naming a condition helps raise awareness of it, makes it discursively available and, thus, a possible object of knowledge and understanding. This, in turn, can enable those afflicted by it to understand their experience and give those who care about them another way of nudging them into seeking help.
Surely, if adding prolonged grief disorder to the DSM-5 were merely a matter of recognizing the condition and of facilitating assistance, nobody should have any qualms with it. However, the addition also turns intense grief into a mental disorder—something for whose treatment insurance companies can be billed. With this, significant forces of interest enter the scene. The DSM-5, recall, is mainly consulted by psychiatrists. In contrast to talk-therapists like psychotherapists or psychoanalysts, psychiatrists constitute a highly medicalized profession, in which symptoms—clustered together as syndromes or disorders—are frequently taken to require drugs to treat them. Adding prolonged grief disorder thus heralds the advent of research into various drug-based grief therapies. Ellen Barry of the New York Times confirms this: “naltrexone, a drug used to help treat addiction,” she reports, “is currently in clinical trials as a form of grief therapy”, and we are likely to see a “competition for approval of medicines by the Food and Drug Administration.”3
Adding diagnoses to the DSM-5 creates financial incentives for players in the pharmaceutical industry to develop drugs advertised as providing relief to those so diagnosed. Surely, for various conditions, providing drug-induced relief from severe symptoms is useful, even necessary to enable patients to return to normal levels of functioning. But while drugs may help suppress feelings associated with intense grief, they cannot remove the grief. If all mental illnesses were brain diseases, they might be removed by adhering to some drug regimen or other. Note, however, that ‘mental illness’ is a metaphor that carries the implicit suggestion that just like physical illnesses, mental afflictions, too, are curable by providing the right kind of physical treatment. Unsurprisingly, this metaphor is embraced by those who stand to massively benefit from what profits they may reap from selling a plethora of drugs to those diagnosed with any of what seems like an ever-increasing number of mental disorders. But metaphors have limits. Lou Marinoff, a proponent of philosophical counselling, puts the point aptly:
Those who are dysfunctional by reason of physical illness entirely beyond their control—such as manic-depressives—are helped by medication. For handling that kind of problem, make your first stop a psychiatrist’s office. But if your problem is about identity or values or ethics, your worst bet is to let someone reify a mental illness and write a prescription. There is no pill that will make you find yourself, achieve your goals, or do the right thing.
Much more could be said about the differences between psychotherapy, psychiatry, and the newcomer in the field: philosophical counselling. Interested readers may benefit from consulting Marinoff’s work. Written in a provocative, sometimes alarmist style, it is both entertaining and—if taken with a substantial grain of salt—frequently insightful. My own view is this: from Fricker’s work, we can extract reasons to side with the proponents of adding prolonged grief disorder to the DSM-5. Creating hermeneutic resources that allow us to help raise awareness, promote understanding, and facilitate assistance is commendable. If the addition achieves that, we should welcome it. And yet, one may indeed worry that practitioners are too eager to move from the recognition of a mental condition to the implementation of therapeutic interventions that are based on the assumption that such afflictions must be understood on the model of physical disease. The issue is not whether certain mental conditions are real—they are. It is how we conceptualize them and what we think treating them requires.
No doubt, grief manifests physically. It is, however, not primarily a physical condition—let alone a brain disease. Grief is a distinctive mental condition. Apart from bouts of sadness, its symptoms typically include the loss of orientation or a sense of meaning. To overcome grief, we must come to terms with who we are or can be without the loved one’s physical presence in our life. We may need to reinvent ourselves, figure out how to be better again and whence to derive a new purpose. What is at stake is our sense of identity, our self-worth, and, ultimately, our happiness. Thinking that such issues are best addressed by popping pills puts us on a dangerous path, leading perhaps towards the kind of dystopian society Aldous Huxley imagined in his 1932 novel Brave New World. It does little to help us understand, let alone address, the moral and broader philosophical issues that trouble the bereaved and that lie at the root not just of prolonged grief but, arguably, of many so-called mental illnesses.
Footnotes:
1 For this and the following, cf. Fricker 2007, chapter 7.
2 Fricker 2007: 152
3 Barry 2022
References:
Barry, E. (2022). “How Long Should It Take to Grieve? Psychiatry Has Come Up With an Answer.” The New York Times, 03/18/2022, URL = https://www.nytimes.com/2022/03/18/health/prolonged-grief-
disorder.html [last access: 04/05/2022])
Fricker, M. (2007). Epistemic Injustice. Power & the Ethics of knowing. Oxford/New York: Oxford University Press.
Huxley, A. (1932). Brave New World. New York: Harper Brothers.
Marinoff, L. (1999). Plato, not Prozac! New York: HarperCollins Publishers.Professor Raja Rosenhagen is currently serving as Assistant Professor of Philosophy, Head of Department, and Associate Dean of Academic Affairs at Ashoka University. He earned his PhD in Philosophy from the University of Pittsburgh and has a broad range of philosophical interests (see here). He wrote this article a) because he was invited to do so and b) because he is currently nurturing a growing interest in philosophical counselling.
This article is republished from OpenAxis under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Sweet Truth About Glycine
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Make Your Collagen Work Better

This is Dr. James Nicolantonio. He’s a doctor of pharmacy, and a research scientist. He has a passion for evidence-based nutrition, and has written numerous books on the subject.
Controversy! Dr. DiNicolatonio’s work has included cardiovascular research, in which field he has made the case for increasing (rather than decreasing) the recommended amount of salt in our diet. This, of course, goes very much against the popular status quo.
We haven’t reviewed that research so we won’t comment on it here, but we thought it worth a mention as a point of interest. We’ll investigate his claims in that regard another time, though!
Today, however, we’ll be looking at his incisive, yet not controversial, work pertaining to collagen and glycine.
A quick recap on collagen
We’ve written about collagen before, and its importance for maintaining… Well, pretty much most of our body, really, buta deficiency in collagen can particularly weaken bones and joints.
On a more surface level, collagen’s also important for healthy elastic skin, and many people take it for that reason alone,
Since collagen is found only in animals, even collagen supplements are animal-based (often marine collagen or bovine collagen). However, if we don’t want to consume those, we can (like most animals) synthesize it ourselves from the relevant amino acids, which we can get from plants (and also laboratories, in some cases).
You can read our previous article about this, here:
We Are Such Stuff As Fish Are Made Of
What does he want us to know about collagen?
We’ll save time and space here: first, he’d like us to know the same as what we said in our article above
However, there is also more:
Let’s assume that your body has collagen to process. You either consumed it, or your body has synthesized it. We’ll skip describing the many steps of collagen synthesis, fascinating as that is, and get to the point:
When our body weaves together collagen fibrils out of the (triple-helical) collagen molecules…
- the cross-linking of the collagen requires lysyl oxidase
- the lysyl oxidase (which we make inside us) deanimates some other amino acids yielding aldehydes that allow the stable cross-links important for the high tensile strength of collagen, but to do that, it requires copper
- in order to use the copper it needs to be in its reduced cuprous form and that requires vitamin C
- but moving it around the body requires vitamin A
So in other words: if you are taking (or synthesizing) collagen, you also need copper and vitamins A and C.
However! Just to make things harder, if you take copper and vitamin C together, it’ll reduce the copper too soon in the wrong place.
Dr. DiNicolantonio therefore advises taking vitamin C after copper, with a 75 minutes gap between them.
What does he want us to know about glycine?
Glycine is one of the amino acids that makes up collagen. Specifically, it makes up every third amino acid in collagen, and even more specifically, it’s also the rate-limiting factor in the formation of glutathione, which is a potent endogenous (i.e., we make it inside us) antioxidant that works hard to fight inflammation inside the body.
What this means: if your joints are prone to inflammation, being glycine-deficient means a double-whammy of woe.
As well as being one of the amino acids most key to collagen production, glycine has another collagen-related role:
First, the problem: as we age, glycated collagen accumulates in the skin and cartilage (that’s bad; there is supposed to be collagen there, but not glycated).
More on glycation and what it is and why it is so bad:
Are You Eating Advanced Glycation End-Products? The Trouble Of The AGEs
Now, the solution: glycine suppresses advanced glycation end products, including the glycation of collagen.
See for example:
With these three important functions of glycine in mind…
Dr. DiNicolantonio therefore advises getting glycine at a dose of 100mg/kg/day. So, if you’re the same size as this rather medium-sized writer, that means 7.2g/day.
Where can I get it?
Glycine is found in many foods, including gelatin for those who eat that, eggs for the vegetarians, and spinach for vegans.
However, if you’d like to simply take it as a supplement, here’s an example product on Amazon
(the above product is not clear whether it’s animal-derived or not, so if that’s important to you, shop around. This writer got some locally that is certified vegan, but is in Europe rather than N. America, which won’t help most of our subscribers)
Note: pure glycine is a white crystalline powder that has the same sweetness as glucose. Indeed, that is how it got its name, from the Greek “γλυκύς”, pronounced /ɡly.kýs/, meaning “sweet”. Yes, same etymology as glucose.
So don’t worry that you’ve been conned if you order it and think “this is sugar!”; it just looks and tastes the same.
That does mean you should buy from a reputable source though, as a con would be very easy!
this does also mean that if you like a little sugar/sweetener in your tea or coffee, glycine can be used as a healthy substitute.
If you don’t like sweet tastes, then, condolences. This writer pours two espresso coffees (love this decaffeinated coffee that actually tastes good), puts the glycine in the first, and then uses the second to get rid of the sweet taste of the first. So that’s one way to do it.
Enjoy (if you can!)
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: