Why You Feel Like You Have To Pee Again Right After You Just Went
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Amy Konvalin talks us through breaking the pattern:
When nature calls… Repeatedly
Fun fact: feeling like you need to pee again right after standing up is often more a matter of bladder sensation, pelvic floor tension, positioning, and learned bathroom habits, rather than necessarily incomplete emptying.
Notably, repeatedly sitting back down “just in case” can accidentally train your brain and bladder into expecting a second round, reinforcing the pattern over time.
So, what to do instead?
- Before: sit down, take three slow deep belly breaths in through your nose, then exhale fully, to help relax your nervous system and pelvic floor before starting.
- During: consciously relax your pelvic floor instead of rushing or straining.
- After: once you feel done, take one more deep breath, exhale, and check once, dry and stand up, resisting any urge to return.
- After after: distract yourself and move on with your day to help break the automatic “go twice” pattern.
Safety note, though: persistent urinary urgency, frequent urination, pain, burning, blood in your urine, prolapse symptoms, recurrent infections, or trouble emptying should all be checked out by an medical professional, as many causes—including UTIs, overactive bladder, pelvic floor dysfunction, or prostate/bladder issues and even cancer—can overlap.
For more on all of this and for some mysterious reason absolutely no visual demonstrations for this one, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Stop Pain Spreading

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Put Your Back Into It (Or Don’t)!
We’ve written before about Managing Chronic Pain (Realistically!), and today we’re going to tackle a particular aspect of chronic pain management.
- It’s a thing where the advice is going to be “don’t do this”
- And if you have chronic pain, you will probably respond “yep, I do that”
However, it’s definitely a case of “when knowing isn’t the problem”, or at the very least, it’s not the whole problem.
Stop overcompensating and address the thing directly
We all do it, whether in chronic pain, or just a transient injury. But we all need to do less of it, because it causes a lot of harm.
Example: you have pain in your right knee, so you sit, stand, walk slightly differently to try to ease that pain. It works, albeit marginally, at least for a while, but now you also have pain in your left hip and your lumbar vertebrae, because of how you leaned a certain way. You adjust how you sit, stand, walk, to try to ease both sets of pain, and before you know it, now your neck also hurts, you have a headache, and you’re sure your digestion isn’t doing what it should and you feel dizzy when you stand. The process continues, and before long, what started off as a pain in one knee has now turned your whole body into a twisted aching wreck.
What has happened: the overcompensation due to the original pain has unduly stressed a connected part of the body, which we then overcompensate for somewhere else, bringing down the whole body like a set of dominoes.
For more on this: Understanding How Pain Can Spread
“Ok, but how? I can’t walk normally on that knee!”
We’re keeping the knee as an example here, but please bear in mind it could be any chronic pain and resultant disability.
Note: if you found the word “disability” offputting, please remember: if it adversely affects your abilities, it is a disability. Disabilities are not something that only happen to other people! They will happen to most of us at some point!
Ask yourself: what can you do, and what can’t you do?
For example:
- maybe you can walk, but not normally
- maybe you can walk normally, but not without great pain
- maybe you can walk normally, but not at your usual walking pace
First challenge: accept your limitations. If you can’t walk at your usual walking pace without great pain and/or throwing your posture to the dogs, then walk more slowly. To Hell with societal expectations that it shouldn’t take so long to walk from A to B. Take the time you need.
Second challenge: accept help. It doesn’t have to be help from another person (although it could be). It might be accepting the help of a cane, or maybe even a wheelchair for “flare-up” days. Society, especially American society which is built on ideas of self-sufficiency, has framed a lot of such options as “giving up”, but if they help you get about your day while minimizing doing further harm to your body, then they can be good and even health-preserving things. Same goes for painkillers if they help you from doing more harm to your body by balling up tension in a part of your body in a way that ends up spreading out and laying ruin to your whole body.
Speaking of which:
How Much Does It Hurt? Get The Right Help For Your Pain
After which, you might want to check out:
The 7 Approaches To Pain Management
and
Science-Based Alternative Pain Relief
Third challenge: deserves its own section, so…
Do what you can
If you have chronic pain (or any chronic illness, really), you are probably fed up of hearing how this latest diet will fix you, or yoga will fix you, and so on. But, while these things may not be miracle cures…
- A generally better diet really will lessen symptoms and avoid flare-ups (a low-inflammation diet is a great start for lessening the symptoms of a lot of chronic illnesses)
- Doing what exercise you can, being mindful of your limitations yes but still keeping moving as much as possible, will also prevent (or at least slow) deterioration. Consider consulting a physiotherapist for guidance (a doctor will more likely just say “rest, take it easy”, whereas a physiotherapist will be able to give more practical advice).
- Getting good sleep may be a nightmare in the case of chronic pain (or other chronic illnesses! Here’s to those late night hyperglycemia incidents for Type 1 Diabetics that then need monitoring for the next few hours while taking insulin and hoping it goes back down) but whatever you can do to prioritize it, do it.
Want to read more?
We reviewed a little while ago a great book about this; the title sounds like a lot of woo, but we promise the content is extremely well-referenced science:
…and if your issue is back pain specifically, we highly recommend:
Healing Back Pain: The Mind-Body Connection – by Dr. John Sarno
Take care!
Share This Post
-

4 Ways Vaccine Skeptics Mislead You on Measles and More
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Measles is on the rise in the United States. In the first quarter of this year, the number of cases was about 17 times what it was, on average, during the same period in each of the four years before, according to the Centers for Disease Control and Prevention. Half of the people infected — mainly children — have been hospitalized.
It’s going to get worse, largely because a growing number of parents are deciding not to get their children vaccinated against measles as well as diseases like polio and pertussis. Unvaccinated people, or those whose immunization status is unknown, account for 80% of the measles cases this year. Many parents have been influenced by a flood of misinformation spouted by politicians, podcast hosts, and influential figures on television and social media. These personalities repeat decades-old notions that erode confidence in the established science backing routine childhood vaccines. KFF Health News examined the rhetoric and explains why it’s misguided:
The No-Big-Deal Trope
A common distortion is that vaccines aren’t necessary because the diseases they prevent are not very dangerous, or too rare to be of concern. Cynics accuse public health officials and the media of fear-mongering about measles even as 19 states report cases.
For example, an article posted on the website of the National Vaccine Information Center — a regular source of vaccine misinformation — argued that a resurgence in concern about the disease “is ‘sky is falling’ hype.” It went on to call measles, mumps, chicken pox, and influenza “politically incorrect to get.”
Measles kills roughly 2 of every 1,000 children infected, according to the CDC. If that seems like a bearable risk, it’s worth pointing out that a far larger portion of children with measles will require hospitalization for pneumonia and other serious complications. For every 10 measles cases, one child with the disease develops an ear infection that can lead to permanent hearing loss. Another strange effect is that the measles virus can destroy a person’s existing immunity, meaning they’ll have a harder time recovering from influenza and other common ailments.
Measles vaccines have averted the deaths of about 94 million people, mainly children, over the past 50 years, according to an April analysis led by the World Health Organization. Together with immunizations against polio and other diseases, vaccines have saved an estimated 154 million lives globally.
Some skeptics argue that vaccine-preventable diseases are no longer a threat because they’ve become relatively rare in the U.S. (True — due to vaccination.) This reasoning led Florida’s surgeon general, Joseph Ladapo, to tell parents that they could send their unvaccinated children to school amid a measles outbreak in February. “You look at the headlines and you’d think the sky was falling,” Ladapo said on a News Nation newscast. “There’s a lot of immunity.”
As this lax attitude persuades parents to decline vaccination, the protective group immunity will drop, and outbreaks will grow larger and faster. A rapid measles outbreak hit an undervaccinated population in Samoa in 2019, killing 83 people within four months. A chronic lack of measles vaccination in the Democratic Republic of the Congo led to more than 5,600 people dying from the disease in massive outbreaks last year.
The ‘You Never Know’ Trope
Since the earliest days of vaccines, a contingent of the public has considered them bad because they’re unnatural, as compared with nature’s bounty of infections and plagues. “Bad” has been redefined over the decades. In the 1800s, vaccine skeptics claimed that smallpox vaccines caused people to sprout horns and behave like beasts. More recently, they blame vaccines for ailments ranging from attention-deficit/hyperactivity disorder to autism to immune system disruption. Studies don’t back the assertions. However, skeptics argue that their claims remain valid because vaccines haven’t been adequately tested.
In fact, vaccines are among the most studied medical interventions. Over the past century, massive studies and clinical trials have tested vaccines during their development and after their widespread use. More than 12,000 people took part in clinical trials of the most recent vaccine approved to prevent measles, mumps, and rubella. Such large numbers allow researchers to detect rare risks, which are a major concern because vaccines are given to millions of healthy people.
To assess long-term risks, researchers sift through reams of data for signals of harm. For example, a Danish group analyzed a database of more than 657,000 children and found that those who had been vaccinated against measles as babies were no more likely to later be diagnosed with autism than those who were not vaccinated. In another study, researchers analyzed records from 805,000 children born from 1990 through 2001 and found no evidence to back a concern that multiple vaccinations might impair children’s immune systems.
Nonetheless, people who push vaccine misinformation, like candidate Robert F. Kennedy Jr., dismiss massive, scientifically vetted studies. For example, Kennedy argues that clinical trials of new vaccines are unreliable because vaccinated kids aren’t compared with a placebo group that gets saline solution or another substance with no effect. Instead, many modern trials compare updated vaccines with older ones. That’s because it’s unethical to endanger children by giving them a sham vaccine when the protective effect of immunization is known. In a 1950s clinical trial of polio vaccines, 16 children in the placebo group died of polio and 34 were paralyzed, said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia and author of a book on the first polio vaccine.
The Too-Much-Too-Soon Trope
Several bestselling vaccine books on Amazon promote the risky idea that parents should skip or delay their children’s vaccines. “All vaccines on the CDC’s schedule may not be right for all children at all times,” writes Paul Thomas in his bestselling book “The Vaccine-Friendly Plan.” He backs up this conviction by saying that children who have followed “my protocol are among the healthiest in the world.”
Since the book was published, Thomas’ medical license was temporarily suspended in Oregon and Washington. The Oregon Medical Board documented how Thomas persuaded parents to skip vaccines recommended by the CDC, and reported that he “reduced to tears” a mother who disagreed. Several children in his care came down with pertussis and rotavirus, diseases easily prevented by vaccines, wrote the board. Thomas recommended fish oil supplements and homeopathy to an unvaccinated child with a deep scalp laceration, rather than an emergency tetanus vaccine. The boy developed severe tetanus, landing in the hospital for nearly two months, where he required intubation, a tracheotomy, and a feeding tube to survive.
The vaccination schedule recommended by the CDC has been tailored to protect children at their most vulnerable points in life and minimize side effects. The combination measles, mumps, and rubella vaccine isn’t given for the first year of a baby’s life because antibodies temporarily passed on from their mother can interfere with the immune response. And because some babies don’t generate a strong response to that first dose, the CDC recommends a second one around the time a child enters kindergarten because measles and other viruses spread rapidly in group settings.
Delaying MMR doses much longer may be unwise because data suggests that children vaccinated at 10 or older have a higher chance of adverse reactions, such as a seizure or fatigue.
Around a dozen other vaccines have discrete timelines, with overlapping windows for the best response. Studies have shown that MMR vaccines may be given safely and effectively in combination with other vaccines.
’They Don’t Want You to Know’ Trope
Kennedy compares the Florida surgeon general to Galileo in the introduction to Ladapo’s new book on transcending fear in public health. Just as the Roman Catholic inquisition punished the renowned astronomer for promoting theories about the universe, Kennedy suggests that scientific institutions oppress dissenting voices on vaccines for nefarious reasons.
“The persecution of scientists and doctors who dare to challenge contemporary orthodoxies is not a new phenomenon,” Kennedy writes. His running mate, lawyer Nicole Shanahan, has campaigned on the idea that conversations about vaccine harms are censored and the CDC and other federal agencies hide data due to corporate influence.
Claims like “they don’t want you to know” aren’t new among the anti-vaccine set, even though the movement has long had an outsize voice. The most listened-to podcast in the U.S., “The Joe Rogan Experience,” regularly features guests who cast doubt on scientific consensus. Last year on the show, Kennedy repeated the debunked claim that vaccines cause autism.
Far from ignoring that concern, epidemiologists have taken it seriously. They have conducted more than a dozen studies searching for a link between vaccines and autism, and repeatedly found none. “We have conclusively disproven the theory that vaccines are connected to autism,” said Gideon Meyerowitz-Katz, an epidemiologist at the University of Wollongong in Australia. “So, the public health establishment tends to shut those conversations down quickly.”
Federal agencies are transparent about seizures, arm pain, and other reactions that vaccines can cause. And the government has a program to compensate individuals whose injuries are scientifically determined to result from them. Around 1 to 3.5 out of every million doses of the measles, mumps, and rubella vaccine can cause a life-threatening allergic reaction; a person’s lifetime risk of death by lightning is estimated to be as much as four times as high.
“The most convincing thing I can say is that my daughter has all her vaccines and that every pediatrician and public health person I know has vaccinated their kids,” Meyerowitz-Katz said. “No one would do that if they thought there were serious risks.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Sleeping Positions & Your Heart & Brain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝Is it true that sleeping on your left side is bad for the heart?❞
Short answer: it can be!
It has to do with how much room the heart has to move around.
Now, mostly we tend to assume that our organs stay put, but the reality is, they have quite a bit of leeway to move around (one of the reasons why sitting is so bad for the health; see: Death by Sitting – by Carolyne Thompson and for how to fix that besides “sit less”, check out Stand Up For Your Health (Or Don’t) ← our main feature on this also includes more things you can do if you must sit, to make sitting less bad!).
When it comes to our heart, this is broadly situated fairly centrally and/but a little to the left, behind our sternum. This means that when we sleep lying on our right-hand side, the pull of gravity on our heart is towards the center, where there the internal structure (namely the mediastinum) supports it and keeps it in place.
When we sleep lying on our left-hand side, however, the heart can squish downwards (i.e. to our left) a bit, which can affect how it beats:
Lying position classification based on ECG waveform and random forest during sleep in healthy people
For most people, this shouldn’t be a huge issue, as our heart (much like the rest of our body) is quite resilient, and capable of looking after itself. However, if one has a predisposition to certain kinds of heart condition, it can become more of a problem, and for everyone, it’s at the very least not ideal.
On the other hand (literally), sleeping on the left-hand side can be better to avoid acid reflux if that’s a problem for you, due to the orientation of the opening at the the top of the stomach.
Body position affects recumbent postprandial reflux
Meanwhile, the brain is also a consideration when it comes to sleep positions and health. Because the glymphatic system (glial cells doing the clean-up job of the lymphatic system, but in the brain, where lymph cannot go) is strongly affected by gravity, the brain’s ability to remove toxins is dependent on the orientation of the head. This is critical for avoiding Alzheimer’s (beta-amyloid clearance) and Parkinson’s (alpha-synuclein clearance) amongst others, and for this:
- sleeping sideways is far better than sleeping on one’s back.
- sleeping on one’s right side is better than sleeping on one’s left side.
For more details on that, see:
Goodnight, Glymphatic System: How Your Sleep Position Changes Dementia Risk
Take care!
Share This Post

Related Posts
-

In This Oklahoma Town, Most Everyone Knows Someone Who’s Been Sued by the Hospital
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
McALESTER, Okla. — It took little more than an hour for Deborah Hackler to dispense with the tall stack of debt collection lawsuits that McAlester Regional Medical Center recently brought to small-claims court in this Oklahoma farm community.
Hackler, a lawyer who sues patients on behalf of the hospital, buzzed through 51 cases, all but a handful uncontested, as is often the case. She bantered with the judge as she secured nearly $40,000 in judgments, plus 10% in fees for herself, according to court records.
It’s a payday the hospital and Hackler have shared frequently over the past three decades, records show. The records indicate McAlester Regional Medical Center and an affiliated clinic have filed close to 5,000 debt collection cases since the early 1990s, most often represented by the father-daughter law firm of Hackler & Hackler.
Some of McAlester’s 18,000 residents have been taken to court multiple times. A deputy at the county jail and her adult son were each sued recently, court records show. New mothers said they compare stories of their legal run-ins with the medical center.
“There’s a lot that’s not right,” Sherry McKee, a dorm monitor at a tribal boarding school outside McAlester, said on the courthouse steps after the hearing. The hospital has sued her three times, most recently over a $3,375 bill for what she said turned out to be vertigo.
In recent years, major health systems in Virginia, North Carolina, and elsewhere have stopped suing patients following news reports about lawsuits. And several states, such as Maryland and New York, have restricted the legal actions hospitals can take against patients.
But with some 100 million people in the U.S. burdened by health care debt, medical collection cases still clog courtrooms across the country, researchers have found. In places like McAlester, a hospital’s debt collection machine can hum away quietly for years, helped along by powerful people in town. An effort to limit hospital lawsuits failed in the Oklahoma Legislature in 2021.
In McAlester, the lawsuits have provided business for some, such as the Adjustment Bureau, a local collection agency run out of a squat concrete building down the street from the courthouse, and for Hackler, a former president of the McAlester Area Chamber of Commerce. But for many patients and their families, the lawsuits can take a devastating toll, sapping wages, emptying retirement accounts, and upending lives.
McKee said she wasn’t sure how long it would take to pay off the recent judgment. Her $3,375 debt exceeds her monthly salary, she said.
“This affects a large number of people in a small community,” said Janet Roloff, an attorney who has spent years assisting low-income clients with legal issues such as evictions in and around McAlester. “The impact is great.”
Settled more than a century ago by fortune seekers who secured land from the Choctaw Nation to mine coal in the nearby hills, McAlester was once a boom town. Vestiges of that era remain, including a mammoth, 140-foot-tall Masonic temple that looms over the city.
Recent times have been tougher for McAlester, now home by one count to 12 marijuana dispensaries and the state’s death row. The downtown is pockmarked by empty storefronts, including the OKLA theater, which has been dark for decades. Nearly 1 in 5 residents in McAlester and the surrounding county live below the federal poverty line.
The hospital, operated by a public trust under the city’s authority, faces its own struggles. Paint is peeling off the front portico, and weeds poke up through the parking lots. The hospital has operated in the red for years, according to independent audit reports available on the state auditor’s website.
“I’m trying to find ways to get the entire community better care and more care,” said Shawn Howard, the hospital’s chief executive. Howard grew up in McAlester and proudly noted he started his career as a receptionist in the hospital’s physical therapy department. “This is my hometown,” he said. “I am not trying to keep people out of getting care.”
The hospital operates a clinic for low-income patients, whose webpage notes it has “limited appointments” at no cost for patients who are approved for aid. But data from the audits shows the hospital offers very little financial assistance, despite its purported mission to serve the community.
In the 2022 fiscal year, it provided just $114,000 in charity care, out of a total operating budget of more than $100 million, hospital records show. Charity care totaling $2 million or $3 million out of a $100 million budget would be more in line with other U.S. hospitals.
While audits show few McAlester patients get financial aid, many get taken to court.
Renee Montgomery, the city treasurer in an adjoining town and mother of a local police officer, said she dipped into savings she’d reserved for her children and grandchildren after the hospital sued her last year for more than $5,500. She’d gone to the emergency room for chest pain.
Dusty Powell, a truck driver, said he lost his pickup and motorcycle when his wages were garnished after the hospital sued him for almost $9,000. He’d gone to the emergency department for what turned out to be gastritis and didn’t have insurance, he said.
“Everyone in this town probably has a story about McAlester Regional,” said another former patient who spoke on the condition she not be named, fearful to publicly criticize the hospital in such a small city. “It’s not even a secret.”
The woman, who works at an Army munitions plant outside town, was sued twice over bills she incurred giving birth. Her sister-in-law has been sued as well.
“It’s a good-old-boy system,” said the woman, who lowered her voice when the mayor walked into the coffee shop where she was meeting with KFF Health News. Now, she said, she avoids the hospital if her children need care.
Nationwide, most people sued in debt collection cases never challenge them, a response experts say reflects widespread misunderstanding of the legal process and anxiety about coming to court.
At the center of the McAlester hospital’s collection efforts for decades has been Hackler & Hackler.
Donald Hackler was city attorney in McAlester for 13 years in the ’70s and ’80s and a longtime member of the local Lions Club and the Scottish Rite Freemasons.
Daughter Deborah Hackler, who joined the family firm 30 years ago, has been a deacon at the First Presbyterian Church of McAlester and served on the board of the local Girl Scouts chapter, according to the McAlester News-Capital newspaper, which named her “Woman of the Year” in 2007. Since 2001, she also has been a municipal judge in McAlester, hearing traffic cases, including some involving people she has sued on behalf of the hospital, municipal and county court records show.
For years, the Hacklers’ debt collection cases were often heard by Judge James Bland, who has retired from the bench and now sits on the hospital board. Bland didn’t respond to an inquiry for interview.
Hackler declined to speak with KFF Health News after her recent court appearance. “I’m not going to visit with you about a current client,” she said before leaving the courthouse.
Howard, the hospital CEO, said he couldn’t discuss the lawsuits either. He said he didn’t know the hospital took its patients to court. “I had to call and ask if we sue people,” he said.
Howard also said he didn’t know Deborah Hackler. “I never heard her name before,” he said.
Despite repeated public records requests from KFF Health News since September, the hospital did not provide detailed information about its financial arrangement with Hackler.
McAlester Mayor John Browne, who appoints the hospital’s board of trustees, said he, too, didn’t know about the lawsuits. “I hadn’t heard anything about them suing,” he said.
At the century-old courthouse in downtown McAlester, it’s not hard to find the lawsuits, though. Every month or two, another batch fills the docket in the small-claims court, now presided over by Judge Brian McLaughlin.
After court recently, McLaughlin, who is not from McAlester, shook his head at the stream of cases and patients who almost never show up to defend themselves, leaving him to issue judgment after judgment in the hospital’s favor.
“All I can do is follow the law,” said McLaughlin. “It doesn’t mean I like it.”
About This Project
“Diagnosis: Debt” is a reporting partnership between KFF Health News and NPR exploring the scale, impact, and causes of medical debt in America.
The series draws on original polling by KFF, court records, federal data on hospital finances, contracts obtained through public records requests, data on international health systems, and a yearlong investigation into the financial assistance and collection policies of more than 500 hospitals across the country.
Additional research was conducted by the Urban Institute, which analyzed credit bureau and other demographic data on poverty, race, and health status for KFF Health News to explore where medical debt is concentrated in the U.S. and what factors are associated with high debt levels.
The JPMorgan Chase Institute analyzed records from a sampling of Chase credit card holders to look at how customers’ balances may be affected by major medical expenses. And the CED Project, a Denver nonprofit, worked with KFF Health News on a survey of its clients to explore links between medical debt and housing instability.
KFF Health News journalists worked with KFF public opinion researchers to design and analyze the “KFF Health Care Debt Survey.” The survey was conducted Feb. 25 through March 20, 2022, online and via telephone, in English and Spanish, among a nationally representative sample of 2,375 U.S. adults, including 1,292 adults with current health care debt and 382 adults who had health care debt in the past five years. The margin of sampling error is plus or minus 3 percentage points for the full sample and 3 percentage points for those with current debt. For results based on subgroups, the margin of sampling error may be higher.
Reporters from KFF Health News and NPR also conducted hundreds of interviews with patients across the country; spoke with physicians, health industry leaders, consumer advocates, debt lawyers, and researchers; and reviewed scores of studies and surveys about medical debt.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Physio at 3 months old – or even earlier – can really help babies with cerebral palsy
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Physiotherapy isn’t just for adults recovering from injuries. Physiotherapists can help babies and children, too – including babies with, or at high risk of, cerebral palsy.
Research has shown physiotherapy improves their physical and cognitive outcomes.

freestocks.org/Pexels Cerebral palsy is complex
Cerebral palsy is a lifelong neurodevelopmental condition. It can affect the way you move and function.
It is caused by injury or a difference in development of the fetal or infant brain.
Each person with cerebral palsy experiences it in their own unique way.
This includes:
- the parts of their body affected
- how their body moves (for example, whether they have stiffness, involuntary movements or trouble with coordination)
- and how their motor impairments, or other issues, affect the way they move around, communicate and play.
The causes of cerebral palsy can be complex. It’s often due to a range of factors, including genetic and birth-related issues.
Early detection can mean early intervention
Until recently, many medical professionals adopted a “wait-and-see” approach.
However, we now have evidence-based tools to help identify babies most at risk of cerebral palsy – even those as young as three months.
After five months, if a baby shows movement difficulties (for example, using one side of their body more than the other or not being able to sit independently after nine months), an MRI and other tests can help your doctor understand more.
Early detection of cerebral palsy provides an opportunity for early intervention.
Some researchers talk about the seven “e-words” of physiotherapy intervention for babies with celebral palsy: earlier, engagement, exploration, enriched environments, experiences, everyday and exercise.
Even very young babies can be good candidates for physio. Photo by Kelly Sikkema on Unsplash Earlier intervention
Where intervention previously often started only around 19 months, now intervention can begin much earlier.
Some babies start physiotherapy as young as three months old once identified as being “high risk” for a diagnosis of cerebral palsy. Premature babies may begin physiotherapy while still in hospital.
Unfortunately, however, not all families have easy access to early intervention treatments. Much depends on where you live.
NDIS support is technically available but it can often take families months to be accepted for funding.
Engagement is key
Engagement refers to when babies deliberately participate in an activity or interact with others. This might be as simple as encouraging infants to look at and focus on a toy the baby finds interesting, or to move their body towards their caregiver’s face.
Research shows when infants are engaged in play, it helps make connections about how to move their body.
Physiotherapists can help parents learn how to engage with and play with their babies, even when babies are very young.
Exploration builds moving, playing and thinking skills
Exploration is how babies learn about and interact with the world.
Physiotherapists can help infants to explore movement, whether this is supporting them to reach for a toy or crawl down a hallway.
Babies and children with cerebral palsy can find it harder than their peers to explore their environments. Research has shown supporting infants and young children to explore their environment, including with mini power wheelchairs, can improve their long-term mobility, social skills and independence.
Enriched environments help challenge babies
Infants love to interact with spaces that are not too difficult to navigate, but also not too easy.
Physiotherapists and families can come up with ideas together about how to modify the environment in the home to help a baby with cerebral palsy successfully play and explore.
This could, for instance, include adjusting the height of toys on a baby play gym to challenge babies to successfully reach and grasp toys above them.
Experiences help babies learn to play, move and communicate
Every infant learns in their own way from doing, seeing, and feeling. These experiences shape the neural pathways in our brains throughout our life, but particularly in the first few years. Our brains’ ability to adapt to experiences is called neuroplasticity.
Physiotherapists can help families harness this neuroplasticity by identifying meaningful experiences that help their baby learn to move, play and explore.
Babies with cerebral palsy benefit from a combination of repeating motivating experiences (such as repeatedly rolling for a toy of interest) and practising new skills in a variety of environments (such as rolling on different surfaces or towards a variety of toys).
Everyday intervention
Physiotherapists work with families to find ways to support their infant’s development in everyday life. This will look different for every family.
Some prefer more structured ideas for activities; they might want to know how many times and how long they could help their baby sit using specific handling techniques.
Others prefer ideas on how to integrate therapy ideas into their everyday life by, for instance, picking their baby up via their side to help develop their head control.
Exercise – for all ages
Exercise helps with everything from heart and gastrointestinal health to bone health.
Infants with movement difficulties are at risk of more sedentary time. This increases the risk of cardiovascular disease and obesity. The Australian government recommends at least three hours of physical activity per day (including no more than one hour at a time of inactivity or restraint) for children aged between zero and five.
However, it can be really difficult for young children with cerebral palsy to meet these recommendations.
Physiotherapy can help. This might include:
- helping a baby play in physically challenging positions (such as tummy time) for longer periods each time
- supervised rough and tumble play with siblings
- encouraging babies to explore different and more challenging environments.
If you have concerns about your baby’s movement, talk to your GP or child health nurse.
Chelsea Mobbs, Lecturer in Physiotherapy, University of Southern Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Likely Are You To Live To 100?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How much hope can we reasonably have of reaching 100?
Yesterday, we asked you: assuming a good Health-Related Quality of Life (HRQoL), how much longer do you hope to live?

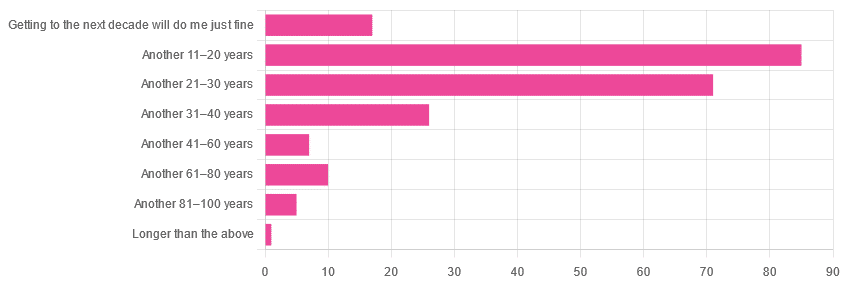
We got the above-depicted, below-described, set of responses:
- A little over 38% of respondents hope to live another 11–20 years
- A little over 31% hope to live another 31–40 years
- A little over 7% will be content to make it to the next decade
- One (1) respondent hopes to live longer than an additional 100 years
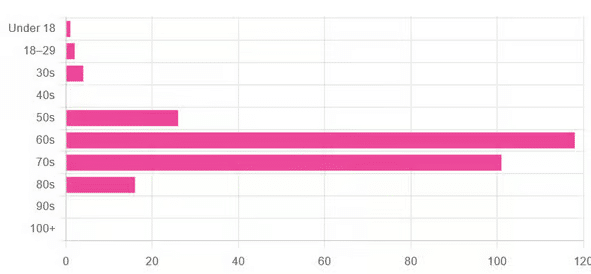
This is interesting when we put it against our graph of how old our subscribers are:

…because it corresponds inversely, right down to the gap/dent in the 40s. And—we may hypothesize—that one person under 18 who hopes to live to 120, perhaps.
This suggests that optimism remains more or less constant, with just a few wobbles that would probably be un-wobbled with a larger sample size.
In other words: most of our education-minded, health-conscious subscriber-base hope to make it to the age of 90-something, while for the most part feeling that 100+ is overly optimistic.
Writer’s anecdote: once upon a time, I was at a longevity conference in Brussels, and a speaker did a similar survey, but by show of hands. He started low by asking “put your hands up if you want to live at least a few more minutes”. I did so, with an urgency that made him laugh, and say “Don’t worry; I don’t have a gun hidden up here!”
Conjecture aside… What does the science say about our optimism?
First of all, a quick recap…
To not give you the same information twice, let’s note we did an “aging mythbusting” piece already covering:
- Aging is inevitable: True or False?
- Aging is, and always will be, unstoppable: True or False?
- We can slow aging: True or False?
- It’s too early to worry about… / It’s too late to do anything about… True or False?
- We can halt aging: True or False?
- We can reverse aging: True or False?
- But those aren’t really being younger, we’ll still die when our time is up: True or False?
You can read the answers to all of those here:
Age & Aging: What Can (And Can’t) We Do About It?
Now, onwards…
It is unreasonable to expect to live past 100: True or False?
True or False, depending on your own circumstances.
First, external circumstances: the modal average person in Hong Kong is currently in their 50s and can expect to live into their late 80s, while the modal average person in Gaza is 14 and may not expect to make it to 15 right now.
To avoid extremes, let’s look at the US, where the modal average person is currently in their 30s and can expect to live into their 70s:
United States Mortality Database
Now, before that unduly worries our many readers already in their 70s…
Next, personal circumstances: not just your health, but your socioeconomic standing. And in the US, one of the biggest factors is the kind of health insurance one has:
SOA Research Institute | Life Expectancy Calculator 2021
You may note that the above source puts all groups into a life expectancy in the 80s—whereas the previous source gave 70s.
Why is this? It’s because the SOA, whose primary job is calculating life insurance risks, is working from a sample of people who have, or are applying for, life insurance. So it misses out many people who die younger without such.
New advances in medical technology are helping people to live longer: True or False?
True, assuming access to those. Our subscribers are mostly in North America, and have an economic position that affords good access to healthcare. But beware…
On the one hand:
The number of people who live past the age of 100 has been on the rise for decades
On the other hand:
The average life expectancy in the U.S. has been on the decline for three consecutive years
COVID is, of course, largely to blame for that, though:
❝The decline of 1.8 years in life expectancy was primarily due to increases in mortality from COVID-19 (61.2% of the negative contribution).
The decline in life expectancy would have been even greater if not for the offsetting effects of decreases in mortality due to cancer (43.1%)❞
Source: National Vital Statistics Reports
The US stats are applicable to Canada, the UK, and Australia: True or False?
False: it’s not quite so universal. Differences in healthcare systems will account for a lot, but there are other factors too:
- Life expectancy in Canada fell for the 3rd year in a row. What’s happening?
- UK life expectancy lagging behind rest of G7 except the US
- Australians are living longer but what does it take to reach 100 years old?
Here’s an interesting (UK-based) tool that calculates not just your life expectancy, but also gives the odds of living to various ages (e.g. this writer was given odds of living to 87, 96, 100).
Check yours here:
Office of National Statistics | Life Expectancy Calculator
To finish on a cheery note…
Data from Italian centenarians suggests a “mortality plateau”:
❝The risk of dying leveled off in people 105 and older, the team reports online today in Science.
That means a 106-year-old has the same probability of living to 107 as a 111-year-old does of living to 112.
Furthermore, when the researchers broke down the data by the subjects’ year of birth, they noticed that over time, more people appear to be reaching age 105.❞
Pop-sci source: Once you hit this age, aging appears to stop
Actual paper: The plateau of human mortality: demography of longevity pioneers
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: