Yoga that Helps You on the Loo
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How This Video Helps You Poo
When you’re feeling a bit bloated, Yoga With Bird’s 10-minute yoga routine promises to help you release…your gas. And, perhaps, more.
From a tabletop flow to soothing twists, each pose allows you to sync your breath with movement, helping to promote organic relief.
With options to modify with pillows for extra support, this video (below) caters to everyone needing a digestive reset.
Other Toilet Tricks
If yoga isn’t your thing, or you’re interested in trying to use different methods to make your visits to the bathroom a bit easier, we’ve spoken about the ways to manage gut health, and use of probiotics or fiber, and even the prevention of hemorrhoids.
Namaste and goodbye to bloat!
How was the video? If you’ve discovered any great videos yourself that you’d like to share with fellow 10almonds readers, then please do email them to us!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Early Bird Or Night Owl? Genes vs Environment

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Sliding Slope?

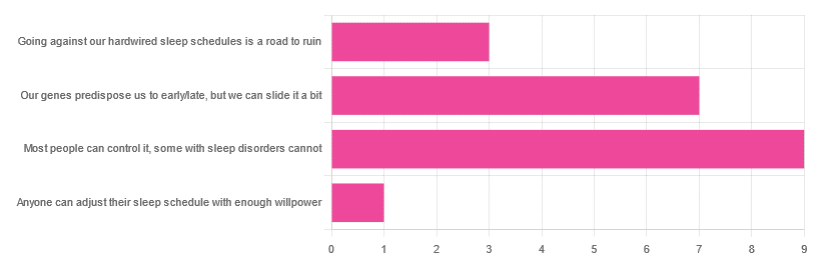
In Tuesday’s newsletter, we asked you how much control you believe we have over our sleep schedule, and got the above-depicted, below-described, set of responses:
- 45% said “most people can control it; some people with sleep disorders cannot
- 35% said “our genes predispose us to early/late, but we can slide it a bit
- 15% said: “going against our hardwired sleep schedules is a road to ruin”
- 5% said “anyone can adjust their sleep schedule with enough willpower”
You may be wondering: what’s with those single-digit numbers in the graph there? And the answer is: Tuesday’s email didn’t go out at the usual time due to a scheduling mistake (sorry!), which is probably what affected the number of responses (poll response levels vary, but are usually a lot higher than this).
Note: yes, this does mean most people who read our newsletter don’t vote. So, not to sound like a politician on the campaign trail, but… Your vote counts! We always love reading your comments when you add those, too—often they provide context that allow us to tailor what we focus on in our articles
However, those are the responses we got, so here we are!
What does the science say?
Anyone can adjust their sleep with enough willpower: True or False?
False, simply. It’s difficult for most people, but for many people with sleep disorders, it is outright impossible.
In a battle of narcolepsy vs willpower, for example, no amount of willpower will stop the brain from switching to sleep mode when it thinks it’s time to sleep:
❝Narcolepsy is the most common neurological cause of chronic sleepiness. The discovery about 20 years ago that narcolepsy is caused by selective loss of the neurons producing orexins sparked great advances in the field
[There is also] developing evidence that narcolepsy is an autoimmune disorder that may be caused by a T cell-mediated attack on the orexin neurons and explain how these new perspectives can inform better therapeutic approaches.❞
~ Dr. Carrie Mahoney et al. (lightly edited for brevity)
Source: The neurobiological basis of narcolepsy
For further reading, especially if this applies to you or a loved one:
Our genes predispose us to early/late, but we can slide it a bit: True or False?
True! First, about our genes predisposing us:
…and also:
Gene distinguishes early birds from night owls and helps predict time of death
Now, as for the “can slide it a bit”, this is really just a function of the general categories of “early bird” and “night owl” spanning periods of time that allow for a few hours’ wiggle-room at either side.
However, it is recommended to make any actual changes more gradually, with the Sleep Foundation going so far as to recommend 30 minutes, or even just 15 minutes, of change per day:
Sleep Foundation | How to Fix Your Sleep Schedule
Going against our hardwired sleep schedule is a road to ruin: True or False?
False, contextually. By this we mean: our “hardwired” sleep schedule is (for most of us), genetically predisposed but not predetermined.
Also, genetic predispositions are not necessarily always good for us; one would not argue, for example, for avoiding going against a genetic predisposition to addiction.
Some genetic predispositions are just plain bad for us, and genes can be a bit of a lottery.
That said, we do recommend getting some insider knowledge (literally), by getting personal genomics tests done, if that’s a viable option for you, so you know what’s really a genetic trait (and what to do with that information) and what’s probably caused by something else (and what to do with that information):
Genetic Testing: Health Benefits & Methods
Take care!
Share This Post
-

Good to Go – by Christie Aschwanden
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many of us may more often need to recover from a day of moving furniture than running a marathon, but the science of recovery can still teach us a lot. The author, herself an endurance athlete and much-decorated science journalist, sets out to do just that.
She explores a lot of recovery methods, and examines whether the science actually backs them up, and if so, to what degree. She also, in true science journalism style, talks to a lot of professionals ranging from fellow athletes to fellow scientists, to get their input too—she is nothing if not thorough, and this is certainly not a book of one person’s opinion with something to sell.
Indeed, on the contrary, her findings show that some of the best recovery methods are the cheapest, or even free. She also looks at the psychological aspect though, and why many people are likely to continue with things that objectively do not work better than placebo.
The style is very easy-reading jargon-free pop-science, while nevertheless being backed up with hundreds of studies cited in the bibliography—a perfect balance of readability and reliability.
Bottom line: for those who wish to be better informed about how to recover quickly and easily, this book is a treasure trove of information well-presented.
Click here to check out Good To Go, and always be good to go!
Share This Post
-

Astaxanthin: Super-Antioxidant & Neuroprotectant
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Think Pink For Brain Health!
Astaxanthin is a carotenoid that’s found in:
- certain marine microalgae
- tiny crustaceans that eat the algae
- fish (and flamingos!) that eat the crustaceans
Yes, it’s the one that makes things pink.
But it does a lot more than that…
Super-antioxidant
Move over, green tea! Astaxanthin has higher antioxidant activity than most carotenoids. For example, it is 2–5 times more effective than alpha-carotene, lutein, beta-carotene, and lycopene:
Antioxidant activities of astaxanthin and related carotenoids
We can’t claim credit for naming it a super-antioxidant though, because:
Astaxanthin: A super antioxidant from microalgae and its therapeutic potential
Grow new brain cells
Axtaxanthin is a neuroprotectant, but that’s to be expected from something with such a powerful antioxidant ability.
What’s more special to astaxanthin is that it assists continued adult neurogenesis (creation of new brain cells):
❝The unique chemical structure of astaxanthin enables it to cross the blood-brain barrier and easily reach the brain, where it may positively influence adult neurogenesis.
Furthermore, astaxanthin appears to modulate neuroinflammation by suppressing the NF-κB pathway, reducing the production of pro-inflammatory cytokines, and limiting neuroinflammation associated with aging and chronic microglial activation.
By modulating these pathways, along with its potent antioxidant properties, astaxanthin may contribute to the restoration of a healthy neurogenic microenvironment, thereby preserving the activity of neurogenic niches during both normal and pathological aging. ❞
That first part is very important, by the way! There are so many things that our brain needs, and we can eat, but the molecules are unable to pass the blood-brain barrier, meaning they either get wasted, or used elsewhere, or dismantled for their constituent parts. In this case, it zips straight into the brain instead.
See also:
How To Grow New Brain Cells (At Any Age)
(Probably) good for the joints, too
First, astaxanthin got a glowing report in a study we knew not to trust blindly:
…and breathe. What a title that was! But, did you catch why it’s not to be trusted blindly? It was down at the bottom…
❝Conflict of interest statement
NOVAREX Co., Ltd. funded the study. Valensa International provided the FlexPro MD® ingredients, and NOVAREX Co., Ltd. encapsulated the test products (e.g., both FlexPro MD® and placebo)❞
Studies where a supplement company funded the study are not necessarily corrupt, but they can certainly sway publication bias, i.e. the company funds a bunch of studies and then pulls funding from the ones that aren’t going the way it wants.
So instead let’s look at:
Astaxanthin attenuates joint inflammation induced by monosodium urate crystals
and
Astaxanthin ameliorates cartilage damage in experimental osteoarthritis
…which had no such conflicts of interest.
They agree that astaxanthin indeed does the things (attenuates joint inflammation & ameliorates cartilage damage).
However, they are animal studies (rats), so we’d like to see studies with humans to be able to say for sure how much it helps these things.
Summary of benefits
Based on the available research, astaxanthin…
- is indeed a super-antioxidant
- is a neuroprotective agent
- also assists adult neurogenesis
- is probablygood for joints too
How much do I take, and is it safe?
A 2019 safety review concluded:
❝Recommended or approved doses varied in different countries and ranged between 2 and 24 mg.
We reviewed 87 human studies, none of which found safety concerns with natural astaxanthin supplementation, 35 with doses ≥12 mg/day.❞
Source: Astaxanthin: How much is too much? A safety review
In short: for most people, it’s very safe and well-tolerated. If you consume it to an extreme, you will likely turn pink, much as you would turn orange if you did the same thing with carrots. But aside from that, the risks appear to be minimal.
However! If you have a seafood allergy, please take care to get a supplement that’s made from microalgae, not one that’s made from krill or other crustaceans, or from other creatures that eat those.
Where can I get it?
We don’t sell it, but here’s an example product on Amazon, for your convenience
Enjoy!
Share This Post

Related Posts
-

White Beans vs Pinto Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing white beans to pinto beans, we picked the pinto beans.
Why?
Both are good and both have their strengths! But we say the pinto beans come out on top in total:
In terms of macros, the two beans are about equal in protein and carbs, while pinto beans have notably more fiber. White beans were already good, but we say having 1.5x the fiber makes pinto beans the winner in this category.
In the category of vitamins, white beans are not higher in any vitamins, while pinto beans have more of vitamins B1, B2, B3, B6, B7, B9, and C, making for a 7:0 win for pinto beans. It’s worth mentioning that both beans are equal in vitamins B5, E, K, and choline, though. Still, pinto beans win easily on the strength of those 7 vitamins they have more of.
When it comes to minerals, white beans have more calcium, copper, iron, magnesium, manganese, potassium, and zinc, while pinto beans have more phosphorus and selenium, making for a win for white beans this time.
Adding up the sections makes for an overall win for pinto beans, but by all means, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Not to Age – by Dr. Michael Greger
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First things first: it’s a great book, and it’s this reviewer’s favorite of Dr. Greger’s so far (for posterity: it’s just been published and this reviewer has just finished reading the copy she got on pre-order)
Unlike many popular physician authors, Dr. Greger doesn’t rehash a lot of old material, and instead favours prioritizing new material in each work. Where appropriate, he’ll send the reader to other books for more specific information (e.g: you want to know how to avoid premature death? Go read How Not To Die. You want to know how to lose weight? How Not To Diet. Etc).
In the category of new information, he has a lot to offer here. And with over 8,000 references, it’s information, not conjecture. On which note, we recommend the e-book version if that’s possible for you, for three reasons:
- It’s possible to just click the references and be taken straight to the cited paper itself online
- To try to keep the book’s size down, Dr. Greger has linked to other external resources too
- The only negative reviews on Amazon, so far, are people complaining that the print copy’s text is smaller than they’d like
For all its information-density (those 8,000+ references are packed into 600ish pages), the book is very readable even to a lay reader; the author is a very skilled writer.
As for the content, we can’t fit more than a few sentences here so forgive the brevity, but we’ll mention that he covers:
- Slowing 11 pathways of aging
- The optimal anti-aging regimen according to current best science
- Preserving function (specific individual aspects of aging, e.g. hearing, sight, cognitive function, sexual function, hair, bones, etc)
- “Dr. Greger’s Anti-Aging Eight”
In terms of “flavor” of anti-aging science, his approach can be summed up as: diet and lifestyle as foundation; specific supplements and interventions as cornerstones.
Bottom line: this is now the anti-aging book.
Click here to check out How Not To Age, and look after yourself with the best modern science!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hazelnuts vs Almonds – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing hazelnuts to almonds, we picked the almonds.
Why?
It’s closer than you might think! But we say almonds do come out on top.
In terms of macronutrients, almonds have notably more protein, while hazelnuts have notably more fat (healthy fats, though). Almonds are also higher in both carbs and fiber. Looking at Glycemic Index, hazelnuts’ GI is low and almonds’ GI is zero. We could call the macros category a tie, but ultimately if we need to prioritize any of these things, it’s protein and fiber, so we’ll call this a nominal win for almonds.
When it comes to vitamins, hazelnuts have more of vitamins B1, B5, B6, B9 C, and K. Meanwhile, almonds have more of vitamins B2, B3, E, and choline. So, a moderate win for hazelnuts.
In the category of minerals, almonds retake the lead with more calcium, magnesium, phosphorus, potassium, selenium, and zinc, while hazelnuts boast more copper and manganese. A clear win for almonds.
Adding up the categories, this makes for a marginal win for almonds. Of course, both of these nuts are very healthy (assuming you are not allergic), and best is to enjoy both if possible.
Want to learn more?
You might like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: