Hearing voices is common and can be distressing. Virtual reality might help us meet and ‘treat’ them
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Have you ever heard something that others cannot – such as your name being called? Hearing voices or other noises that aren’t there is very common. About 10% of people report experiencing auditory hallucinations at some point in their life.
The experience of hearing voices can be very different from person to person, and can change over time. They might be the voice of someone familiar or unknown. There might be many voices, or just one or two. They can be loud or quiet like a whisper.
For some people these experiences are positive. They might represent a spiritual or supernatural experience they welcome or a comforting presence. But for others these experiences are distressing. Voices can be intrusive, negative, critical or threatening. Difficult voices can make a person feel worried, frightened, embarrassed or frustrated. They can also make it hard to concentrate, be around other people and get in the way of day-to-day activities.
Although not everyone who hears voices has a mental health problem, these experiences are much more common in people who do. They have been considered a hallmark symptom of schizophrenia, which affects about 24 million people worldwide.
However, such experiences are also common in other mental health problems, particularly in mood- and trauma-related disorders (such as bipolar disorder or depression and post-traumatic stress disorder) where as many as half of people may experience them.

Why do people hear voices?
It is unclear exactly why people hear voices but exposure to prolonged stress, trauma or depression can increase the chances.
Some research suggests people who hear voices might have brains that are “wired” differently, particularly between the hearing and speaking parts of the brain. This may mean parts of our inner speech can be experienced as external voices. So, having the thought “you are useless” when something goes wrong might be experienced as an external person speaking the words.
Other research suggests it may relate to how our brains use past experiences as a template to make sense of and make predictions about the world. Sometimes those templates can be so strong they lead to errors in how we experience what is going on around us, including hearing things our brain is “expecting” rather than what is really happening.
What is clear is that when people tell us they are hearing voices, they really are! Their brain perceives voice experiences as if someone were talking in the room. We could think of this “mistake” as working a bit like being susceptible to common optical tricks or visual illusions.

Coping with hearing voices
When hearing voices is getting in the way of life, treatment guidelines recommend the use of medications. But roughly a third of people will experience ongoing distress. As such, treatment guidelines also recommend the use of psychological therapies such as cognitive behavioural therapy.
The next generation of psychological therapies are beginning to use digital technologies and virtual reality offers a promising new medium.
Avatar therapy allows a person to create a virtual representation of the voice or voices, which looks and sounds like what they are experiencing. This can help people regain power in the “relationship” as they interact with the voice character, supported by a therapist.
Jason’s experience
Aged 53, Jason (not his real name) had struggled with persistent voices since his early 20s. Antipsychotic medication had helped him to some extent over the years, but he was still living with distressing voices. Jason tried out avatar therapy as part of a research trial.
He was initially unable to stand up to the voices, but he slowly gained confidence and tested out different ways of responding to the avatar and voices with his therapist’s support.
Jason became more able to set boundaries, such as not listening to them for periods throughout the day. He also felt more able to challenge what they said and make his own choices.
Over a couple of months, Jason started to experience some breaks from the voices each day and his relationship with them started to change. They were no longer like bullies, but more like critical friends pointing out things he could consider or be aware of.

Gaining recognition
Following promising results overseas and its recommendation by the United Kingdom’s National Institute for Health and Care Excellence, our team has begun adapting the therapy for an Australian context.
We are trialling delivering avatar therapy from our specialist voices clinic via telehealth. We are also testing whether avatar therapy is more effective than the current standard therapy for hearing voices, based on cognitive behavioural therapy.
As only a minority of people with psychosis receive specialist psychological therapy for hearing voices, we hope our trial will support scaling up these new treatments to be available more routinely across the country.
We would like to acknowledge the advice and input of Dr Nadine Keen (consultant clinical psychologist at South London and Maudsley NHS Foundation Trust, UK) on this article.
Leila Jameel, Trial Co-ordinator and Research Therapist, Swinburne University of Technology; Imogen Bell, Senior Research Fellow and Psychologist, The University of Melbourne; Neil Thomas, Professor of Clinical Psychology, Swinburne University of Technology, and Rachel Brand, Senior Lecturer in Clinical Psychology, University of the Sunshine Coast
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

3 Ways To Increase Your Push-Ups (In Just 30-Days!)

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowitz, of “Strong at Every Age”, shows us how:
Pushing it up
A lot of people who struggle with push-ups will do make-it-easier modifications; doing them one one’s knees is a popular one, for example. However, more reps of a modified push-up only makes you stronger at that modification, not at the full push-up.
So, how to get around this problem?
Three ways:
- Cluster sets: do 3–5 rounds at the start of your workout; set a target of 6–10 total reps per round, and do 1–3 reps of the hardest variation you can, resting 15–30 seconds between mini-sets until the round is complete (rest for at least a minute between rounds).
- Slow eccentric push-ups: for 3–5 seconds, focus only on lowering yourself down, then reset at the top. This lets you train harder variations and build control even if you can’t push back up yet.
- Push-up holds: hold the push-up at weak points (e.g. bottom, halfway, or top—whatever it is for you) to build slow-twitch tension and improve your form (so that you no longer find yourself wobbly). This helps develop mind–muscle connection, which in turn helps pretty much all other parts of this endeavor.
For an extra upwards push, you can combine these three ways with incline push-ups. As a very strong general rule, it’s almost always better to push towards harder variations rather than higher reps of the same easier version.
Why “almost always”? Well, if you’re doing some push-up challenge and specifically want to do very many reps for the sake of it, then building rep count will be what you want. But for anything that’s not “high reps for the sake high reps”, the above method will stand you in better stead.
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post
-

What Most People Don’t Know About HIV
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What To Know About HIV This World AIDS Day

Yesterday, we asked 10almonds readers to engage in a hypothetical thought experiment with us, and putting aside for a moment any reason you might feel the scenario wouldn’t apply for you, asked:
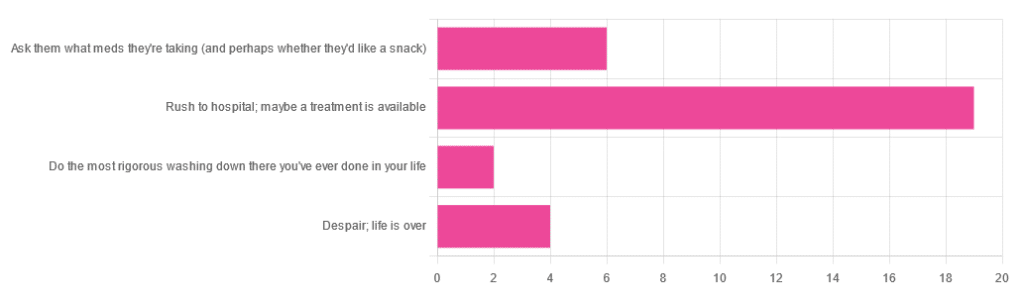
❝You have unprotected sex with someone who, afterwards, conversationally mentions their HIV+ status. Do you…❞
…and got the above-depicted, below-described, set of responses. Of those who responded…
- Just over 60% said “rush to hospital; maybe a treatment is available”
- Just under 20% said “ask them what meds they’re taking (and perhaps whether they’d like a snack)”
- Just over 10% said “despair; life is over”
- Two people said “do the most rigorous washing down there you’ve ever done in your life”
So, what does science say about it?
First, a quick note on terms
- HIV is the Human Immunodeficiency Virus. It does what it says on the tin; it gives humans immunodeficiency. Like many viruses that have become epidemic in humans, it started off in animals (called SIV, because there was no “H” involved yet), which were then eaten by humans, passing the virus to us when it one day mutated to allow that.
- It’s technically two viruses, but that’s beyond the scope of today’s article; for our purposes they are the same. HIV-1 is more virulent and infectious than HIV-2, and is the kind more commonly found in most of the world.
- AIDS is Acquired Immunodeficiency Syndrome, and again, is what it sounds like. When a person is infected with HIV, then without treatment, they will often develop AIDS.
- Technically AIDS itself doesn’t kill people; it just renders people near-defenseless to opportunistic infections (and immune-related diseases such as cancer), since one no longer has a properly working immune system. Common causes of death in AIDS patients include cancer, influenza, pneumonia, and tuberculosis.
People who contract HIV will usually develop AIDS if untreated. Untreated life expectancy is about 11 years.
HIV/AIDS are only a problem for gay people: True or False?
False, unequivocally. Anyone can get HIV and develop AIDS.
The reason it’s more associated with gay men, aside from homophobia, is that since penetrative sex is more likely to pass it on, then if we go with the statistically most likely arrangements here:
- If a man penetrates a woman and passes on HIV, that woman will probably not go on to penetrate someone else
- If a man penetrates a man and passes on HIV, that man could go on to penetrate someone else—and so on
- This means that without any difference in safety practices or promiscuity, it’s going to spread more between men on average, by simple mathematics.
- This is why “men who have sex with men” is the generally-designated higher-risk category.
There is medication to cure HIV/AIDS: True or False?
False so far (though there have been individual case studies of gene treatments that may have cured people—time will tell).
But! There are medications that can prevent HIV from being a life-threatening problem:
- PrEP (Pre-Exposure Prophylaxis) is a medication that one can take in advance of potential exposure to HIV, to guard against it.
- This is a common choice for people aren’t sure about their partners’ statuses, or people working in risky environments.
- PEP (Post-Exposure Prophylaxis) is a medication that one can take after potential exposure to HIV, to “nip it in the bud”.
- Those of you who were rushing to hospital in our poll, this is what you’re rushing there for.
- ARVs (Anti-RetroVirals) are a class of medications (there are different options; we don’t have room to distinguish them) that reduce an HIV+ person’s viral load to undetectable levels.
- Those of you who were asking what meds your partner was taking, these will be those meds. Also, most of them are to be taken in the morning with food, so that’s what the snack was for.
If someone is HIV+, the risk of transmission in unprotected sex is high: True or False?
True or False, with false being the far more likely. It depends on their medications, and this is why you were asking. If someone is on ARVs and their viral load is undetectable (as is usual once someone has been on ARVs for 6 months), they cannot transmit HIV to you.
U=U is not a fancy new emoticon, it means “undetectable = untransmittable”, which is a mathematically true statement in the case of HIV viral loads.
See: NIH | HIV Undetectable=Untransmittable (U=U)
If you’re thinking “still sounds risky to me”, then consider this:
You are safer having unprotected sex with someone who is HIV+ and on ARVs with an undetectable viral load, than you are with someone you are merely assuming is HIV- (perhaps you assume it because “surely this polite blushing young virgin of a straight man won’t give me cooties” etc)
Note that even your monogamous partner of many decades could accidentally contract HIV due to blood contamination in a hospital or an accident at work etc, so it’s good practice to also get tested after things that involve getting stabbed with needles, cut in a risky environment, etc.
If you’re concerned about potential stigma associated with HIV testing, you can get kits online:
CDC | How do I find an HIV self-test?
(these are usually fingerprick blood tests, and you can either see the results yourself at home immediately, or send it in for analysis, depending on the kit)
If I get HIV, I will get AIDS and die: True or False?
False, assuming you get treatment promptly and keep taking it. So those of you who were at “despair; life is over” can breathe a sigh of relief now.
However, if you get HIV, it does currently mean you will have to take those meds every day for the rest of your (no reason it shouldn’t be long and happy) life.
So, HIV is definitely still something to avoid, because it’s not great to have to take a life-saving medication every day. For a little insight as to what that might be like:
HIV.gov | Taking HIV Medication Every Day: Tips & Challenges
(as you’ll see there, there are also longer-lasting injections available instead of daily pulls, but those are much less widely available)
Summary
Some quick take-away notes-in-a-nutshell:
- Getting HIV may have been a death sentence in the 1980s, but nowadays it’s been relegated to the level of “serious inconvenience”.
- Happily, it is very preventable, with PrEP, PEP, and viral loads so low that they can’t transmit HIV, thanks to ARVs.
- Washing will not help, by the way. Safe sex will, though!
- As will celibacy and/or sexual exclusivity in seroconcordant relationships, e.g. you have the same (known! That means actually tested recently! Not just assumed!) HIV status as each other.
- If you do get it, it is very manageable with ARVs, but prevention is better than treatment
- There is no certain cure—yet. Some people (small number of case studies) may have been cured already with gene therapy, but we can’t know for sure yet.
Want to know more? Check out:
Take care!
Share This Post
-
Is spinal cord stimulation safe? Does it work? Here’s what you need to know if you have back pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Spinal cord stimulators are electrical devices that are surgically implanted in the body to treat long-term pain. They have a battery pack and leads that deliver electrical impulses directly to the spinal cord. The devices are thought to work by providing electrical impulses that interfere with how the brain senses pain.
Spinal cord stimulators are mainly used to treat chronic back pain, especially when other less invasive treatments have not worked. They also aim to reduce people’s reliance on risky pain medicines. These include opioids, which research shows are ineffective and harmful for low-back pain.
But research, including our own, shows spinal cord stimulators work no better than a placebo. And they can also carry risks.

AsiaVision/Getty Do they work?
In a 2023 Cochrane review, researchers reviewed data from 13 randomised controlled trials on low-back pain and found no benefits in the short and medium term. These international reviews draw together the most robust evidence to provide a detailed summary of what we know on a particular topic.
Only one of the trials in the review tested efficacy in the longer term (six months). That trial found no benefits of spinal cord stimulation.
An earlier Cochrane review looked at the evidence of spinal cord stimulation for chronic pain in general, including for neck pain. Reviewers looked at 15 randomised controlled trials and couldn’t be certain about its benefits, largely due to the quality and reliability of the available trials.
Are there side effects?
Aside from disappointing results for pain relief, there are risks and side effects to consider.
We co-authored an analysis of 520 adverse events reported to Australia’s Therapeutic Goods Administration (TGA). We found 79% of reported events were rated as severe, with 13% life-threatening. The same research found 80% of events required surgery to correct.
Our recent analysis in the Medical Journal of Australia looked at data from private health insurers. These cover 90% of spinal cord stimulation implants in Australia. Five major insurers, which covered 76% of privately insured people, contributed de-identified data.
We found about one-quarter of people who had a spinal cord stimulator implanted needed corrective surgery afterwards. These surgeries occurred within a median of about 17 months. This indicates these surgeries are not routine or expected interventions, such as to replace batteries, which are meant to last five to ten years.
Our previous research shows the sorts of reasons for corrective surgery. These include to replace a malfunctioning device, or the person was in more pain, had an infection, or a puncture of the delicate tissues covering the spinal cord.
However, even our latest findings are likely to underestimate the risk of these devices.
Sometimes the lead delivering the electrical current moves away from the spinal cord to elsewhere in the body. This requires surgery to reposition the lead, but does not necessarily require new hardware, such as a brand new lead. So this type of corrective surgery is not counted in the data from the private health insurance companies.
How much does it cost?
We found spinal cord stimulators cost about A$55,000 per patient, including the device, its insertion, and managing any associated additional surgeries.
For people who only had a “trial” – where the leads are implanted temporarily but the battery pack remains outside the body – this cost was about $14,000 per patient.
These figures do not include any out-of-pocket costs.
What do regulators say about the devices?
In 2022 the TGA began a review of spinal cord stimulators on the market because of safety and performance concerns.
As a result, several devices were removed from the Australian Register of Therapeutic Goods – that is, they were banned from use in Australia, but existing stock could still be used.
The rest of the devices had conditions imposed, such as the manufacturers being required to collect and report safety data to the TGA at regular time points.
Should I do my own online research?
Yes, but be careful. Unfortunately not all online information about spinal cord stimulators is correct.
Look for sites independent of those who manufacture or implant these devices.
Government agencies, health departments and universities that have no financial interests in this area may be a better option.
The Cochrane Library is also a reliable and independent source for trustworthy health information.
What shall I ask my doctor?
The Australian health department provides useful advice for consumers about medical implants.
It says medical implants “are considered higher-risk therapeutic goods, and the decision to get one should not be taken lightly”. It recommends asking your health professional these questions:
- do I really need this medical implant?
- what are the risks/benefits?
- is the medical implant approved?
- where can I get more information?
- what happens if I experience an adverse event?
What else could I do for my back pain?
There are other treatment options that are effective and have fewer risks than spinal cord stimulation.
For example, education about how to manage your pain yourself, exercise, cognitive behavioural therapy (a type of psychological therapy), and non-steroidal anti-inflammatory medicines (such as ibuprofen) all have solid evidence to back them. All offer benefits that are not outweighed by their potential risks.
Australian research has shown other types of therapy – such as sensorimotor retraining and cognitive functional therapy – are also effective. You can discuss these and other options with your health professional.
Spinal cord stimulation is a good example of a treatment that got ahead of the evidence. Although the devices have been around since the 1960s, we’ve only had reliable trials to test whether they work in recent years.
Everyone wants to find ways to help people with chronic pain, but we must ensure medical care is grounded in reliable science.
Caitlin Jones, Postdoctoral Research Associate in Musculoskeletal Health, University of Sydney and Christopher Maher, Professor, Sydney School of Public Health, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-
The Surprising Relationship Between Glucosamine & Alzheimer’s
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Glucosamine is popularly taken for joint health,
and it really is the best thing out there for that.No wait, it’s not: Cucumber Extract Beats Glucosamine & Chondroitin… At 1/135th Of The Dose?!
Today, we’re not doing glucosamine’s PR any favors, but well, we’re a health science publication and the truth is there may be a problem:
Glucosamine, hyperglycosylation, & you
Researchers (Dr. Tara Hawkinson et al.) analyzed thousands of US health records, and found that glucosamine use was associated with:
- 25% higher likelihood of progressing from mild cognitive impairment (MCI) to dementia
- 25% higher mortality risk among people who already had Alzheimer’s disease or related dementias.
Among the patients studied, about 8% reported taking glucosamine supplements, including 2,750 people with MCI and 1,896 people with dementia.
And as for how this happened?
Dr. Hawkinson and her team found that excessive protein glycosylation (the attachment of sugar structures to proteins) appeared to be a significant driver of Alzheimer’s disease progression, suggesting that glucosamine may worsen an already overactive “sugar-tagging pathway” in the Alzheimer’s brain.
Now, that data was from humans, and/but this was an observational retrospective study, meaning it couldn’t prove cause and effect by itself.
However, when they went on to test it in mice with Alzheimer’s disease, glucosamine increased protein glycosylation and worsened social-memory performance, while suppressing glycosylation improved memory.
Back to humans: examination of post-mortem Alzheimer’s brain tissue showed significantly higher levels of protein glycosylation than in non-Alzheimer’s control brains, further supporting the idea that this pathway likely contributes to disease progression.
This is important, because glucosamine has often been considered relatively safe and has even been linked in some studies to lower risks of certain chronic diseases, but this research suggests that effects may depend on the disease context, and quite possibly may be harmful in the context of Alzheimer’s disease.
In other words:
❝A lot of these people actively take an over-the-counter supplement that could be making their disease progression worse.❞
~ Dr. Ramon Sun, a colleague of Dr. Hawkinson and fellow researcher in this study
You can read the paper itself, here: Hyperglycosylation is a metabolic driver of Alzheimer’s disease ← notice the bold statement in the title; scientists are very reticent to make concrete claims without concrete evidence. Here, they are expressing their strong clear finding that hyperglycosylation is a metabolic driver or Alzheimer’s disease.
Want to learn more?
We’ve written quite a bit about reducing the risk of cognitive decline in general and Alzheimer’s in particular; here are just a few:
- Alzheimer’s Causative Factors To Avoid
- How To Reduce Your Alzheimer’s Risk
- How To Walk Away From Alzheimer’s
- How To Clean Your Brain (Glymphatic Health Primer)
- Take Care Of Your Lymphatic System To Beat Cognitive Decline
- Goodnight, Glymphatic System: How Your Sleep Position Changes Dementia Risk
- The 6 Dimensions Of Sleep (And Why They Matter)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Power Vegan Meals – by Maya Sozer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book has inspired some of the recipes we’ve shared recently—we’ve invariably tweaked and in our opinion improved them, but the recipes are great as written too.
The recipes, of which there are 75, are all vegan, gluten-free, high protein, and high fiber. Some reviewers on Amazon have complained that the recipes are high-calorie, and they often are, but those calories are mostly from healthy fats, so we don’t think it’s a bad thing. Still, if you’re doing a strict calorie-controlled diet, this is probably not the one for you.
Another thing the recipes are is tasty without being unduly complicated, as well as being mostly free from obscure ingredients. This latter is a good thing not because obscure ingredients are inherently bad, but rather that it can be frustrating to read a recipe and find its star ingredient is a cup of perambulatory periannath that must be harvested from the west-facing slopes of Ithilien during a full moon, no substitutions.
The style and format is simple and clear with minimal overture, one recipe per double-page; picture on one side, recipe on the other; perfect for a kitchen reading-stand.
Bottom line: these recipes are for the most part very consistent with what we share here, and we recommend them, unless you’re looking for low-calorie options.
Click here to check out Power Vegan Meals, and power-up your vegan meals!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Get Past Executive Dysfunction
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In mathematics, there is a thing called the “travelling salesman problem”, and it is hard. Not just subjectively; it is classified in mathematical terms as an “NP-hard problem”, wherein NP stands for “nondeterministic polynomial”.
The problem is: a travelling salesman must visit a certain list of cities, order undetermined, by the shortest possible route that visits them all.
To work out what the shortest route is involves either very advanced mathematics, or else solving it by brute force, which means measuring every possible combination order (which number gets exponentially larger very quickly after the first few cities) and then selecting the shortest.
Why are we telling you this?
Executive dysfunction’s analysis paralysis
Executive dysfunction is the state of knowing you have things to do, wanting to do them, intending to do them, and then simply not doing them.
Colloquially, this can be called “analysis paralysis” and is considered a problem of planning and organizing, as much as it is a problem of initiating tasks.
Let’s give a simple example:
You wake up in the morning, and you need to go to the bathroom. But the bathroom will be cold, so you’ll want to get dressed first. However, it will be uncomfortable to get dressed while you still need to use the bathroom, so you contemplate doing that first. Those two items are already a closed loop now. You’re thirsty, so you want to have a drink, but the bathroom is calling to you. Sitting up, it’s colder than under the covers, so you think about getting dressed. Maybe you should have just a sip of water first. What else do you need to do today anyway? You grab your phone to check, drink untouched, clothes unselected, bathroom unvisited.
That was a simple example; now apply that to other parts of your day that have much more complex planning possible.
This is like the travelling salesman problem, except that now, some things are better if done before or after certain other things. Sometimes, possibly, they are outright required to be done before or after certain other things.
So you have four options:
- Solve the problem of your travelling-salesman-like tasklist using advanced mathematics (good luck if you don’t have advanced mathematics)
- Solve the problem by brute force, calculating all possible variations and selecting the shortest (good luck getting that done the same day)
- Go with a gut feeling and stick to it (people without executive dysfunction do this)
- Go towards the nearest item, notice another item on the way, go towards that, notice a different item on the way there, and another one, get stuck for a while choosing between those two, head towards one, notice another one, and so on until you’ve done a very long scenic curly route that has narrowly missed all of your targetted items (this is the executive dysfunction approach).
So instead, just pick one, do it, pick another one, do it, and so forth.
That may seem “easier said than done”, but there are tools available…
Task zero
We’ve mentioned this before in the little section at the top of our daily newsletter that we often use for tips.
One of the problems that leads to executive function is a shortage of “working memory”, like the RAM of a computer, so it’s easy to get overwhelmed with lists of things to do.
So instead, hold only two items in your mind:
- Task zero: the thing you are doing right now
- Task one: the thing you plan to do next
When you’ve completed task zero, move on to task one, renaming it task zero, and select a new task one.
With this approach, you will never:
- Think “what did I come into this room for?”
- Get distracted by alluring side-quests
Do not get corrupted by the cursed artefact
In fantasy, and occasionally science fiction, there is a trope: an item that people are drawn towards, but which corrupts them, changes their motivations and behaviors for the worse, as well as making them resistant to giving the item up.
An archetypal example of this would be the One Ring from The Lord of the Rings.
It’s easy to read/watch and think “well I would simply not be corrupted by the cursed artefact”.
And then pick up one’s phone to open the same three apps in a cycle for the next 40 minutes.
This is because technology that is designed to be addictive hijacks our dopamine processing, and takes advantage of executive dysfunction, while worsening it.
There are some ways to mitigate this:
Rebalancing Dopamine (Without “Dopamine Fasting”)
…but one way to avoid it entirely is to mentally narrate your choices. It’s a lot harder to make bad choices with an internal narrator going:
- “She picked up her phone absent-mindedly, certain that this time it really would be only a few seconds”
- “She picked up her phone for the eleventy-third time”
- “Despite her plan to put her shoes on, she headed instead for the kitchen”
This method also helps against other bad choices aside from those pertaining to executive dysfunction, too:
- “Abandoning her plan to eat healthily, she lingered in the confectionary aisle, scanning the shelves for sugary treats”
- “Monday morning will be the best time to start my new exercise regime”, she thought, for the 35th week so far this year
Get pharmaceutical or nutraceutical help
While it’s not for everyone, many people with executive dysfunction benefit from ADHD meds. However, they have their pros and cons (perhaps we’ll do a run-down one of these days).
There are also gentler options that can significantly ameliorate executive dysfunction, for example:
Bacopa Monnieri: A Well-Evidenced Cognitive Enhancer For Focus & More
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: