5 reasons we shouldn’t ‘compliment’ people who lose weight
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“You look so great! Have you lost weight?”
“Wow, you’re looking so healthy now! Good for you.”
As fat people, we’ve heard comments like this for most of our lives. At the times when our bodies were smaller, these comments made us feel proud and accepted. We felt like we were finally “good enough”.
But when we regained the weight, as happens for most people, we felt like our bodies were no longer “good enough” and that these well-intentioned comments were in fact harmful.
Through our work as size- and weight-inclusive researchers, we’ve come to understand it wasn’t just us – the extent of harm from comments such as these is far-reaching.
Both positive and negative comments about weight can lead to negative outcomes. Whether they lose weight or not, larger-bodied people are judged and criticised.
Women’s weight in particular is policed and considered fair game for comment. Consider the commentary about the recent weight loss of celebrities such as Lizzo and Serena Williams.
The effects can be even worse for those with multiple marginalised identities across race or ethnicity, gender, class and ability.
It’s time we stop “complimenting” weight loss, even when well-intentioned. Here’s why – and what to do instead.

5 reasons why ‘complimenting’ weight loss can harm
1. It reinforces weight stigma
Complimenting weight loss sends the message that smaller bodies are better, and contributes to negative attitudes, beliefs and stereotypes about larger-bodied people.
This leads to unfair treatment of larger-bodied people in places such as school, work and social settings. For example, larger-bodied people, especially women, are often seen as less suitable for jobs.
These negative views can also be internalised, causing larger-bodied people to believe they are less deserving of respect or fair treatment because of their body size.
2. It links worth with appearance
Praising someone for losing weight reinforces the belief that the most important aspect of a person is the appearance of a smaller body, rather than valuing other qualities or achievements.
This also impacts children. Family-based weight stigma and parental comments about weight and dieting are associated with higher psychological distress in pre-adolescents and adolescents.
3. It overlooks natural diversity of body size
It holds onto the idea that there is only one “right” way for a body to look, and assumes everyone is aiming to be smaller, rather than recognising that bodies naturally come in all shapes and sizes.
4. It assumes intent
It ignores the fact that sometimes weight loss is unintentional and caused by health issues, stress, abuse, neglect or financial challenges. It’s better not to comment on someone’s body as you might inadvertently be praising illness or distress.
5. It can trigger disordered eating
It can send people who have struggled with their relationship with food back into ways of thinking that they may have worked hard to overcome. This can make old patterns of eating resurface or create new ones, particularly in adolescence, with the harm extending through to adulthood.
What to do instead
We’re not suggesting you stop complimenting people all together, as it can be beneficial to both the people receiving and giving the compliments. As Roman philosopher Lucius Annaeus Seneca once said, “Whenever there is a human being, there is an opportunity for a kindness.”
But we need to ensure our compliments truly are kind and not inadvertently harmful.
Instead of complimenting others on weight loss, share compliments on more important attributes, such as “You have such an infectious laugh” or “I always feel happier after seeing you”. You could also compliment someone on an achievement, such as “I really admire the way you created such a fantastic event.”
Likewise, irrespective of any change in your body weight, focus your self-compliments on improvements in your wellbeing. You could tell yourself “I’m proud of myself for getting stronger” or “It feels great to be more flexible now I’m moving more.”
It’s OK not to respond when someone “compliments” you on weight loss, or even to choose not take on the labour of explaining why it’s harmful. On the days it feels challenging to speak up, be kind to yourself. Try saying something like, “Yeah, I’d rather not talk about my body” or “I promise my weight is the least interesting thing about me.”
If you’re tempted to comment on your own or other people’s weight, learn more about the harms of weight-related comments from larger-bodied people and those who have experienced weight stigma. Organisations such as Size Inclusive Health Australia, the Butterfly Foundation, the Embrace Collective and the National Eating Disorders Collaboration are also good sources of information.
Comments on weight loss stay with you. They can have long-term impacts on your self worth, health and wellbeing, as well as your relationships with your family members, friends and others. So let’s not send the message that a peron’s worth is measured in kilos.
Evangeline Gardiner, PhD Candidate in Public Health, The University of Queensland and Lily O’Hara, Senior Lecturer in Public Health, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The New Menopause – by Dr. Mary Claire Haver

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author is most famous for “The Galveston Diet”, which book is astonishingly similar in its content, chapters, format, etc to Nikki Williams’ “It’s Not You, It’s Your Hormones” which came out a few years previously but didn’t get the same marketing.
Nonetheless, this time Dr. Haver has something new to add, and we think it’s worth a read.
The general theme of this book is a comprehensive overview of the menopause, experientially (subjective to the person going through it) and empirically (by science), from start to finish and beyond. This book’s more about human physiology, and less about diet than the previous.
Dr. Haver also discusses in-depth how estrogen is thought of as a sex hormone (and it is), to the point that people consider it perhaps expendable, and forget (or are simply unaware) that we have estrogen receptors throughout our bodies and estrogen is vital for maintaining many other bodily functions, including your heart, cognitive function, bone integrity, blood sugar balance, and more.
(in case you’re wondering “why don’t men fall to bits, then?”, don’t worry, their testosterone does these things for them. Testosterone is orders of magnitude less potent than estrogen, mg for mg, so they need a lot more of it, but under good conditions they produce plenty so it’s fine)
But, the amount of testosterone available to peri/postmenopausal women is simply not enough to do that job (and it’d also result in a transition of secondary sex characteristics, which for most people would be very unwanted), so, something else needs to be done.
Dr. Haver also discusses in detail the benefits and risks of HRT and how to get/manage them, respectively, with the latest up-to-date research (at time of going to print; the book was published in April 2024).
Bottom line: if you want to know what’s going on with your peri- or post-menopausal body and how it could be better (or if you want to know what’s going on with someone else approaching/experiencing menopause), then this is a top-tier book.
Click here to check out The New Menopause, and know what’s going on and what to do about it!
Share This Post
-

Half of Australians in aged care have depression. Psychological therapy could help
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
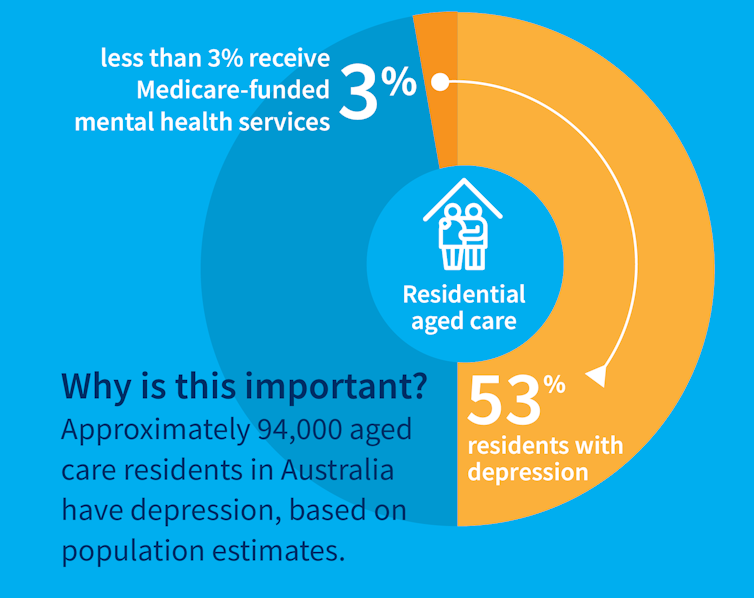
While many people maintain positive emotional wellbeing as they age, around half of older Australians living in residential aged care have significant levels of depression. Symptoms such as low mood, lack of interest or pleasure in life and difficulty sleeping are common.
Rates of depression in aged care appear to be increasing, and without adequate treatment, symptoms can be enduring and significantly impair older adults’ quality of life.
But only a minority of aged care residents with depression receive services specific to the condition. Less than 3% of Australian aged care residents access Medicare-subsidised mental health services, such as consultations with a psychologist or psychiatrist, each year.

Cochrane AustraliaInstead, residents are typically prescribed a medication by their GP to manage their mental health, which they often take for several months or years. A recent study found six in ten Australian aged care residents take antidepressants.
While antidepressant medications may help many people, we lack robust evidence on whether they work for aged care residents with depression. Researchers have described “serious limitations of the current standard of care” in reference to the widespread use of antidepressants to treat frail older people with depression.
Given this, we wanted to find out whether psychological therapies can help manage depression in this group. These treatments address factors contributing to people’s distress and provide them with skills to manage their symptoms and improve their day-to-day lives. But to date researchers, care providers and policy makers haven’t had clear information about their effectiveness for treating depression among older people in residential aged care.
The good news is the evidence we published today suggests psychological therapies may be an effective approach for people living in aged care.
We reviewed the evidence
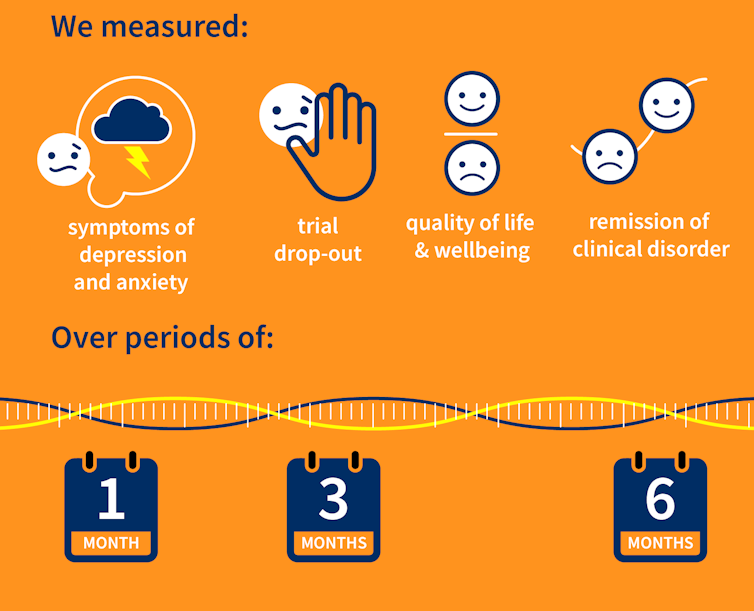
Our research team searched for randomised controlled trials published over the past 40 years that were designed to test the effectiveness of psychological therapies for depression among aged care residents 65 and over. We identified 19 trials from seven countries, including Australia, involving a total of 873 aged care residents with significant symptoms of depression.
The studies tested several different kinds of psychological therapies, which we classified as cognitive behavioural therapy (CBT), behaviour therapy or reminiscence therapy.
CBT involves teaching practical skills to help people re-frame negative thoughts and beliefs, while behaviour therapy aims to modify behaviour patterns by encouraging people with depression to engage in pleasurable and rewarding activities. Reminiscence therapy supports older people to reflect on positive or shared memories, and helps them find meaning in their life history.
The therapies were delivered by a range of professionals, including psychologists, social workers, occupational therapists and trainee therapists.
Cochrane AustraliaIn these studies, psychological therapies were compared to a control group where the older people did not receive psychological therapy. In most studies, this was “usual care” – the care typically provided to aged care residents, which may include access to antidepressants, scheduled activities and help with day-to-day tasks.
In some studies psychological therapy was compared to a situation where the older people received extra social contact, such as visits from a volunteer or joining in a discussion group.
What we found
Our results showed psychological therapies may be effective in reducing symptoms of depression for older people in residential aged care, compared with usual care, with effects lasting up to six months. While we didn’t see the same effect beyond six months, only two of the studies in our review followed people for this length of time, so the data was limited.
Our findings suggest these therapies may also improve quality of life and psychological wellbeing.
Psychological therapies mostly included between two and ten sessions, so the interventions were relatively brief. This is positive in terms of the potential feasibility of delivering psychological therapies at scale. The three different therapy types all appeared to be effective, compared to usual care.
However, we found psychological therapy may not be more effective than extra social contact in reducing symptoms of depression. Older people commonly feel bored, lonely and socially isolated in aged care. The activities on offer are often inadequate to meet their needs for stimulation and interest. So identifying ways to increase meaningful engagement day-to-day could improve the mental health and wellbeing of older people in aged care.
Some limitations
Many of the studies we found were of relatively poor quality, because of small sample sizes and potential risk of bias, for example. So we need more high-quality research to increase our confidence in the findings.
Many of the studies we reviewed were also old, and important gaps remain. For example, we are yet to understand the effectiveness of psychological therapies for people from diverse cultural or linguistic backgrounds.
Separately, we need better research to evaluate the effectiveness of antidepressants among aged care residents.
What needs to happen now?
Depression should not be considered a “normal” experience at this (or any other) stage of life, and those experiencing symptoms should have equal access to a range of effective treatments. The royal commission into aged care highlighted that Australians living in aged care don’t receive enough mental health support and called for this issue to be addressed.
While there have been some efforts to provide psychological services in residential aged care, the unmet need remains very high, and much more must be done.
The focus now needs to shift to how to implement psychological therapies in aged care, by increasing the competencies of the aged care workforce, training the next generation of psychologists to work in this setting, and funding these programs in a cost-effective way.

Tanya Davison, Adjunct professor, Health & Ageing Research Group, Swinburne University of Technology and Sunil Bhar, Professor of Clinical Psychology, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Total Recovery – by Dr. Gary Kaplan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First, know: Dr. Kaplan is an osteopath, and as such, will be mostly approaching things from that angle. That said, he is also board certified in other things too, including family medicine, so he’s by no means a “one-trick pony”, nor are there “when your only tool is a hammer, everything starts to look like a nail” problems to be found here. Instead, the scope of the book is quite broad.
Dr. Kaplan talks us through the diagnostic process that a doctor goes through when presented with a patient, what questions need to be asked and answered—and by this we mean the deeper technical questions, e.g. “what do these symptoms have in common”, and “what mechanism was at work when the pain become chronic”, not the very basic questions asked in the initial debriefing with the patient.
He also asks such questions (and questions like these get chapters devoted to them) as “what if physical traumas build up”, and “what if physical and emotional pain influence each other”, and then examines how to interrupt the vicious cycles that lead to deterioration of one’s condition.
The style of the book is very pop-science and often narrative in its presentation, giving lots of anecdotes to illustrate the principles. It’s a “sit down and read it cover-to-cover” book—or a chapter a day, whatever your preferred pace; the point is, it’s not a “dip directly to the part that answers your immediate question” book; it’s not a textbook or manual.
Bottom line: a lot of this work is about prompting the reader to ask the right questions to get to where we need to be, but there are many illustrative possible conclusions and practical advices to be found and given too, making this a useful read if you and/or a loved one suffers from chronic pain.
Click here to check out Total Recovery, and solve your own mysteries!
Share This Post
-

The Toe-Tapping Tip For Better Balance
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Balance is critical for health especially in older age, since it’s amazing how much else can go dramatically and suddenly wrong after a fall. So, here’s an exercise to give great balance and stability:
How to do it
You will need:
- Something to hold onto, such as a countertop
- A target on the floor, such as a mark or a coin
The steps:
- Lift one leg up, bring your foot forward, and tap the object in front of you.
- Then, bring that foot back to where it started.
- Next, switch to the other leg and tap.
- Alternate between your right and left legs, shifting back and forth.
- Your goal is to do this for 10 repetitions on each leg without holding on.
How it works:
Whenever you tap, you have to lift one leg up and reach it out in front of you. Doing this requires you to stand on one leg while moving a weight (namely: your other leg), which is something many people, especially upon getting older, are hesitant to do. If you’re unable to stand on one leg, let alone move your center of gravity (per the counterbalance of the other leg) while doing so, you may end up shuffling and walking with your feet sliding across the ground—something you really want to avoid.
For more on all of this plus a visual demonstration, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Fall Special ← this is about not falling, or, failing that, minimizing injury if you do
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Lower Cholesterol Naturally
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Lower Cholesterol, Without Statins
We’ll start this off by saying that lowering cholesterol might not, in fact, be critical or even especially helpful for everyone, especially in the case of women. We covered this more in our article about statins:
…which was largely informed by the wealth of data in this book:
The Truth About Statins – by Dr. Barbara H. Roberts
…which in turn, may in fact put a lot of people off statins. We’re not here to tell you don’t use them—they may indeed be useful or even critical for some people, as Dr. Roberts herself also makes makes clear. But rather, we always recommend learning as much as possible about what’s going on, to be able to make the most informed choices when it comes to what often might be literally life-and-death decisions.
On which note, if anyone would like a quick refresher on cholesterol, what it actually is (in its various forms) and what it does, why we need it, the problems it can cause anyway, then here you go:
Now, with all that in mind, we’re going to assume that you, dear reader, would like to know:
- how to lower your LDL cholesterol, and/or
- how to maintain a safe LDL cholesterol level
Because, while the jury’s out on the dangers of high LDL levels for women in particular, it’s clear that for pretty much everyone, maintaining them within well-established safe zones won’t hurt.
Here’s how:
Relax
Or rather, manage your stress. This doesn’t just reduce your acute risk of a heart attack, it also improves your blood metrics along the way, and yes, that includes not just blood pressure and blood sugars, but even triglycerides! Here’s the science for that, complete with numbers:
What are the effects of psychological stress and physical work on blood lipid profiles?
With that in mind, here’s…
How To Manage Chronic Stress (Even While Chronically Stressed)
Not chemically “relaxed”, though
While relaxing is important, drinking alcohol and smoking are unequivocally bad for pretty much everything, and this includes cholesterol levels:
Can We Drink To Good Health? ← this also covers popular beliefs about red wine and heart health, and the answer is no, we cannot
As for smoking, it is good to quit as soon as possible, unless your doctor specifically advises you otherwise (there are occasional situations where something else needs to be dealt with first, but not as many some might like to believe):
Addiction Myths That Are Hard To Quit
If you’re wondering about cannabis (CBD and/or THC), then we’d love to tell you about the effect these things have on heart health in general and cholesterol levels in particular, but the science is far too young (mostly because of the historic, and in some places contemporary, illegality cramping the research), and we could only find small, dubious, mutually contradictory studies so far. So the honest answer is: science doesn’t know this one, yet.
Exercise… But don’t worry, you can still stay relaxed
When it comes to heart health, the most important thing is keeping moving, so getting in those famous 150 minutes per week of moderate exercise is critical, and getting more is ideal.
240 minutes per week is a neat 40 minutes per day, by the way and is very attainable (this writer lives a 20-minute walk away from where she does her daily grocery shopping, thus making for a daily 40-minute round trip, not counting the actual shopping).
See: The Doctor Who Wants Us To Exercise Less, And Move More
If walking is for some reason not practical for you, here’s a whole list of fun options that don’t feel like exercise but are:
Manage your hormones
This one is mostly for menopausal women, though some people with atypical hormonal situations may find it applicable too.
Estrogen protects the heart… Until it doesn’t:
See also: World Menopause Day: Menopause & Cardiovascular Disease Risk
Here’s a great introduction to sorting it out, if necessary:
Dr. Jen Gunter: What You Should Have Been Told About Menopause Beforehand
Eat a heart-healthy diet
Shocking nobody, but it has to be said, for the sake of being methodical. So, what does that look like?
What Matters Most For Your Heart? Eat More (Of This) For Lower Blood Pressure
(it’s fiber in the #1 spot, but there’s a list of most important things there, that’s worth checking out and comparing it to what you habitually eat)
You can also check out the DASH (Dietary Approaches to Stop Hypertension) edition of the Mediterranean diet, here:
Four Ways To Upgrade The Mediterranean Diet
As for saturated fat (and especially trans-fats), the basic answer is to keep them to minimal, but there is room for nuance with saturated fats at least:
Can Saturated Fats Be Healthy?
And lastly, do make sure to get enough omega 3 fatty-acids:
What Omega-3s Really Do For Us
And enjoy plant sterols and stanols! This would need a whole list of their own, so here you go:
Take These To Lower Cholesterol! (Statin Alternatives)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Magic Pill – by Johann Hari
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most well-known for his book “Stolen Focus”, this one’s about GLP-1 receptor agonists drugs, their strengths, and their problems.
In this case, Hari himself opted for Ozempic, and this book chronicles his year-long journey on such, his personal experiences, and those he gathered from others along the way.
From a starting position of being a sedentary enjoyer of junk food with 32% body fat and a 40” waist, he was prompted to act after his similarly-aged, similarly-lifestyled friend Hannah died of a heart attack.
Being the science journalist he is, he also takes us through the history of the development of GLP-1 RAs, which sounds like it should be a very dry topic, but actually it’s very engaging reading.
He also talks us through the side effects, and differently than how scientific papers do. We’re accustomed to reading “nausea” and that’s it; instead we get a lengthy description of dry-heaving next to a potted plant in Zürich airport while onlookers assumed he was drunk, we hear about belching up bile, of accidentally taking a double-dose and being too ill to leave the house for several days, making it only the distance from the bed to the bathtub.
We hear, in short, about the disruption to normal life, in a way that adds a little color to the “many people stop because of the side effects”.
A lot of the book is also given over to the psychology and sociology of it, as much as the hard science. Why did the West become fat in the first place; what is driving this change, and are these drugs just a commercial solution to a commercially-made problem, and if so, is that just perpetuating the root cause?
Bottom line: ultimately, this text is both strongly for, and strongly against, GLP-1 receptor agonists. If you’ve been looking for a balanced book on the topic, this is it. And, as users of the new drugs grow in number, some have suggested that it will change humanity to an extent comparable with the invention of the smartphone. So, for or against or a bit of both, it’s good to at least understand them.
Click here to check out Magic Pill, and understand both sides!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: