The Distracted Mind – by Dr. Adam Gazzaley and Dr. Larry Rosen
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Yes, yes, we know, unplug once in a while. But what else do this highly-qualified pair of neuroscientists have to offer?
Rather than being a book for the sake of being a book, with lots of fluff and the usual advice about single-tasking, the authors start with a reframe:
Neurologically speaking, the hit of dopamine we get when looking for information is the exact same as the hit of dopamine that we, a couple of hundred thousand years ago, got when looking for nuts and berries.
- When we don’t find them, we become stressed, and search more.
- When we do find them, we are encouraged and search more nearby, and to the other side of nearby, and near around, to find more.
But in the case of information (be it useful information or celebrity gossip or anything in between), the Internet means that’s always available now.
So, we jitter around like squirrels, hopping from one to the next to the next.
A strength of this book is where it goes from there. Specifically, what evidence-based practices will actually keep our squirrel-brain focused… and which are wishful thinking for anyone who lives in this century.
Bringing original research from their own labs, as well as studies taken from elsewhere, the authors present a science-based toolkit of genuinely useful resources for actual focus.
Bottom line: if you think you could really optimize your life if you could just get on track and stay on track, this is the book for you.
Click here to check out The Distracted Mind, and get yours to focus!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

10almonds Tells The Tea…

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!

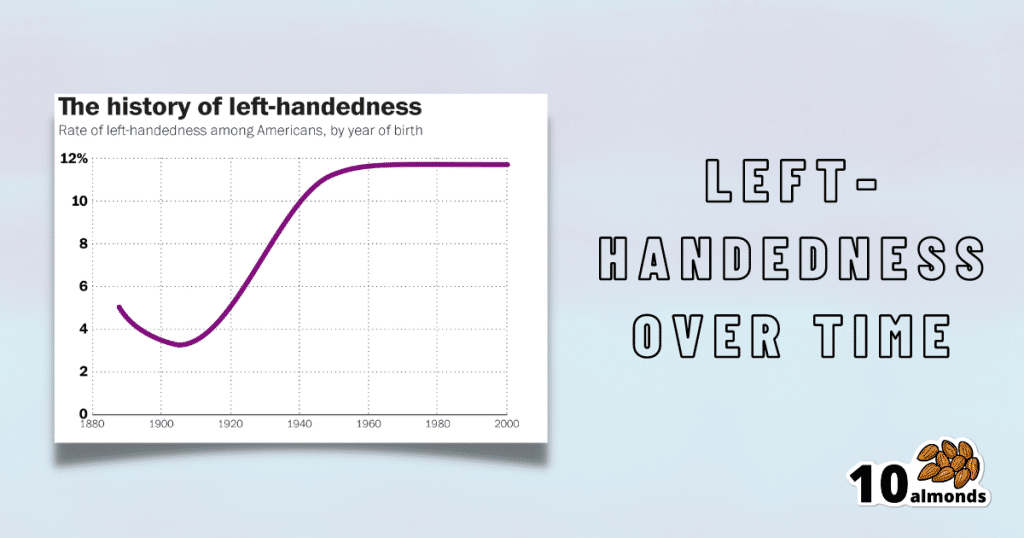
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Share This Post
-

America’s Health System Isn’t Ready for the Surge of Seniors With Disabilities
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The number of older adults with disabilities — difficulty with walking, seeing, hearing, memory, cognition, or performing daily tasks such as bathing or using the bathroom — will soar in the decades ahead, as baby boomers enter their 70s, 80s, and 90s.
But the health care system isn’t ready to address their needs.
That became painfully obvious during the covid-19 pandemic, when older adults with disabilities had trouble getting treatments and hundreds of thousands died. Now, the Department of Health and Human Services and the National Institutes of Health are targeting some failures that led to those problems.
One initiative strengthens access to medical treatments, equipment, and web-based programs for people with disabilities. The other recognizes that people with disabilities, including older adults, are a separate population with special health concerns that need more research and attention.
Lisa Iezzoni, 69, a professor at Harvard Medical School who has lived with multiple sclerosis since her early 20s and is widely considered the godmother of research on disability, called the developments “an important attempt to make health care more equitable for people with disabilities.”
“For too long, medical providers have failed to address change in society, changes in technology, and changes in the kind of assistance that people need,” she said.
Among Iezzoni’s notable findings published in recent years:
Most doctors are biased. In survey results published in 2021, 82% of physicians admitted they believed people with significant disabilities have a worse quality of life than those without impairments. Only 57% said they welcomed disabled patients.
“It’s shocking that so many physicians say they don’t want to care for these patients,” said Eric Campbell, a co-author of the study and professor of medicine at the University of Colorado.
While the findings apply to disabled people of all ages, a larger proportion of older adults live with disabilities than younger age groups. About one-third of people 65 and older — nearly 19 million seniors — have a disability, according to the Institute on Disability at the University of New Hampshire.
Doctors don’t understand their responsibilities. In 2022, Iezzoni, Campbell, and colleagues reported that 36% of physicians had little to no knowledge of their responsibilities under the 1990 Americans With Disabilities Act, indicating a concerning lack of training. The ADA requires medical practices to provide equal access to people with disabilities and accommodate disability-related needs.
Among the practical consequences: Few clinics have height-adjustable tables or mechanical lifts that enable people who are frail or use wheelchairs to receive thorough medical examinations. Only a small number have scales to weigh patients in wheelchairs. And most diagnostic imaging equipment can’t be used by people with serious mobility limitations.
Iezzoni has experienced these issues directly. She relies on a wheelchair and can’t transfer to a fixed-height exam table. She told me she hasn’t been weighed in years.
Among the medical consequences: People with disabilities receive less preventive care and suffer from poorer health than other people, as well as more coexisting medical conditions. Physicians too often rely on incomplete information in making recommendations. There are more barriers to treatment and patients are less satisfied with the care they do get.
Egregiously, during the pandemic, when crisis standards of care were developed, people with disabilities and older adults were deemed low priorities. These standards were meant to ration care, when necessary, given shortages of respirators and other potentially lifesaving interventions.
There’s no starker example of the deleterious confluence of bias against seniors and people with disabilities. Unfortunately, older adults with disabilities routinely encounter these twinned types of discrimination when seeking medical care.
Such discrimination would be explicitly banned under a rule proposed by HHS in September. For the first time in 50 years, it would update Section 504 of the Rehabilitation Act of 1973, a landmark statute that helped establish civil rights for people with disabilities.
The new rule sets specific, enforceable standards for accessible equipment, including exam tables, scales, and diagnostic equipment. And it requires that electronic medical records, medical apps, and websites be made usable for people with various impairments and prohibits treatment policies based on stereotypes about people with disabilities, such as covid-era crisis standards of care.
“This will make a really big difference to disabled people of all ages, especially older adults,” said Alison Barkoff, who heads the HHS Administration for Community Living. She expects the rule to be finalized this year, with provisions related to medical equipment going into effect in 2026. Medical providers will bear extra costs associated with compliance.
Also in September, NIH designated people with disabilities as a population with health disparities that deserves further attention. This makes a new funding stream available and “should spur data collection that allows us to look with greater precision at the barriers and structural issues that have held people with disabilities back,” said Bonnielin Swenor, director of the Johns Hopkins University Disability Health Research Center.
One important barrier for older adults: Unlike younger adults with disabilities, many seniors with impairments don’t identify themselves as disabled.
“Before my mom died in October 2019, she became blind from macular degeneration and deaf from hereditary hearing loss. But she would never say she was disabled,” Iezzoni said.
Similarly, older adults who can’t walk after a stroke or because of severe osteoarthritis generally think of themselves as having a medical condition, not a disability.
Meanwhile, seniors haven’t been well integrated into the disability rights movement, which has been led by young and middle-aged adults. They typically don’t join disability-oriented communities that offer support from people with similar experiences. And they don’t ask for accommodations they might be entitled to under the ADA or the 1973 Rehabilitation Act.
Many seniors don’t even realize they have rights under these laws, Swenor said. “We need to think more inclusively about people with disabilities and ensure that older adults are fully included at this really important moment of change.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Hard to Kill – by Dr. Jaime Seeman
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about Dr. Seeman’s method for robust health at all ages, focussing on:
- Nutrition
- Movement
- Sleep
- Mindset
- Environment
In this book, she expands on these things far more than we have room to in our little newsletter, including (importantly!) how each interplays with the others. She also follows up with an invitation to take the “Hard to Kill 30-Day Challenge”.
That said, in the category of criticism, it’s only 152 pages, and she takes some of that to advertise her online services in an effort to upsell the reader.
Nevertheless, there’s a lot of worth in the book itself, and the writing style is certainly easy-reading and compelling.
Bottom line: this book is half instructional, half motivational, and covers some very important areas of health.
Click here to check out “Hard to Kill”, and enjoy robust health at every age!
Share This Post
-

The Autoimmune Cure – by Dr. Sara Gottfried
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve featured Dr. Gottfried before, as well as another of her books (“Younger”), and this one’s a little different, and on the one hand very specific, while on the other hand affecting a lot of people.
You may be thinking, upon reading the subtitle, “this sounds like Dr. Gabor Maté’s ideas” (per: “When The Body Says No”), and 1) you’d be right, and 2) Dr. Gottfried does credit him in the introduction and refers back to his work periodically later.
What she adds to this, and what makes this book a worthwhile read in addition to Dr. Maté’s, is looking clinically at the interactions of the immune system and nervous system, but also the endocrine system (Dr. Gottfried’s specialty) and the gut.
Another thing she adds is more of a focus on what she writes about as “little-t trauma”, which is the kind of smaller, yet often cumulative, traumas that often eventually add up over time to present as C-PTSD.
While “stress increases inflammation” is not a novel idea, Dr. Gottfried takes it further, and looks at a wealth of clinical evidence to demonstrate the series of events that, if oversimplified, seem unbelievable, such as “you had a bad relationship and now you have lupus”—showing evidence for each step in the snowballing process.
The style is a bit more clinical than most pop-science, but still written to be accessible to laypersons. This means that for most of us, it might not be the quickest read, but it will be an informative and enlightening one.
In terms of practical use (and living up to its subtitle promise of “cure”), this book does also cover all sorts of potential remedial approaches, from the obvious (diet, sleep, supplements, meditation, etc) to the less obvious (ketamine, psilocybin, MDMA, etc), covering the evidence so far as well as the pros and cons.
Bottom line: if you have or suspect you may have an autoimmune problem, and/or would just like to nip the risk of such in the bud (especially bearing in mind that the same things cause neuroinflammation and thus, putatively, depression and dementia too), then this is one for you.
Click here to check out the Autoimmune Cure, and take care of your body and mind!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Psyllium Is Healthy Through-And-Through
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Psyllium is the powder of the husk of the seed of the plant Plantago ovata.
It can be taken as a supplement, and/or used in cooking.
What’s special about it?
It is fibrous, and the fiber is largely soluble fiber. It’s a “bulk-forming laxative”, which means that (dosed correctly) it is good against both constipation (because it’s a laxative) and diarrhea (because it’s bulk-forming).
See also, because this is Research Review Monday and we provide papers for everything:
In other words, it will tend things towards being a 3 or 4 on the Bristol Stool Scale ← this is not pretty, but it is informative.
Before the bowels
Because of how it increases the viscosity of substances it finds itself in, psyllium slows stomach-emptying, and thus improves feelings of satiety.
Here’s a study in which taking psyllium before breakfast and lunch resulted in increased satiety between meals, and reduction in food-related cravings:
Satiety effects of psyllium in healthy volunteers
Prebiotic benefits
We can’t digest psyllium, but our gut bacteria can—somewhat! Because they can only digest some of the psyllium fibers, that means the rest will have the stool-softening effect, while we also get the usual in-gut benefits from prebiotic fiber first too:
The Effect of Psyllium Husk on Intestinal Microbiota in Constipated Patients and Healthy Controls
Cholesterol-binding
Psyllium can bind to cholesterol during the digestive process. Why only “can”? Well, if you don’t consume cholesterol (for example, if you are vegan), then there won’t be cholesterol in the digestive tract to bind to (yes, we do need some cholesterol to live, but like most animals, we can synthesize it ourselves).
What this cholesterol-binding action means is that the dietary cholesterol thus bound cannot enter the bloodstream, and is simply excreted instead:
Heart health beyond cholesterol
Psyllium supplementation can also help lower high blood pressure but does not significantly lower already-healthy blood pressure, so it can be particularly good for keeping things in safe ranges:
❝Given the overarching benefits and lack of reported side effects, particularly for hypertensive patients, health care providers and clinicians should consider the use of psyllium supplementation for the treatment or abatement of hypertension, or hypertensive symptoms.❞
Read in full: The effect of psyllium supplementation on blood pressure: a systematic review and meta-analysis of randomized controlled trials ← you can see the concrete numbers here
Is it safe?
Psyllium is first and foremost a foodstuff, and is considered very safe unless you have an allergy (which is rare, but possible).
However, it is still recommended to start at a low dose and work up, because anything that changes your gut microbiota, even if it changes it for the better, will be easiest if done slowly (or else, you will hear about it from your gut).
Want to try some?
We don’t sell it, but here for your convenience is an example product on Amazon
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

When “Normal” Health Is Not What You Want
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝When going to sleep, I try to breathe through my nose (since everyone says that’s best). But when I wake I often find that I am breathing through my mouth. Is that normal, or should I have my nose checked out?❞
It is quite normal, but when it comes to health, “normal” does not always mean “optimal”.
- Good news: it is correctable!
- Bad news: it is correctable by what may be considered rather an extreme practice that comes with its own inconveniences and health risks.
Some people correct this by using medical tape to keep their mouth closed at night, ensuring nose-breathing. Advocates of this say that after using it for a while, nose-breathing in sleep will become automatic.
We know of no hard science to confirm this, and cannot even offer a personal anecdote on this one. Here are some pop-sci articles that do link to the (very few) studies that have been conducted:
- Mouth taping may be a trending sleep hack, but the science behind it is slim
- Mouth Taping for Sleep: Does it Work? And What are the Side Effects?
This writer’s personal approach is simply to do breathing exercises when going to sleep and first thing upon awakening, and settle for imperfection in this regard while asleep.
Meanwhile, take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: