5 Surprising Benefits Of Exercise After 50 (More Than Just Fitness)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s easy to want to do less as we get older, but the benefits of continuing to actively exercise, pushing oneself even just a little, can be far-reaching.
Direct and indirect benefits
As well as the obvious fitness benefits, keeping up good levels of exercise can also offer:
Healthy Skin
Exercise improves circulation, bringing growth factors (thus: regeneration, because it’s replacing cells), oxygen, and nutrients to the skin. Accordingly, it can lead to healthier, more youthful-looking skin as a low-cost alternative to a lot of skincare products. That said, it also encourages good skin habits, like daily sunscreen use.
Bone Health
Weight-bearing and resistance exercises (which between them, encompasses most forms of exercise) improve bone density. This is because physical stress signals bones to strengthen, reducing the risk of fractures. This includes activities like walking, hiking, and using resistance bands or weights. Note however that it is on a “per bone” basis. So for example, hiking will improve your lower body and spine, but do nothing for your arms. On the other hand, doing a daily groceries trip on foot, if local geography makes that practicable, can do the whole body, if one is then carrying groceries home (this writer lives about 2 miles from where she buys groceries, and does this pretty much daily).
Mental Health
Exercise, especially outdoors, has well-established positive effects on mental well-being, and can relieve stress and improve mood. As a bonus, community engagement and shared experiences can enhance mental health benefits for many people—but if you prefer it as peaceful time for yourself, that’s beneficial in its own way too!
Better Sleep
Physical activity helps promote better sleep quality, which is important for so many aspects of health—because fatiguing the body through exercise can lead to a more restful night, which is often harder to achieve with age.
Visibility and Confidence
Staying active and taking on challenges (e.g. training for some event) can boost visibility in social and family settings, countering “invisibility” often felt from midlife onwards. And even if one doesn’t do those things, exercise fosters confidence and helps people carry themselves with more self-assurance, which has a lot of knock-on benefits too.
For more on all of these things, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Are There Any Sensible Age Limits To Exercise?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

To-Do List Formula – by Damon Zahariades

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The first part of this book is given to reviewing popular to-do list methods that are already widely “out there”. This treatment is practical and exploratory, looking at the pros and cons of each.
The second part of the book is more Zahariades’ own method, taking what he sees as the best of each, plus some tricks and practices of his own. With these, he builds (and shares!) his optimized system.
You may be wondering what you, dear reader, can expect to get out of this book. Well, that depends on where you’re coming from:
Are you new to approaching your general to-dos with a system more organized than post-it notes on your fridge? If so, this will be a great initial introduction to many systems.
Or are you, perhaps, a veteran of GTD, ToDoist, assorted Pomodoro-based systems, and more? Do you do/delegate/defer/ditch tasks more deftly and dextrously than Serena Williams despatches tennis balls?
If so, what you’re more likely to gain here is a fresh perspective on old ideas, and maybe a trick or two you didn’t know before. At the very least, a boost to your motivation, getting you fired up for doing what you know best again.
All in all, a very respectable book for anyone’s to-read list!
Pick Up Your Copy of Zahariades’ To-Do List Formula on Amazon Today!
Share This Post
-

Hearing voices is common and can be distressing. Virtual reality might help us meet and ‘treat’ them
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever heard something that others cannot – such as your name being called? Hearing voices or other noises that aren’t there is very common. About 10% of people report experiencing auditory hallucinations at some point in their life.
The experience of hearing voices can be very different from person to person, and can change over time. They might be the voice of someone familiar or unknown. There might be many voices, or just one or two. They can be loud or quiet like a whisper.
For some people these experiences are positive. They might represent a spiritual or supernatural experience they welcome or a comforting presence. But for others these experiences are distressing. Voices can be intrusive, negative, critical or threatening. Difficult voices can make a person feel worried, frightened, embarrassed or frustrated. They can also make it hard to concentrate, be around other people and get in the way of day-to-day activities.
Although not everyone who hears voices has a mental health problem, these experiences are much more common in people who do. They have been considered a hallmark symptom of schizophrenia, which affects about 24 million people worldwide.
However, such experiences are also common in other mental health problems, particularly in mood- and trauma-related disorders (such as bipolar disorder or depression and post-traumatic stress disorder) where as many as half of people may experience them.

Rawpixel/Shutterstock Why do people hear voices?
It is unclear exactly why people hear voices but exposure to prolonged stress, trauma or depression can increase the chances.
Some research suggests people who hear voices might have brains that are “wired” differently, particularly between the hearing and speaking parts of the brain. This may mean parts of our inner speech can be experienced as external voices. So, having the thought “you are useless” when something goes wrong might be experienced as an external person speaking the words.
Other research suggests it may relate to how our brains use past experiences as a template to make sense of and make predictions about the world. Sometimes those templates can be so strong they lead to errors in how we experience what is going on around us, including hearing things our brain is “expecting” rather than what is really happening.
What is clear is that when people tell us they are hearing voices, they really are! Their brain perceives voice experiences as if someone were talking in the room. We could think of this “mistake” as working a bit like being susceptible to common optical tricks or visual illusions.
There may be differences in the brains of people who hear voices. Triff/Shutterstock Coping with hearing voices
When hearing voices is getting in the way of life, treatment guidelines recommend the use of medications. But roughly a third of people will experience ongoing distress. As such, treatment guidelines also recommend the use of psychological therapies such as cognitive behavioural therapy.
The next generation of psychological therapies are beginning to use digital technologies and virtual reality offers a promising new medium.
Avatar therapy allows a person to create a virtual representation of the voice or voices, which looks and sounds like what they are experiencing. This can help people regain power in the “relationship” as they interact with the voice character, supported by a therapist.
Jason’s experience
Aged 53, Jason (not his real name) had struggled with persistent voices since his early 20s. Antipsychotic medication had helped him to some extent over the years, but he was still living with distressing voices. Jason tried out avatar therapy as part of a research trial.
He was initially unable to stand up to the voices, but he slowly gained confidence and tested out different ways of responding to the avatar and voices with his therapist’s support.
Jason became more able to set boundaries, such as not listening to them for periods throughout the day. He also felt more able to challenge what they said and make his own choices.
Over a couple of months, Jason started to experience some breaks from the voices each day and his relationship with them started to change. They were no longer like bullies, but more like critical friends pointing out things he could consider or be aware of.
A screenshot from HekaVR, the software used in the Australian AMETHYST trial. HekaVR, CC BY-ND Gaining recognition
Following promising results overseas and its recommendation by the United Kingdom’s National Institute for Health and Care Excellence, our team has begun adapting the therapy for an Australian context.
We are trialling delivering avatar therapy from our specialist voices clinic via telehealth. We are also testing whether avatar therapy is more effective than the current standard therapy for hearing voices, based on cognitive behavioural therapy.
As only a minority of people with psychosis receive specialist psychological therapy for hearing voices, we hope our trial will support scaling up these new treatments to be available more routinely across the country.
We would like to acknowledge the advice and input of Dr Nadine Keen (consultant clinical psychologist at South London and Maudsley NHS Foundation Trust, UK) on this article.
Leila Jameel, Trial Co-ordinator and Research Therapist, Swinburne University of Technology; Imogen Bell, Senior Research Fellow and Psychologist, The University of Melbourne; Neil Thomas, Professor of Clinical Psychology, Swinburne University of Technology, and Rachel Brand, Senior Lecturer in Clinical Psychology, University of the Sunshine Coast
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Too Much Or Too Little Testosterone?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One Man’s Saw Palmetto Is Another Woman’s Serenoa Repens…
Today we’re going to look at saw palmetto. So, first:
What is it?
Saw palmetto is a type of palm native to the southeastern United States. Its scientific name is “Serenoa repens”, so if that name appears in studies we cite, it’s the same thing. By whichever name, it’s widely enjoyed as a herbal supplement.
Why do people take it?
Here’s where it gets interesting, because people take it for some completely opposite reasons…
Indeed, searching for it on the Internet will cause Google to suggest “…for men” and “…for women” as the top suggestions.
That’s because it works on testosterone, and testosterone can be a bit of a double-edged sword, so some people want to increase or decrease certain testosterone-related effects on their body.
And it works for both! Here be science:
- Testosterone (henceforth, “T”) is produced in the human body.
- Yes, all human bodies, to some extent.
- An enzyme called 5-alpha-reductase converts T in to DHT (dihydrogen testosterone)
- DHT is a much more potent androgen (masculinizing agent) than T alone, such that its effects are often unwanted, including:
- Enlarged prostate (if you have one)
- Hair loss (especially in men)
- New facial hair growth (usually unwanted by women)
- Women are more likely to get this due to PCOS and/or the menopause
To avoid those effects, you really want less of your T to be converted into DHT.
Saw palmetto is a 5α-reductase inhibitor, so if you take it, you’ll have less DHT, and you’ll consequently lose less hair, have fewer prostate problems, etc.
^The above study showed that saw palmetto extract performed comparably to finasteride. Finasteride is the world’s main go-to prescription drug for treating enlarged prostate and/or hair loss.
See also: Natural Hair Supplement: Friend or Foe? Saw Palmetto, a Systematic Review in Alopecia
Hair today… Growing tomorrow!
So, what was that about increasing T levels?
Men usually suffer declining T levels as they get older, with a marked drop around the age of 45. With lower T comes lower energy, lower mood, lower libido, erectile dysfunction, etc.
Guess what… It’s T that’s needed for those things, not DHT. So if you block the conversion of T to DHT, you’ll have higher blood serum T levels, higher energy, higher mood, higher libido, and all that.
(the above assumes you have testicles, without which, your T levels will certainly not increase)
Saw Palmetto Against Enlarged Prostate?
With higher DHT levels in mid-late life, prostate enlargement (benign prostatic hyperlasia) can become a problem for many men. The size of that problem ranges from urinary inconvenience (common, when the prostate presses against the bladder) to prostate cancer (less common, much more serious). Saw palmetto, like other 5α-reductase inhibitors such as finasteride, may be used to prevent or treat this.
Wondering how safe/reliable it is? We found a very high-quality fifteen-year longitudinal observational study of the use of saw palmetto, and it found:
❝The 15 years’ study results suggest that taking S. repens plant extract continuously at a daily dose of 320 mg is an effective and safe way to prevent the progression of benign prostatic hyperplasia.❞
Want a second opinion? We also found a 10-year study (by different researchers with different people taking it), which reached the same conclusion:
❝The results of study showed the absence of progression, both on subjective criteria (IPSS, and QoL scores), and objective criteria (prostate volume, the rate of urination, residual urine volume). Furthermore, patients had no undesirable effects directly related to the use of this drug.❞
- IPSS = International Prostate Symptom Score
- QoL = Quality of Life
❝But wait a minute; I, a man over the age of 45 with potentially declining T levels but a fabulous beard, remember that you said just a minute ago that saw palmetto is used by women to avoid having facial hair; I don’t want to lose mine!❞
You won’t. Once your facial hair follicles were fully developed and activated during puberty, they’ll carry on doing what they do for life. That’s no longer regulated by hormones once they’re up and running.
The use of saw palmetto can only be used to limit facial hair if caught early—so it’s more useful at the onset of menopause, for those who have (or will have) such, or else upon the arrival of PCOS symptoms or hirsuitism from some other cause.
Take The Test!
Do you have a prostate, and would like to know your IPSS score, and what that means for your prostate health?
(takes 1 minute, no need to pee or go probing for anything)
Bottom Line on Saw Palmetto
- It blocks the conversion of T into DHT
- It will increase blood serum T levels, thus boosting mood, energy, libido, etc in men (who typically have more T, but whose T levels decline with age)
- It will decrease DHT levels, thus limiting hair loss (especially in men) and later-life new facial hair growth (especially in women).
- It can be used to prevent or treat prostate enlargement
- Bonus: it’s a potent antioxidant and thus reduces general inflammation (in everyone)
Want To Try Saw Palmetto?
We don’t sell it (or anything else), but for your convenience…
Share This Post
- Testosterone (henceforth, “T”) is produced in the human body.



-

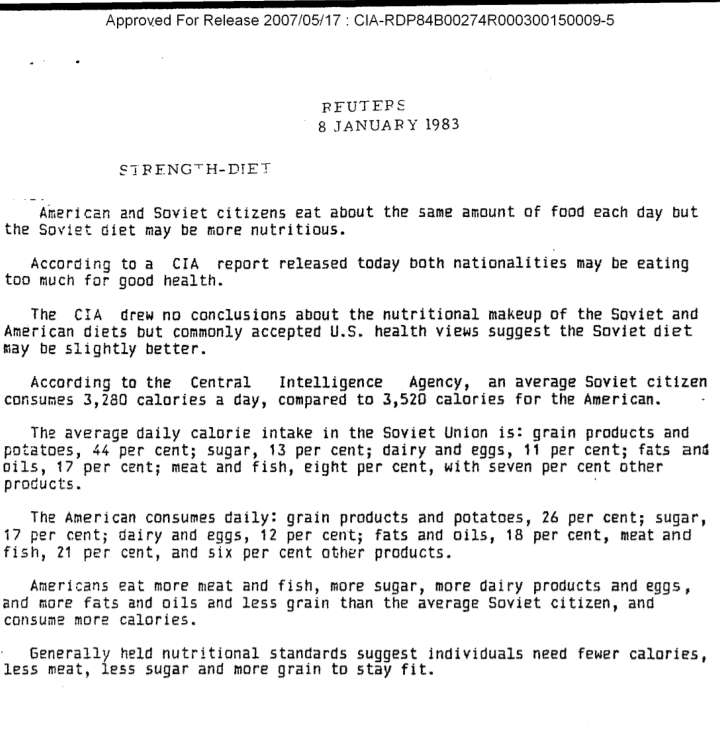
Revealed: The Soviet Secret Recipe For Success That The CIA Admits Put The US To Shame
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Today’s edition of 10almonds brings you a blast from the past with a modern twist: an ancient Russian peasant food that became a Soviet staple, and today, is almost unknown in the West.
Before we get to that, let’s take a sneaky look at this declassified CIA memorandum from near the end of the Cold War:

(Click here to see a bigger version)
The take-away here is:
- Americans were eating 2–3 times more meat than Soviets
- Soviets were eating nearly double the amount of grain products and potatoes
…and both of these statistics meant that nutritionally speaking, the Soviets were doing better.
Americans also consumed more sugar and fats, which again, wasn’t the best dietary option.
But was the American diet tastier? Depends on whom you ask.
Which brings us to a literal recipe we’re going to be sharing with you today:
It’s not well-known in the West, but in Russia, it’s a famous national comfort food, a bastion of health and nutrition, and it rose to popularity because it was not only cheap and nutritious, but also, you could eat it for days without getting sick of it. And it could be easily frozen for reheating later without losing any of its appeal—it’d still be just as good.
In Russia there are sayings about it:
Щи да каша — пища наша (Shchi da kasha — pishcha nasha)
“Shchi and buckwheat are what we eat”
Top tip: buckwheat makes an excellent (and naturally sweet) alternative to porridge oats if prepared the same way!
Где щи, там и нас ищи (Gdye shchi, tam i nas ishchi)
“Where there’s shchi, us you’ll see”
Голь голью, а луковка во щах есть (Gol’ gol’yu, a lukovka vo shchakh yest’)
“I’m stark naked, but there’s shchi with onions”
There’s a very strong sentiment in Russia that really, all you need is shchi (shchi, shchi… shchi is all you need )
But what, you may ask, is shchi?
Our culinary cultural ambassador Nastja is here to offer her tried-and-tested recipe for…

…Russian cabbage soup (yes, really—bear with us now, and you can thank us later)
There are a lot of recipes for shchi (see for yourself what the Russian version of Lifehacker recommends), and we’ll be offering our favorite…
Nastja’s Nutritious and Delicious Homemade Shchi
Hi, Nastja here! I’m going to share with you my shchi recipe that is:
- Cheap
- So tasty
- Super nutritious*
- Vegan
- Gluten Free
You will also need:
- A cabbage (I use sweetheart, but any white cabbage will do)
- 1 cup (250g) red lentils (other kinds of lentils will work too)
- ½ lb or so (250–300g) tomatoes (I use baby plum tomatoes, but any kind will do)
- ½ lb or so (250–300g) mushrooms (the edible kind)
- An onion (I use a brown onion; any kind will do)
- Salt, pepper, rosemary, thyme, parsley, cumin
- Marmite or similar yeast extract (do you hate it? Me too. Trust me, it’ll be fine, you’ll love it. Omit if you’re a coward.)
- A little oil for sautéing (I use sunflower, but canola is fine, as is soy oil. Do not use olive oil or coconut oil, because the taste is too strong and the flashpoint too low)
First, what the French call mise-en-place, the prep work:
- Chop the cabbage into small strips, ⅛–¼ inch x 1 inch is a good guideline, but you can’t really go wrong unless you go to extremes
- Chop the tomatoes. If you’re using baby plum tomatoes (or cherry tomatoes), cut them in half. If using larger tomatoes, cut them into eighths (halve them, halve the halves, then halve the quarters)
- Chop the mushrooms. If using button mushrooms, half them. If using larger mushrooms, quarter them.
- Chop the onion finely.
- Gather the following kitchenware: A big pan (stock pot or similar), a sauté pan (a big wok or frying pan will do), a small frying pan (here a wok will not do), and a saucepan (a rice cook will also do)
Now, for actual cooking:
- Cook the red lentils until soft (I use a rice cooker, but a saucepan is fine) and set aside
- Sauté the cabbage, put it in the big pot (not yet on the heat!)
- Fry the mushrooms, put them in the big pot (still not yet on the heat!)
When you’ve done this a few times and/or if you’re feeling confident, you can do the above simultaneously to save time
- Blend the lentils into the water you cooked them in, and then add to the big pot.
- Turn the heat on low, and if necessary, add more water to make it into a rich soup
- Add the seasonings to taste, except the parsley. Go easy on the cumin, be generous with the rosemary and thyme, let your heart guide you with the salt and pepper.
- When it comes to the yeast extract: add about one teaspoon and stir it into the pot. Even if you don’t like Marmite, it barely changes the flavour (makes it slightly richer) and adds a healthy dose of vitamin B12.
We did not forget the tomatoes and the onion:
- Caramelize the onion (keep an eye on the big pot) and set it aside
- Fry the tomatoes and add them to the big pot
Last but definitely not least:
- Serve!
- The caramelized onion is a garnish, so put a little on top of each bowl of shchi
- The parsley is also a garnish, just add a little
Any shchi you don’t eat today will keep in the fridge for several days, or in the freezer for much longer.
*That nutritious goodness I talked about? Check it out:
- Lentils are high in protein and iron
- Cabbage is high in vitamin C and calcium
- Mushrooms are high in magnesium
- Tomatoes are good against inflammation
- Black pepper has a host of health benefits
- Yeast extract contains vitamin B12
Let us know how it went! We love to receive emails from our subscribers!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Avocado vs Jackfruit – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing avocado to jackfruit, we picked the avocado.
Why?
In terms of macros, avocado is higher in fats (famously healthy ones, including a good dose of omega-3), fiber (nearly 5x more), and protein (despite jackfruit being more often used as a meaty element in recipes, avocado has slightly more). Meanwhile, jackfruit is about 3x higher in carbs. All in all, a clear win for avocado.
Looking at vitamins, avocado has more of vitamins A, B2, B3, B5, B7, B9, E, K, and choline, while jackfruit has more of vitamins B1, B6, and C. Another win for avocado in this category.
In the category of minerals, avocado has more copper, iron, manganese, phosphorus, potassium, selenium, and zinc, while jackfruit has more calcium. One more win for avocado.
Adding up the sections makes for an easy overall win for avocado, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Jackfruit vs Durian – Which is Healthier? ← including some fun durian facts (such as how to pick a good one, and what happens if you eat durian and drink alcohol)
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What Actually Causes High Cholesterol?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 1968, the American Heart Association advised limiting egg consumption to three per week due to cholesterol concerns linked to cardiovascular disease. Which was reasonable based on the evidence available back then, but it didn’t stand the test of time.
Eggs are indeed high in cholesterol, but that doesn’t mean that those who eat them will also be high in cholesterol, because…
It’s not quite what many people think
Some quite dietary pointers to start with:
- Egg yolks are high in cholesterol but have a minimal impact on blood cholesterol.
- Saturated and trans fats (as found in fatty meats or dairy, and some processed foods) have a greater influence on LDL levels than dietary cholesterol.
And on the other hand:
- Unsaturated fats (e.g. from fish, nuts, seeds) have anti-inflammatory benefits
- Fiber-rich foods help lower LDL by affecting fat absorption in the digestive tract
A quick primer on LDL and other kinds of cholesterol:
- VLDL (Very Low-Density Lipoprotein):
- delivers triglycerides and cholesterol to muscle and fat cells for energy
- is converted into LDL after delivery
- LDL (Low-Density Lipoprotein):
- is called “bad cholesterol”, which we call that due to its role in arterial plaque formation
- in excess leads to inflammation, overworked macrophage activity, and artery narrowing
- HDL (High-Density Lipoprotein):
- known as “good cholesterol,” picks up excess LDL and returns it to the liver for excretion
- is anti-inflammatory, in addition to regulating LDL levels
There are other factors too, for example:
- Smoking and drinking increase LDL buildup and cause oxidative damage to lipids in general and the blood vessels through which they travel
- Regular exercise, meanwhile, can lower LDL and raise HDL
- Statins and other medications can help lower LDL and manage cholesterol when lifestyle changes and genetics require additional support—but they often come with serious side effects, and the usefulness varies from person to person.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: