5 Ways To Beat Afternoon Energy Slumps
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Nisha Vora, of Rainbow Plant Life fame. After graduating from Harvard Law School, she realized she hated being a lawyer, and pivoted completely to become what she now is 12 years later, a chef and health coach.
Here are her tips for boosting energy through the day:
Caffeine timing
If you don’t do caffeine at all, no need to change that, but if you do, Vora advises that midday is the best time for it, with a very good rationale:
- of course it should not be too late in the day, because the elimination half-life of caffeine (4–8 hours to eliminate just half of the caffeine, depending on genes, call it 6 hours as an average though honestly for most people it will either be 4 or 8, not 6) is such that it can easily interfere with sleep for most people
- because caffeine is an adenosine blocker, not an adenosine inhibitor, taking caffeine in the morning means either there’s no adenosine to block, or it’ll just “save” that adenosine for later, i.e. when the caffeine is eliminated, then the adenosine will kick in, meaning that your morning sleepiness has now been deferred to the afternoon, rather than eliminated.
Another reminder that caffeine is the “payday loan” of energy. So, midday it is. No morning sleepiness to defer, and yet also not so late as to interfere with sleep.
See also: Calculate (And Enjoy) The Perfect Night’s Sleep
Simplify what can be simplified
This one’s not from a physiological basis, but rather, that a lot of the time most of us have much of our energy being taken by constant task-switching (what gets called multitasking, but as our brain is a single processor, it really means switching rapidly between different kinds of cognition, which is not efficient). In order to avoid that energy drain, try to streamline things and make a particular effort to not only single-task, but to do so without distractions.
Counterpoint: if you have unmedicated ADHD, then chances are you’ll do better with a single small distraction chosen by you, than trying to go without distractions, because your brain will find distractions anyway, so you might as well choose one (for many people it is background music, or a podcast or TV show that one doesn’t may attention to but it’s there) as a matter of harm reduction, and that way you’ll do better at focusing on your primary task than if your brain were reaching out for every and any possible distraction.
Manage your blood sugars
In particular, she advocates for avoiding sugary breakfasts, opting instead for protein, fat, and fiber-rich options. For more in this regard, see:
10 Ways To Balance Your Blood Sugars
Walk after meals
You don’t have to don hiking boots and “I am just going outside and may be some time“; rather, even a 2–5 minute walk after a meal helps regulate digestion and glucose levels, avoiding postprandial energy slumps.
So,
- if you have a treadmill, after eating is a great time to use it for a few minutes
- if you have stairs, now’s a great time to go up and down them a few times
One last technique for when everything else fails
We’ll quote her directly on this one:
❝Despite my best efforts, soemtimes I just have one of those days. Maybe I didn’t sleep well or I’m distracted by my never ending thoughts. If I need to be productive or energized on those days, I will do something that I absolutely hate:
I will take a cold shower.
And I hate it because I’m already always cold all the time, so why would I want to get a cold shower?
Well, it’s because cold water immersion has been shown to dramatically boost your dopamine levels, which gives you more energy and motivation.
In the moment though, it’s mostly painful and I hate everything and everyone around me.
But I know that if I can suffer through two minutes of a cold shower, I will feel so refreshed.❞
There are more benefits than just that, though, see:
A Cold Shower A Day Keeps The Doctor Away?
Want more from Nisha Vora?
We reviewed one of her books a while back:
The Vegan Instant Pot Cookbook – by Nisha Vora
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Our family is always glued to separate devices. How can we connect again?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Saturday afternoon and the kids are all connected to separate devices. So are the parents. Sounds familiar?
Many families want to set ground rules to help them reduce their screen time – and have time to connect with each other, without devices.
But it can be difficult to know where to start and how to make a plan that suits your family.
First, look at your own screen time
Before telling children to “hop off the tech”, it’s important parents understand how much they are using screens themselves.
Globally, the average person spends an average of six hours and 58 minutes on screens each day. This has increased by 13%, or 49 minutes, since 2013.
Parents who report high screen time use tend to see this filtering down to the children in their family too. Two-thirds of primary school-aged children in Australia have their own mobile screen-based device.
Australia’s screen time guidelines recommended children aged five to 17 years have no more than two hours of sedentary screen time (excluding homework) each day. For those aged two to five years, it’s no more than one hour a day. And the guidelines recommend no screen time at all for children under two.
Yet the majority of children, across age groups, exceed these maximums. A new Australian study released this week found the average three-year-old is exposed to two hours and 52 minutes of screen time a day.
Some screen time is OK, too much increases risks
Technology has profoundly impacted children’s lives, offering both opportunities and challenges.
On one hand, it provides access to educational resources, can develop creativity, facilitates communication with peers and family members, and allows students to seek out new information.
On the other hand, excessive screen use can result in too much time being sedentary, delays in developmental milestones, disrupted sleep and daytime drowsiness.

Disrupted sleep can leave children tired the next day.
Yulia Raneva/ShutterstockToo much screen time can affect social skills, as it replaces time spent in face-to-face social interactions. This is where children learn verbal and non-verbal communication, develop empathy, learn patience and how to take turns.
Many families also worry about how to maintain a positive relationship with their children when so much of their time is spent glued to screens.
What about when we’re all on devices?
When families are all using devices simultaneously, it results in less face-to-face interactions, reducing communication and resulting in a shift in family dynamics.
The increased use of wireless technology enables families to easily tune out from each other by putting in earphones, reducing the opportunity for conversation. Family members wearing earphones during shared activities or meals creates a physical barrier and encourages people to retreat into their own digital worlds.
Wearing earphones for long periods may also reduce connection to, and closeness with, family members. Research from video gaming, for instance, found excessing gaming increases feelings of isolation, loneliness and the displacement of real-world social interactions, alongside weakened relationships with peers and family members.
How can I set screen time limits?
Start by sitting down as a family and discussing what limits you all feel would be appropriate when using TVs, phones and gaming – and when is an appropriate time to use them.
Have set rules around family time – for example, no devices at the dinner table – so you can connect through face-to-face interactions.
One rule might be no devices at the dinner table.
Monkey Business Images/ShutterstockConsider locking your phone or devices away at certain periods throughout the week, such as after 9pm (or within an hour of bedtime for younger children) and seek out opportunities to balance your days with physical activities, such kicking a footy at the park or going on a family bush walk.
Parents can model healthy behaviour by regulating and setting limits on their own screen time. This might mean limiting your social media scrolling to 15 or 30 minutes a day and keeping your phone in the next room when you’re not using it.
When establishing appropriate boundaries and ensuring children’s safety, it is crucial for parents and guardians to engage in open communication about technology use. This includes teaching critical thinking skills to navigate online content safely and employing parental control tools and privacy settings.
Parents can foster a supportive and trusting relationship with children from an early age so children feel comfortable discussing their online experiences and sharing their fears or concerns.
For resources to help you develop your own family’s screen time plan, visit the Raising Children Network.

Elise Waghorn, Lecturer, School of Education, RMIT University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Can a drug like Ozempic help treat addictions to alcohol, opioids or other substances?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Semaglutide (sold as Ozempic, Wegovy and Rybelsus) was initially developed to treat diabetes. It works by stimulating the production of insulin to keep blood sugar levels in check.
This type of drug is increasingly being prescribed for weight loss, despite the fact it was initially approved for another purpose. Recently, there has been growing interest in another possible use: to treat addiction.
Anecdotal reports from patients taking semaglutide for weight loss suggest it reduces their appetite and craving for food, but surprisingly, it also may reduce their desire to drink alcohol, smoke cigarettes or take other drugs.
But does the research evidence back this up?
Animal studies show positive results
Semaglutide works on glucagon-like peptide-1 receptors and is known as a “GLP-1 agonist”.
Animal studies in rodents and monkeys have been overwhelmingly positive. Studies suggest GLP-1 agonists can reduce drug consumption and the rewarding value of drugs, including alcohol, nicotine, cocaine and opioids.
Out team has reviewed the evidence and found more than 30 different pre-clinical studies have been conducted. The majority show positive results in reducing drug and alcohol consumption or cravings. More than half of these studies focus specifically on alcohol use.
However, translating research evidence from animal models to people living with addiction is challenging. Although these results are promising, it’s still too early to tell if it will be safe and effective in humans with alcohol use disorder, nicotine addiction or another drug dependence.
What about research in humans?
Research findings are mixed in human studies.
Only one large randomised controlled trial has been conducted so far on alcohol. This study of 127 people found no difference between exenatide (a GLP-1 agonist) and placebo (a sham treatment) in reducing alcohol use or heavy drinking over 26 weeks.
In fact, everyone in the study reduced their drinking, both people on active medication and in the placebo group.
However, the authors conducted further analyses to examine changes in drinking in relation to weight. They found there was a reduction in drinking for people who had both alcohol use problems and obesity.
For people who started at a normal weight (BMI less than 30), despite initial reductions in drinking, they observed a rebound increase in levels of heavy drinking after four weeks of medication, with an overall increase in heavy drinking days relative to those who took the placebo.
There were no differences between groups for other measures of drinking, such as cravings.
Some studies show a rebound increase in levels of heavy drinking. Deman/Shutterstock In another 12-week trial, researchers found the GLP-1 agonist dulaglutide did not help to reduce smoking.
However, people receiving GLP-1 agonist dulaglutide drank 29% less alcohol than those on the placebo. Over 90% of people in this study also had obesity.
Smaller studies have looked at GLP-1 agonists short-term for cocaine and opioids, with mixed results.
There are currently many other clinical studies of GLP-1 agonists and alcohol and other addictive disorders underway.
While we await findings from bigger studies, it’s difficult to interpret the conflicting results. These differences in treatment response may come from individual differences that affect addiction, including physical and mental health problems.
Larger studies in broader populations of people will tell us more about whether GLP-1 agonists will work for addiction, and if so, for whom.
How might these drugs work for addiction?
The exact way GLP-1 agonists act are not yet well understood, however in addition to reducing consumption (of food or drugs), they also may reduce cravings.
Animal studies show GLP-1 agonists reduce craving for cocaine and opioids.
This may involve a key are of the brain reward circuit, the ventral striatum, with experimenters showing if they directly administer GLP-1 agonists into this region, rats show reduced “craving” for oxycodone or cocaine, possibly through reducing drug-induced dopamine release.
Using human brain imaging, experimenters can elicit craving by showing images (cues) associated with alcohol. The GLP-1 agonist exenatide reduced brain activity in response to an alcohol cue. Researchers saw reduced brain activity in the ventral striatum and septal areas of the brain, which connect to regions that regulate emotion, like the amygdala.
In studies in humans, it remains unclear whether GLP-1 agonists act directly to reduce cravings for alcohol or other drugs. This needs to be directly assessed in future research, alongside any reductions in use.
Are these drugs safe to use for addiction?
Overall, GLP-1 agonists have been shown to be relatively safe in healthy adults, and in people with diabetes or obesity. However side effects do include nausea, digestive troubles and headaches.
And while some people are OK with losing weight as a side effect, others aren’t. If someone is already underweight, for example, this drug might not be suitable for them.
In addition, very few studies have been conducted in people with addictive disorders. Yet some side effects may be more of an issue in people with addiction. Recent research, for instance, points to a rare risk of pancreatitis associated with GLP-1 agonists, and people with alcohol use problems already have a higher risk of this disorder.
Other drugs treatments are currently available
Although emerging research on GLP-1 agonists for addiction is an exciting development, much more research needs to be done to know the risks and benefits of these GLP-1 agonists for people living with addiction.
In the meantime, existing effective medications for addiction remain under-prescribed. Only about 3% of Australians with alcohol dependence, for example, are prescribed medication treatments such as like naltrexone, acamprosate or disulfiram. We need to ensure current medication treatments are accessible and health providers know how to prescribe them.
Continued innovation in addiction treatment is also essential. Our team is leading research towards other individualised and effective medications for alcohol dependence, while others are investigating treatments for nicotine addiction and other drug dependence.
Read the other articles in The Conversation’s Ozempic series here.
Shalini Arunogiri, Addiction Psychiatrist, Associate Professor, Monash University; Leigh Walker, , Florey Institute of Neuroscience and Mental Health, and Roberta Anversa, , The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Healthy Kids, Happy Kids – by Dr. Elisa Song
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you have young children or perhaps grandchildren, you probably care deeply about those children and their wellbeing, but there can often be a lot more guesswork than would be ideal, when it comes to ensuring they be and remain healthy.
Nevertheless, a lot of common treatments for children are based (whether parents know it or not—and often they dont) on what is most convenient for the parent, not necessarily what is best for the child. Dr. Song looks to correct that.
Rather than dosing kids with acetaminophen or even antibiotics, assuming eczema can be best fixed with a topical cream (treating the symptom rather than the cause, much?), and that some things like asthma “just are”, and “that’s unfortunate”, Dr. Song takes us on a tour of pediatric health, centered around the gut.
Why the gut? Well, it’s pretty central to us as adults, and it’s the same for kids, except one difference: their gut microbiome is changing even more quickly than ours (along with the rest of their body), and as such, is even more susceptible to little nudges for better or for worse, having a big impact in either direction. So, might as well make it a good one!
After an explanatory overview, most of the book is given over to recognizing and correcting what things can go wrong, including the top 25 acute childhood conditions, and the most critical chronic ones, and how to keep things on-track as a team (the child is part of the team! An important part!).
The style of the book is very direct and instructional; easy to understand throughout. It’s a lot like being in a room with a very competent pediatrician who knows her stuff and explains it well, thus neither patronizing nor mystifying.
Bottom line: if there are kids in your life, be they yours or your grandkids or someone else, this is a fine book for giving them the best foundational health.
Click here to check out Healthy Kids, Happy Kids, and take care of yours!
Share This Post



Related Posts
-
Healthy Relationship, Healthy Life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Only One Kind Of Relationship Promotes Longevity This Much!
One of the well-established keys of a long healthy life is being in a fulfilling relationship. That’s not to say that one can’t be single and happy and fulfilled—one totally can. But statistically, those who live longest, do so in happy, fulfilling, committed relationships.
Note: happy, fulfilling, committed relationships. Less than that won’t do. Your insurance company might care about your marital status for its own sake, but your actual health doesn’t—it’s about the emotional safety and security that a good, healthy, happy, fulfilling relationship offers.
How to keep the “love coals” warm
When “new relationship energy” subsides and we’ve made our way hand-in-hand through the “honeymoon period”, what next? For many, a life of routine. And that’s not intrinsically bad—routine itself can be comforting! But for love to work, according to relational psychologists, it also needs something a little more.
What things? Let’s break it down…
Bids for connection—and responsiveness to same
There’s an oft-quoted story about a person who knew their marriage was over when their spouse wouldn’t come look at their tomatoes. That may seem overblown, but…
When we care about someone, we want to share our life with them. Not just in the sense of cohabitation and taxes, but in the sense of:
- Little moments of joy
- Things we learned
- Things we saw
- Things we did
…and there’s someone we’re first to go to share these things with. And when we do, that’s a “bid for connection”. It’s important that we:
- Make bids for connection frequently
- Respond appropriately to our partner’s bids for connection
Of course, we cannot always give everything our full attention. But whenever we can, we should show as much genuine interest as we can.
Keep asking the important questions
Not just “what shall we have for dinner?”, but:
- “What’s a life dream that you have at the moment?”
- “What are the most important things in life?”
- “What would you regret not doing, if you never got the chance?”
…and so forth. Even after many years with a partner, the answers can sometimes surprise us. Not because we don’t know our partners, but because the answers can change with time, and sometimes we can even surprise ourselves, if it’s a question we haven’t considered for a while.
It’s good to learn and grow like this together—and to keep doing so!
Express gratitude/appreciation
For the little things as well as the big:
- Thank you for staying by my side during life’s storms
- Thank you for bringing me a coffee
- Thank you for taking on these responsibilities with me
- I really appreciate your DIY skills
- I really appreciate your understanding nature
On which note…
Compliment, often and sincerely
Most importantly, compliment things intrinsic to their character, not just peripheral attributes like appearance, and also not just what they do for you.
- You’re such a patient person; I really admire that
- I really hit the jackpot to get someone I can trust so completely as you
- You are the kindest and sweetest soul I have ever encountered in life
- I love that you have such a blend of strength and compassion
- Your unwavering dedication to your personal values makes me so proud
…whatever goes for your partner and how you see them and what you love about them!
Express your needs, and ask about theirs
We’re none of us mind-readers, and it’s easy to languish in “if they really cared, I wouldn’t have to ask”, or conversely, “if they wanted something, they would surely say so”.
Communicate. Effectively. Life is too short to waste in miscommunication and unsaid things!
We covered much more detailed how-tos of this in a previous issue, but good double-whammy of top tier communication is:
- “I need…” / “Please will you…”
- “What do you need?” / “How can I help?”
Touch. Often.
It takes about 20 seconds of sustained contact for oxytocin to take effect, so remember that when you hug your partner, hold hands when walking, or cuddle up the sofa.
Have regular date nights
It doesn’t have to be fancy. A date night can be cooking together, it can be watching a movie together at home. It can be having a scheduled time to each bring a “big question” or five, from what we talked about above!
Most importantly: it’s a planned shared experience where the intent is to enjoy each other’s romantic company, and have a focus on each other. Having a regularly recurring date night, be it the last day of each month, or every second Saturday, or every Friday night, whatever your schedules allow, makes such a big difference to feel you are indeed “dating” and in the full flushes of love—not merely cohabiting pleasantly.
Want ideas?
Check out these:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A short history of sunscreen, from basting like a chook to preventing skin cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australians have used commercial creams, lotions or gels to manage our skin’s sun exposure for nearly a century.
But why we do it, the preparations themselves, and whether they work, has changed over time.
In this short history of sunscreen in Australia, we look at how we’ve slathered, slopped and spritzed our skin for sometimes surprising reasons.
At first, suncreams helped you ‘tan with ease’

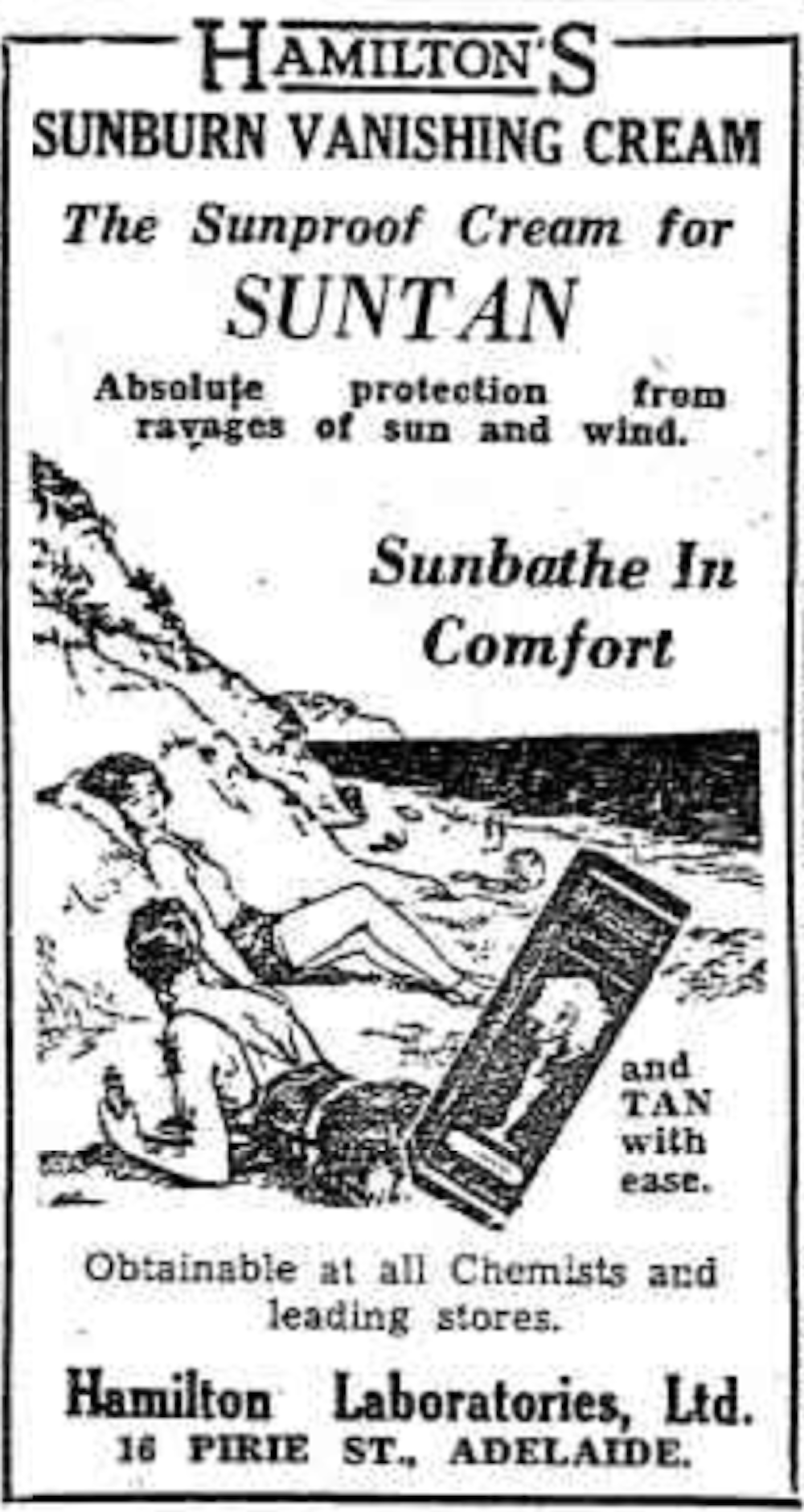
This early sunscreen claimed you could ‘tan with ease’.
Trove/NLASunscreens have been available in Australia since the 30s. Chemist Milton Blake made one of the first.
He used a kerosene heater to cook batches of “sunburn vanishing cream”, scented with French perfume.
His backyard business became H.A. Milton (Hamilton) Laboratories, which still makes sunscreens today.
Hamilton’s first cream claimed you could “
Sunbathe in Comfort and TAN with ease”. According to modern standards, it would have had an SPF (or sun protection factor) of 2.The mirage of ‘safe tanning’
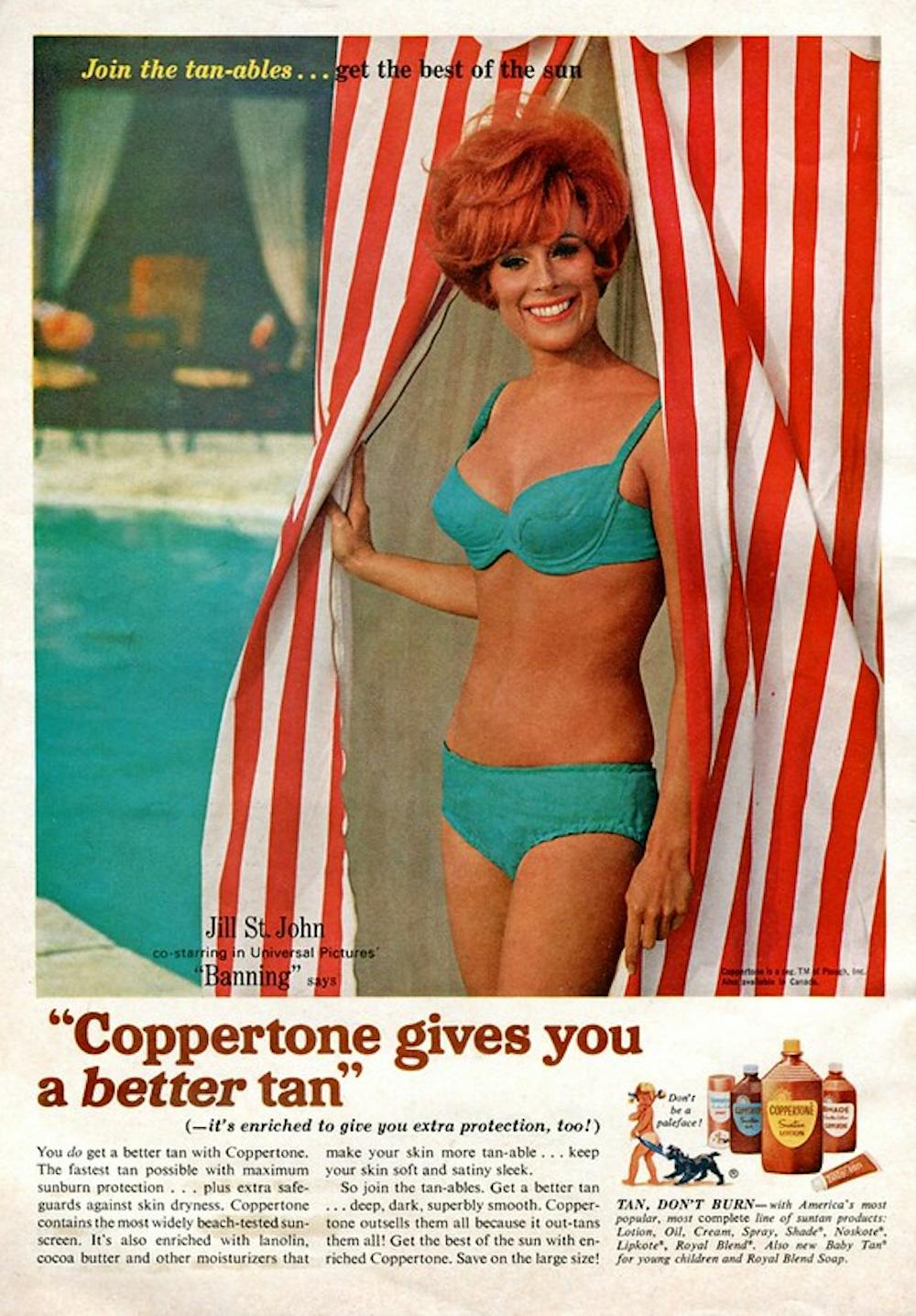
A tan was considered a “modern complexion” and for most of the 20th century, you might put something on your skin to help gain one. That’s when “safe tanning” (without burning) was thought possible.

This 1967 Coppertone advertisement urged you to ‘tan, not burn’.
SenseiAlan/Flickr, CC BY-SASunburn was known to be caused by the UVB component of ultraviolet (UV) light. UVA, however, was thought not to be involved in burning; it was just thought to darken the skin pigment melanin. So, medical authorities advised that by using a sunscreen that filtered out UVB, you could “safely tan” without burning.
But that was wrong.
From the 70s, medical research suggested UVA penetrated damagingly deep into the skin, causing ageing effects such as sunspots and wrinkles. And both UVA and UVB could cause skin cancer.
Sunscreens from the 80s sought to be “broad spectrum” – they filtered both UVB and UVA.
Researchers consequently recommended sunscreens for all skin tones, including for preventing sun damage in people with dark skin.
Delaying burning … or encouraging it?
Up to the 80s, sun preparations ranged from something that claimed to delay burning, to preparations that actively encouraged it to get that desirable tan – think, baby oil or coconut oil. Sun-worshippers even raided the kitchen cabinet, slicking olive oil on their skin.
One manufacturer’s “sun lotion” might effectively filter UVB; another’s merely basted you like a roast chicken.
Since labelling laws before the 80s didn’t require manufacturers to list the ingredients, it was often hard for consumers to tell which was which.
At last, SPF arrives to guide consumers
In the 70s, two Queensland researchers, Gordon Groves and Don Robertson, developed tests for sunscreens – sometimes experimenting on students or colleagues. They printed their ranking in the newspaper, which the public could use to choose a product.
An Australian sunscreen manufacturer then asked the federal health department to regulate the industry. The company wanted standard definitions to market their products, backed up by consistent lab testing methods.
In 1986, after years of consultation with manufacturers, researchers and consumers, Australian Standard AS2604 gave a specified a testing method, based on the Queensland researchers’ work. We also had a way of expressing how well sunscreens worked – the sun protection factor or SPF.
This is the ratio of how long it takes a fair-skinned person to burn using the product compared with how long it takes to burn without it. So a cream that protects the skin sufficiently so it takes 40 minutes to burn instead of 20 minutes has an SPF of 2.
Manufacturers liked SPF because businesses that invested in clever chemistry could distinguish themselves in marketing. Consumers liked SPF because it was easy to understand – the higher the number, the better the protection.
Australians, encouraged from 1981 by the Slip! Slop! Slap! nationwide skin cancer campaign, could now “slop” on a sunscreen knowing the degree of protection it offered.
How about skin cancer?
It wasn’t until 1999 that research proved that using sunscreen prevents skin cancer. Again, we have Queensland to thank, specifically the residents of Nambour. They took part in a trial for nearly five years, carried out by a research team led by Adele Green of the Queensland Institute of Medical Research. Using sunscreen daily over that time reduced rates of squamous cell carcinoma (a common form of skin cancer) by about 60%.
Follow-up studies in 2011 and 2013 showed regular sunscreen use almost halved the rate of melanoma and slowed skin ageing. But there was no impact on rates of basal cell carcinoma, another common skin cancer.
By then, researchers had shown sunscreen stopped sunburn, and stopping sunburn would prevent at least some types of skin cancer.
What’s in sunscreen today?
An effective sunscreen uses one or more active ingredients in a cream, lotion or gel. The active ingredient either works:
-
“chemically” by absorbing UV and converting it to heat. Examples include PABA (para-aminobenzoic acid) and benzyl salicylate, or
-
“physically” by blocking the UV, such as zinc oxide or titanium dioxide.
Physical blockers at first had limited cosmetic appeal because they were opaque pastes. (Think cricketers with zinc smeared on their noses.)
With microfine particle technology from the 90s, sunscreen manufacturers could then use a combination of chemical absorbers and physical blockers to achieve high degrees of sun protection in a cosmetically acceptable formulation.
Where now?
Australians have embraced sunscreen, but they still don’t apply enough or reapply often enough.
Although some people are concerned sunscreen will block the skin’s ability to make vitamin D this is unlikely. That’s because even SPF50 sunscreen doesn’t filter out all UVB.
There’s also concern about the active ingredients in sunscreen getting into the environment and whether their absorption by our bodies is a problem.
Sunscreens have evolved from something that at best offered mild protection to effective, easy-to-use products that stave off the harmful effects of UV. They’ve evolved from something only people with fair skin used to a product for anyone.
Remember, slopping on sunscreen is just one part of sun protection. Don’t forget to also slip (protective clothing), slap (hat), seek (shade) and slide (sunglasses).
Laura Dawes, Research Fellow in Medico-Legal History, Australian National University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
-

The Science Of New Year’s Pre-Resolutions
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Science Of New Year’s Pre-Resolutions
There’s a military dictum that “prior preparation and planning prevents piss-poor performance”.
Would it surprise you to know that soldiers going on the attack are not focused on the goal? Rather, they are focused on the process.
With drills and mnemonics, everything that can be controlled for in advance is; every action, every reaction, everything that can go wrong, and all the “if x then y” decisions in between pre-battle PREWAR and PAWPERSO and post-battle PACESDO (all mnemonic acronyms; the content is not important here but the principle is).
In short: take Murphy’s Law into account now, and plan accordingly!
The same goes for making your plans the winning kind
If you want your resolutions to work, you may need to make pre-resolutions now, so that you’re properly prepared:
- Do you want to make an exercise habit? Make sure now that you have the right clothes/shoes/etc, make sure that they fit you correctly, make sure you have enough of them that you can exercise when one set’s in the wash, etc.
- What grace will you allow yourself if tired, unwell, busy? What’s your back-up plan so that you still do what you can at those times when “what you can” is legitimately a bit less?
- If it’s an outdoors plan, what’s your plan for when it’s rainy? Snowy? Dangerously hot?
- What are the parameters for what counts? Make it measurable. How many exercise sessions per week, what duration?
- Do you want to make a diet habit? Make sure that you have in the healthy foods that you want to eat; know where you can and will get things. We’re often creatures of habit when it comes to shopping, so planning will be critical here!
- Do you want to cut some food/drink/substance out? Make sure you have a plan to run down or otherwise dispose of your current stock first. And make sure you have alternatives set up, and if it was something you were leaning on as a coping strategy of some kind (e.g. alcohol, cannabis, comfort-eating, etc), make sure you have an alternative coping strategy, too!
See also: How To Reduce Or Quit Alcohol
We promised science, so here it comes
Approach-oriented resolutions work better than avoidance-oriented ones.
This means: positively-framed resolutions work better than negatively-framed ones.
On a simple level, this means that, for example, resolving to exercise three times per week is going to work better than resolving to not consume alcohol.
But what if you really want to quit something? Just frame it positively. There’s a reason that Alcoholics Anonymous (and similar Thing Anonymous groups) measure days sober, not relapses.
So it’s not “I will not consume alcohol” but “I will get through each day alcohol-free”.
Semantics? Maybe, but it’s also science:
Why January the 1st? It’s a fresh start
Resolutions started on the 1st of January enjoy a psychological boost of a feeling of a fresh start, a new page, a new chapter.
Similar benefits can be found from starting on the 1st of a month in general, or on a Monday, or on some date that is auspicious to the person in question (religious fasts tied to calendar dates are a fine example of this).
Again, this is borne-out by science:
The Fresh Start Effect: Temporal Landmarks Motivate Aspirational Behavior
Make it a habit
Here be science:
How do people adhere to goals when willpower is low? The profits (and pitfalls) of strong habits
As for how to do that?
How To Really Pick Up (And Keep!) Those Habits
Trim the middle
No, we’re not talking about your waistline. Rather, what Dr. Ayelet Fischbach refers to as “the middle problem”:
❝We’re highly motivated at the beginning. Over time, our motivation declines as we lose steam. To the extent that our goal has a clear end point, our motivation picks up again toward the end.
Therefore, people are more likely to adhere to their standards at the beginning and end of goal pursuit—and slack in the middle. We demonstrate this pattern of judgment and behavior in adherence to ethical standards (e.g., cheating), religious traditions (e.g., skipping religious rituals), and performance standards (e.g., “cutting corners” on a task).
We also show that the motivation to adhere to standards by using proper means is independent and follows a different pattern from the motivation to reach the end state of goal pursuit❞
Read: The end justifies the means, but only in the middle
How to fix this, then?
Give yourself consistent, recurring, short-term goals, with frequent review points. That way, it’s never “the middle” for long:
The fresh start effect: temporal landmarks motivate aspirational behavior
See also:
How do people protect their long-term goals from the influence of short-term motives or temptations?
Finally…
You might like this previous main feature of ours that was specifically about getting oneself through those “middle” parts:
How To Keep On Keeping On… Long Term!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Do you want to make an exercise habit? Make sure now that you have the right clothes/shoes/etc, make sure that they fit you correctly, make sure you have enough of them that you can exercise when one set’s in the wash, etc.