Ticks Are Migrating, Raising Disease Risks if They Can’t Be Tracked Quickly Enough
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Biologist Grant Hokit came to this small meadow in the mountains outside Condon, Montana, to look for ticks. A hiking path crossed the expanse of long grasses and berry bushes.
As Hokit walked the path, he carried a handmade tool made of plastic pipes taped together to hold a large rectangle of white flannel cloth.
He poked fun at this “sophisticated” device, but the scientific survey was quite serious: He was sweeping the cloth over the shrubs and grass, hoping that “questing” ticks would latch on.
Along the summer trail, ticks dangle from blades of grass, sticking their legs out and waiting for a passing mammal.
“We got one,” Hokit said.
“So that came off of this sedge grass right here,” he said. “Simply pick them off with our fingers. We’ve got a vial that we pop them in.”
Any captured ticks would go back to Hokit’s lab in Helena for identification. Most of them would probably be identified as Rocky Mountain wood ticks.
But Hokit also wanted to find out whether new species are making their way into the state.
As human-driven climate change makes winters shorter, ticks are spending less time hibernating and have more active months when they can hitch rides on animals and people. Sometimes the ticks carry themselves — and diseases — to new parts of the country.
Hokit found deer ticks for the first time in northeastern Montana earlier this year. Deer ticks are infamous for transmitting Lyme disease and can infect people with other pathogens.
Knowing a new species like the deer tick has arrived in Montana or other states is important for doctors.
Neil Ku is an infectious disease specialist at the Billings Clinic in eastern Montana. He said most patients don’t come in right after they get bitten by a tick. They usually show up later, when they start feeling sick from a tick-borne illness.
“Fever, some chills, they may just feel bad, similar to many infections we may encounter throughout the year,” he said.
It’s rare that patients connect a tick bite to those symptoms, and even more rare that they capture and keep the tick that bit them. Sorting out whether someone might have a tick-borne illness can be complicated.
Knowing what kinds of ticks are in the region will help doctors know that they might start encountering patients infected with new diseases after a tick bite, Ku said.
That’s partially why the state is on the hunt for new tick species.
“The more we know about what’s in Montana, the better we can inform our physicians, the better care you can receive,” said Devon Cozart, a zoonotic illness and vector-borne disease epidemiologist with the Montana Department of Public Health and Human Services.
Cozart collects and tests the ticks from field surveys in Montana to see whether they are carrying any pathogens.
Whether a tick can get a human sick depends on the species, but the kind of mammal it feeds on also plays a role.
“Usually it’s a rodent that might be carrying, for example, Rocky Mountain spotted fever,” she said. “So, the tick will feed on that rodent, then will get the pathogen as well.”
Because the prevalence of a particular disease can vary in mammal populations, ticks in one part of the state could be more or less likely to get you sick. That’s also important information for medical providers, Cozart said.
This kind of surveillance and testing isn’t happening in every county or state. A 2023 survey of nearly 500 health departments throughout the country found that roughly a quarter do some kind of tick surveillance.
Not all surveillance efforts are equal, said Chelsea Gridley-Smith, director of environmental health at the National Association of City and County Health Officials.
Field surveys can be expensive. For numerous local and state health departments, tick surveillance relies on a less expensive, more passive approach: Concerned patients, veterinarians, and doctors must collect and send in ticks for identification.
“It does provide a little information about what ticks are actually interacting with people and animals, but it doesn’t get into the weeds of how common ticks are in that area and how often do those ticks carry pathogens,” Gridley-Smith said.
She said more health departments want to start tick surveillance, but getting funding is hard — and might get harder as federal public health grants from agencies like the Centers for Disease Control and Prevention dry up.
Montana receives about $60,000 from a federal grant annually, but the bulk of that funding goes toward mosquito surveillance, which is more intensive and costly. What’s left funds trips into the field to look for ticks.
Hokit said he doesn’t have enough funding for his small team to survey everywhere he would like to in a state as large as Montana. That means he’s unable to monitor emerging populations of deer ticks as closely as he would like.
He found those new deer ticks in two Montana counties, but he doesn’t have enough data to determine whether they have begun reproducing there, establishing a local population.
In the meantime, Hokit uses data on climate and vegetation to make predictions about where deer ticks might thrive in the state. He has his eye on particular areas of western Montana, like the Flathead Valley.
He said that will help him and his team narrow down where to look next so they can let the public know when deer ticks — and the diseases they can carry — arrive.
This article is part of a partnership with NPR and Montana Public Radio
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Pineapple vs Watermelon – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pineapple to watermelon, we picked the pineapple.
Why?
Both have their merits, but there’s a clear winner here:
In terms of macros, pineapple has more than 3x the fiber and just under 2x the carbs, making it the best in this category.
In the category of vitamins, pineapple has more of vitamins B1, B2, B3, B6, B9, C, K, and choline, while watermelon has more of vitamins A and E; a clear win for pineapple here, by the numbers.
When it comes to minerals, pineapple has more calcium, copper, iron, magnesium, manganese, and zinc, while watermelon has more phosphorus and potassium. Another win for pineapple.
Looking at other considerations, it’s worth noting that pineapple has bromelain (a highly beneficial enzyme group that’s unique to pineapple), and watermelon is an excellent source of lycopene (better even than tomatoes, which are famous for their lycopene content). So, a tie in this round.
Adding up the sections makes for an easy overall win for pineapple, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Enjoy!
Share This Post
-
Asparagus vs Carrots – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing asparagus to carrots, we picked the asparagus.
Why?
In terms of macros, they’re fairly comparable: asparagus has more protein (but the numbers are small), while carrots have very slightly more fiber, and somewhat more carbs, but again, it’s not much. The glycemic indices also being comparable, we’re calling this round a tie, but feel free to swing it one way or the other if you have strong subjective feelings about those small macro differences.
When it comes to vitamins, asparagus has more of vitamins B1, B2, B7, B9, E, K, and choline, while carrots have more of vitamins A and B6. While carrots are admittedly one of the best sources of vitamin A in existence, there is only so far that can take a vegetable, and we say asparagus wins on strength of numbers (and by large margins on each of those vitamins, too).
In the category of minerals, asparagus has more copper, iron, magnesium, manganese, phosphorus, selenium, and zinc, while carrots have more calcium and potassium. Another win for asparagus.
Looking at polyphenols, asparagus has a greater total mass of polyphenols (mostly quercetin), while carrots have more diversity, but mostly tiny numbers. We’d call this a win for asparagus, but an argument could be made for a tie in this category.
Adding up the sections makes for an overall win for asparagus, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
Fight Inflammation & Protect Your Brain, With Quercetin
Enjoy!
Share This Post
-

Could Just Two Hours Sleep Per Day Be Enough?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Polyphasic Sleep… Super-Schedule Or An Idea Best Put To Rest?
What is it?
Let’s start by defining some terms:
- Monophasic sleep—sleeping in one “chunk” per day. For example, a good night’s “normal” sleep.
- Biphasic sleep—sleeping in two “chunks” per day. Typically, a shorter night’s sleep, with a nap usually around the middle of the day / early afternoon.
- Polyphasic sleep—sleeping in two or more “chunks per day”. Some people do this in order to have more hours awake per day, to do things. The idea is that sleeping this way is more efficient, and one can get enough rest in less time. The most popular schedules used are:
- The Überman schedule—six evenly-spaced 20-minute naps, one every four hours, throughout the 24-hour day. The name is a semi-anglicized version of the German word Übermensch, “Superman”.
- The Everyman schedule—a less extreme schedule, that has a three-hours “long sleep” during the night, and three evenly-spaced 20-minute naps during the day, for a total of 4 hours sleep.
There are other schedules, but we’ll focus on the most popular ones here.
Want to learn about the others? Visit: Polyphasic.Net (a website by and for polyphasic sleep enthusiasts)
Some people have pointed to evidence that suggests humans are naturally polyphasic sleepers, and that it is only modern lifestyles that have forced us to be (mostly) monophasic.
There is at least some evidence to suggest that when environmental light/dark conditions are changed (because of extreme seasonal variation at the poles, or, as in this case, because of artificial changes as part of a sleep science experiment), we adjust our sleeping patterns accordingly.
The counterpoint, of course, is that perhaps when at the mercy of long days/nights at the poles, or no air-conditioning to deal with the heat of the day in the tropics, that perhaps we were forced to be polyphasic, and now, with modern technology and greater control, we are free to be monophasic.
Either way, there are plenty of people who take up the practice of polyphasic sleep.
Ok, But… Why?
The main motivation for trying polyphasic sleep is simply to have more hours in the day! It’s exciting, the prospect of having 22 hours per day to be so productive and still have time over for leisure.
A secondary motivation for trying polyphasic sleep is that when the brain is sleep-deprived, it will prioritize REM sleep. Here’s where the Überman schedule becomes perhaps most interesting:
The six evenly-spaced naps of the Überman schedule are each 20 minutes long. This corresponds to the approximate length of a normal REM cycle.
Consequently, when your head hits the pillow, you’ll immediately begin dreaming, and at the end of your dream, the alarm will go off.
Waking up at the end of a dream, when one hasn’t yet entered a non-REM phase of sleep, will make you more likely to remember it. Similarly, going straight into REM sleep will make you more likely to be aware of it, thus, lucid dreaming.
Read: Sleep fragmentation and lucid dreaming (actually a very interesting and informative lucid dreaming study even if you don’t want to take up polyphasic sleep)
Six 20-minute lucid-dreaming sessions per day?! While awake for the other 22 hours?! That’s… 24 hours per day of wakefulness to use as you please! What sorcery is this?
Hence, it has quite an understandable appeal.
Next Question: Does it work?
Can we get by without the other (non-REM) kinds of sleep?
According to Überman cycle enthusiasts: Yes! The body and brain will adapt.
According to sleep scientists: No! The non-REM slow-wave phases of sleep are essential
Read: Adverse impact of polyphasic sleep patterns in humans—Report of the National Sleep Foundation sleep timing and variability consensus panel
(if you want to know just how bad it is… the top-listed “similar article” is entitled “Suicidal Ideation”)
But what about, for example, the Everman schedule? Three hours at night is enough for some non-REM sleep, right?
It is, and so it’s not as quickly deleterious to the health as the Überman schedule. But, unless you are blessed with rare genes that allow you to operate comfortably on 4 hours per day (you’ll know already if that describes you, without having to run any experiment), it’s still bad.
Adults typically need 7–9 hours of sleep per night, and if you don’t get it, you’ll accumulate a sleep debt. And, importantly:
When you accumulate sleep debt, you are borrowing time at a very high rate of interest!
And, at risk of laboring the metaphor, but this is important too:
Not only will you have to pay it back soon (with interest), you will be hounded by the debt collection agents—decreased cognitive ability and decreased physical ability—until you pay up.
In summary:
- Polyphasic sleep is really very tempting
- It will give you more hours per day (for a while)
- It will give the promised lucid dreaming benefits (which is great until you start micronapping between naps, this is effectively a mini psychotic break from reality lasting split seconds each—can be deadly if behind the wheel of a car, for instance!)
- It is unequivocally bad for the health and we do not recommend it
Bottom line:
Some of the claimed benefits are real, but are incredibly short-term, unsustainable, and come at a cost that’s far too high. We get why it’s tempting, but ultimately, it’s self-sabotage.
(Sadly! We really wanted it to work, too…)
Share This Post


-
I’m feeling run down. Why am I more likely to get sick? And how can I boost my immune system?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It has been a long winter, filled with many viruses and cost-of-living pressures, on top of the usual mix of work, study, life admin and caring responsibilities.
Stress is an inevitable part of life. In short bursts, our stress response has evolved as a survival mechanism to help us be more alert in fight or flight situations.
But when stress is chronic, it weakens the immune system and makes us more vulnerable to illnesses such as the common cold, flu and COVID.

Pexels/Ketut Subiyanto Stress makes it harder to fight off viruses
When the immune system starts to break down, a virus that would normally have been under control starts to flourish.
Once you begin to feel sick, the stress response rises, making it harder for the immune system to fight off the disease. You may be sick more often and for longer periods of time, without enough immune cells primed and ready to fight.
In the 1990s, American psychology professor Sheldon Cohen and his colleagues conducted a number of studies where healthy people were exposed to an upper respiratory infection, through drops of virus placed directly into their nose.
These participants were then quarantined in a hotel and monitored closely to determine who became ill.
One of the most important factors predicting who got sick was prolonged psychological stress.
Cortisol suppresses immunity
“Short-term stress” is stress that lasts for a period of minutes to hours, while “chronic stress” persists for several hours per day for weeks or months.
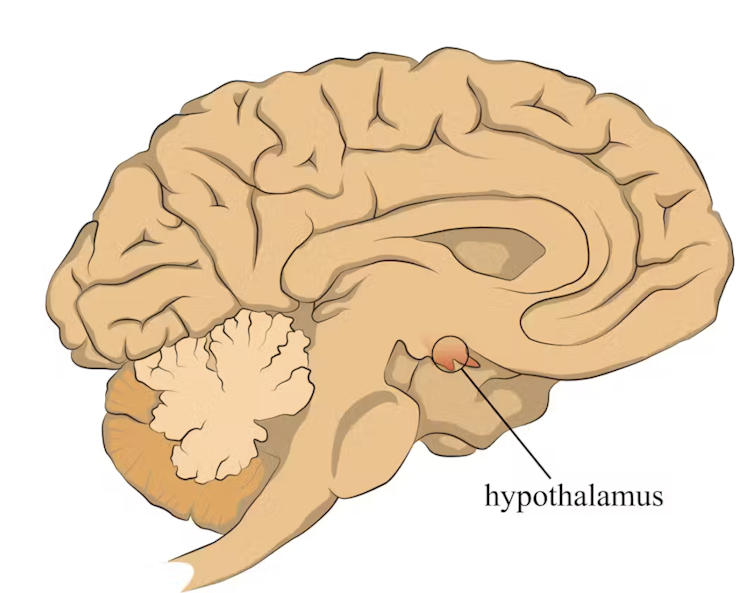
When faced with a perceived threat, psychological or physical, the hypothalamus region of the brain sets off an alarm system. This signals the release of a surge of hormones, including adrenaline and cortisol.
The hypothalamus sets off an alarm system in response to a real or perceived threat. stefan3andrei/Shutterstock In a typical stress response, cortisol levels quickly increase when stress occurs, and then rapidly drop back to normal once the stress has subsided. In the short term, cortisol suppresses inflammation, to ensure the body has enough energy available to respond to an immediate threat.
But in the longer term, chronic stress can be harmful. A Harvard University study from 2022 showed that people suffering from psychological distress in the lead up to their COVID infection had a greater chance of experiencing long COVID. They classified this distress as depression, probable anxiety, perceived stress, worry about COVID and loneliness.
Those suffering distress had close to a 50% greater risk of long COVID compared to other participants. Cortisol has been shown to be high in the most severe cases of COVID.
Stress causes inflammation
Inflammation is a short-term reaction to an injury or infection. It is responsible for trafficking immune cells in your body so the right cells are present in the right locations at the right times and at the right levels.
The immune cells also store a memory of that threat to respond faster and more effectively the next time.
Initially, circulating immune cells detect and flock to the site of infection. Messenger proteins, known as pro-inflammatory cytokines, are released by immune cells, to signal the danger and recruit help, and our immune system responds to neutralise the threat.
During this response to the infection, if the immune system produces too much of these inflammatory chemicals, it can trigger symptoms such as nasal congestion and runny nose.
Our immune response can trigger symptoms such as a runny nose. Alyona Mandrik/Shutterstock What about chronic stress?
Chronic stress causes persistently high cortisol secretion, which remains high even in the absence of an immediate stressor.
The immune system becomes desensitised and unresponsive to this cortisol suppression, increasing low-grade “silent” inflammation and the production of pro-inflammatory cytokines (the messenger proteins).
Immune cells become exhausted and start to malfunction. The body loses the ability to turn down the inflammatory response.
Over time, the immune system changes the way it responds by reprogramming to a “low surveillance mode”. The immune system misses early opportunities to destroy threats, and the process of recovery can take longer.
So how can you manage your stress?
We can actively strengthen our immunity and natural defences by managing our stress levels. Rather than letting stress build up, try to address it early and frequently by:
1) Getting enough sleep
Getting enough sleep reduces cortisol levels and inflammation. During sleep, the immune system releases cytokines, which help fight infections and inflammation.
2) Taking regular exercise
Exercising helps the lymphatic system (which balances bodily fluids as part of the immune system) circulate and allows immune cells to monitor for threats, while sweating flushes toxins. Physical activity also lowers stress hormone levels through the release of positive brain signals.
3) Eating a healthy diet
Ensuring your diet contains enough nutrients – such as the B vitamins, and the full breadth of minerals like magnesium, iron and zinc – during times of stress has a positive impact on overall stress levels. Staying hydrated helps the body to flush out toxins.
4) Socialising and practising meditation or mindfulness
These activities increase endorphins and serotonin, which improve mood and have anti-inflammatory effects. Breathing exercises and meditation stimulate the parasympathetic nervous system, which calms down our stress responses so we can “reset” and reduce cortisol levels.
Sathana Dushyanthen, Academic Specialist & Lecturer in Cancer Sciences & Digital Health| Superstar of STEM| Science Communicator, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Horse Sedative Use Among Humans Spreads in Deadly Mixture of ‘Tranq’ and Fentanyl
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
TREASURE ISLAND, Fla. — Andrew McClave Jr. loved to lift weights. The 6-foot-4-inch bartender resembled a bodybuilder and once posed for a photo flexing his muscles with former pro wrestler Hulk Hogan.
“He was extremely dedicated to it,” said his father, Andrew McClave Sr., “to the point where it was almost like he missed his medication if he didn’t go.”
But the hobby took its toll. According to a police report, a friend told the Treasure Island Police Department that McClave, 36, suffered from back problems and took unprescribed pills to reduce the pain.
In late 2022, the friend discovered McClave in bed. He had no pulse. A medical examiner determined he had a fatal amount of fentanyl, cocaine, and xylazine, a veterinary tranquilizer used to sedate horses, in his system, an autopsy report said. Heart disease was listed as a contributing factor.
McClave is among more than 260 people across Florida who died in one year from accidental overdoses involving xylazine, according to a Tampa Bay Times analysis of medical examiner data from 2022, the first year state officials began tracking the substance. Numbers for 2023 haven’t been published.
The death toll reflects xylazine’s spread into the nation’s illicit drug supply. Federal regulators approved the tranquilizer for animals in the early 1970s and it’s used to sedate horses for procedures like oral exams and colic treatment, said Todd Holbrook, an equine medicine specialist at the University of Florida. Reports of people using xylazine emerged in Philadelphia, then the drug spread south and west.
What’s not clear is exactly what role the sedative plays in overdose deaths, because the Florida data shows no one fatally overdosed on xylazine alone. The painkiller fentanyl was partly to blame in all but two cases in which the veterinary drug was included as a cause of death, according to the Times analysis. Cocaine or alcohol played roles in the cases in which fentanyl was not involved.
Fentanyl is generally the “800-pound gorilla,” according to Lewis Nelson, chair of the emergency medicine department at Rutgers New Jersey Medical School, and xylazine may increase the risk of overdose, though not substantially.
But xylazine appears to complicate the response to opioid overdoses when they do happen and makes it harder to save people. Xylazine can slow breathing to dangerous levels, according to federal health officials, and it doesn’t respond to the overdose reversal drug naloxone, often known by the brand name Narcan. Part of the problem is that many people may not know they are taking the horse tranquilizer when they use other drugs, so they aren’t aware of the additional risks.
Lawmakers in Tallahassee made xylazine a Schedule 1 drug like heroin or ecstasy in 2016, and several other states including Pennsylvania, Ohio, and West Virginia have taken action to classify it as a scheduled substance, too. But it’s not prohibited at the federal level. Legislation pending in Congress would criminalize illicit xylazine use nationwide.
The White House in April designated the combination of fentanyl and xylazine, often called “tranq dope,” as an emerging drug threat. A study of 20 states and Washington, D.C., found that overdose deaths attributed to both illicit fentanyl and xylazine exploded from January 2019 to June 2022, jumping from 12 a month to 188.
“We really need to continue to be proactive,” said Amanda Bonham-Lovett, program director of a syringe exchange in St. Petersburg, “and not wait until this is a bigger issue.”
‘A Good Business Model’
There are few definitive answers about why xylazine use has spread — and its impact on people who consume it.
The U.S. Drug Enforcement Administration in September said the tranquilizer is entering the country in several ways, including from China and in fentanyl brought across the southwestern border. The Florida attorney general’s office is prosecuting an Orange County drug trafficking case that involves xylazine from a New Jersey supplier.
Bonham-Lovett, who runs IDEA Exchange Pinellas, the county’s anonymous needle exchange, said some local residents who use drugs are not seeking out xylazine — and don’t know they’re consuming it.
One theory is that dealers are mixing xylazine into fentanyl because it’s cheap and also affects the brain, Nelson said.
“It’s conceivable that if you add a psychoactive agent to the fentanyl, you can put less fentanyl in and still get the same kick,” he said. “It’s a good business model.”
In Florida, men accounted for three-quarters of fatal overdoses involving xylazine, according to the Times analysis. Almost 80% of those who died were white. The median age was 42.
Counties on Florida’s eastern coast saw the highest death tolls. Duval County topped the list with 46 overdoses. Tampa Bay recorded 19 fatalities.
Cocaine was also a cause in more than 80 cases, including McClave’s, the Times found. The DEA in 2018 warned of cocaine laced with fentanyl in Florida.
In McClave’s case, Treasure Island police found what appeared to be marijuana and a small plastic bag with white residue in his room, according to a police report. His family still questions how he took the powerful drugs and is grappling with his death.
He was an avid fisherman, catching snook and grouper in the Gulf of Mexico, said his sister, Ashley McClave. He dreamed of being a charter boat captain.
“I feel like I’ve lost everything,” his sister said. “My son won’t be able to learn how to fish from his uncle.”
Mysterious Wounds
Another vexing challenge for health officials is the link between chronic xylazine use and open wounds.
The wounds are showing up across Tampa Bay, needle exchange leaders said. The telltale sign is blackened, crusty tissue, Bonham-Lovett said. Though the injuries may start small — the size of a dime — they can grow and “take over someone’s whole limb,” she said.
Even those who snort fentanyl, instead of injecting it, can develop them. The phenomenon is unexplained, Nelson said, and is not seen in animals.
IDEA Exchange Pinellas has recorded at least 10 cases since opening last February, Bonham-Lovett said, and has a successful treatment plan. Staffers wash the wounds with soap and water, then dress them.
One person required hospitalization partly due to xylazine’s effects, Bonham-Lovett said. A 31-year-old St. Petersburg woman, who asked not to be named due to concerns over her safety and the stigma of drug use, said she was admitted to St. Anthony’s Hospital in 2023. The woman, who said she uses fentanyl daily, had a years-long staph infection resistant to some antibiotics, and a wound recently spread across half her thigh.
The woman hadn’t heard of xylazine until IDEA Exchange Pinellas told her about the drug. She’s thankful she found out in time to get care.
“I probably would have lost my leg,” she said.
This article was produced in partnership with the Tampa Bay Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Long-acting contraceptives seem to be as safe as the pill when it comes to cancer risk
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many women worry hormonal contraceptives have dangerous side-effects including increased cancer risk. But this perception is often out of proportion with the actual risks.
So, what does the research actually say about cancer risk for contraceptive users?
And is your cancer risk different if, instead of the pill, you use long-acting reversible contraceptives? These include intrauterine devices or IUDs (such as Mirena), implants under the skin (such as Implanon), and injections (such as Depo Provera).
Our new study, conducted by the University of Queensland and QIMR Berghofer Medical Research Institute and published by the Journal of the National Cancer Institute, looked at this question.
We found long-acting contraceptives seem to be as safe as the pill when it comes to cancer risk (which is good news) but not necessarily any safer than the pill.
Peakstock/Shutterstock Some hormonal contraceptives take the form of implants under the skin. WiP-Studio/Shutterstock How does the contraceptive pill affect cancer risk?
The International Agency for Research on Cancer, which compiles evidence on cancer causes, has concluded that oral contraceptives have mixed effects on cancer risk.
Using the oral contraceptive pill:
- slightly increases your risk of breast and cervical cancer in the short term, but
- substantially reduces your risk of cancers of the uterus and ovaries in the longer term.
Our earlier work showed the pill was responsible for preventing far more cancers overall than it contributed to.
In previous research we estimated that in 2010, oral contraceptive pill use prevented over 1,300 cases of endometrial and ovarian cancers in Australian women.
It also prevented almost 500 deaths from these cancers in 2013. This is a reduction of around 25% in the deaths that could have occurred that year if women hadn’t taken the pill.
In contrast, we calculated the pill may have contributed to around 15 deaths from breast cancer in 2013, which is less than 0.5% of all breast cancer deaths in that year.
Previous work showed the pill was responsible for preventing far more cancers overall than it contributed to. Image Point Fr What about long-acting reversible contraceptives and cancer risk?
Long-acting reversible contraceptives – which include intrauterine devices or IUDs, implants under the skin, and injections – release progesterone-like hormones.
These are very effective contraceptives that can last from a few months (injections) up to seven years (intrauterine devices).
Notably, they don’t contain the hormone oestrogen, which may be responsible for some of the side-effects of the pill (including perhaps contributing to a higher risk of breast cancer).
Use of these long-acting contraceptives has doubled over the past decade, while the use of the pill has declined. So it’s important to know whether this change could affect cancer risk for Australian women.
Our new study of more than 1 million Australian women investigated whether long-acting, reversible contraceptives affect risk of invasive cancers. We compared the results to the oral contraceptive pill.
We used de-identified health records for Australian women aged 55 and under in 2002.
Among this group, about 176,000 were diagnosed with cancer between 2004 and 2013 when the oldest women were aged 67. We compared hormonal contraceptive use among these women who got cancer to women without cancer.
We found that long-term users of all types of hormonal contraception had around a 70% lower risk of developing endometrial cancer in the years after use. In other words, the risk of developing endometrial cancer is substantially lower among women who took hormonal contraception compared to those who didn’t.
For ovarian cancer, we saw a 50% reduced risk (compared to those who took no hormonal contraception) for women who were long-term users of the hormone-containing IUD.
The risk reduction was not as marked for the implants or injections, however few long-term users of these products developed these cancers in our study.
As the risk of endometrial and ovarian cancers increases with age, it will be important to look at cancer risk in these women as they get older.
What about breast cancer risk?
Our findings suggest that the risk of breast cancer for current users of long-acting contraceptives is similar to users of the pill.
However, the contraceptive injection was only associated with an increase in breast cancer risk after five years of use and there was no longer a higher risk once women stopped using them.
Our results suggested that the risk of breast cancer also reduces after stopping use of the contraceptive implants.
We will need to follow-up the women for longer to determine whether this is also the case for the IUD.
It is worth emphasising that the breast cancer risk associated with all hormonal contraceptives is very small.
About 30 in every 100,000 women aged 20 to 39 years develop breast cancer each year, and any hormonal contraceptive use would only increase this to around 36 cases per 100,000.
What about other cancers?
Our study did not show any consistent relationships between contraceptive use and other cancers types. However, we only at looked at invasive cancers (meaning those that start at a primary site but have the potential to spread to other parts of the body).
A recent French study found that prolonged use of the contraceptive injection increased the risk of meningioma (a type of benign brain tumour).
However, meningiomas are rare, especially in young women. There are around two cases in every 100,000 in women aged 20–39, so the extra number of cases linked to contraceptive injection use was small.
The French study found the hormonal IUD did not increase meningioma risk (and they did not investigate contraceptive implants).
Benefits and side-effects
There are benefits and side-effects for all medicines, including contraceptives, but it is important to know most very serious side-effects are rare.
A conversation with your doctor about the balance of benefits and side-effects for you is always a good place to start.
Susan Jordan, Professor of Epidemiology, The University of Queensland; Karen Tuesley, Postdoctoral Research Fellow, School of Public Health, The University of Queensland, and Penny Webb, Distinguished Scientist, Gynaecological Cancers Group, QIMR Berghofer Medical Research Institute
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: