“Why Does It Hurt When I Have Sex?” (And What To Do About It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is one that affects mostly women, with 43% of American women reporting such issues at some point. There’s a distribution curve to this, with higher incidence in younger and older women; younger while first figuring things out, and older with menopause-related body changes. But, it can happen at any time (and often not for obvious reasons!), so here’s what OB/GYN Dr. Jennifer Lincoln advises:
Many possibilities, but easily narrowed down
Common causes include:
- vaginal dryness, which itself can have many causes (half of which are “low estrogen levels” for various different reasons)
- muscular issues, which can be in response to anxiety, pain, and occur as a result of pelvic floor muscle tightening
- vulvar issues, ranging from skin disorders (e.g. lichen sclerosis or lichen planus) to nerve disorders (e.g. vestibulitis or vestibulodynia)
- uterine issues, including endometriosis, fibroids, or scar tissue if you had a surgery
- infections, of the STI variety, but bear in mind that some STIs such as herpes do not necessarily require direct sexual contact per se, and yeast infections definitely don’t. Some STIs are more serious than others, so getting things checked out is a good idea (don’t worry, clinics are discreet about this sort of thing)
- bowel issues, notwithstanding that we have been talking about vaginal sex here, it can’t be happy if its anatomical neighbors aren’t happy—so things like IBS, Crohn’s, or even just constipation, aren’t irrelevant
- trauma, of various kinds, affecting sexual experiences
That’s a lot of possibilities, so if there’s not something standing out as “yes, now that you mention it, it’s obviously that”, Dr. Lincoln recommends a full health evaluation and examination of medical history, as well as a targeted physical exam. That may not be fun, but at least, once it’s done, it’s done.
Treatments vary depending on the cause, of course, and there are many kinds of physical and psychological therapies, as well as surgeries for the uterine issues we mentioned.
Happily, many of the above things can be addressed with simpler and less invasive methods, including learning more about the relevant anatomy and physiology and how to use it (be not ashamed; most people never got meaningful education about this!)*, vulvar skin care (“gentle” is the watchword here), the difference a good lube can make, and estrogen supplementation—which if you’re not up for general HRT, can be a topical estrogen cream that alleviates sexual function issues without raising blood serum estradiol levels.
*10almonds tip: check out the recommended book “Come As You Are” in our links below; it has 400 pages of stuff most people never knew about anatomy and physiology down there; you can thank us later!
Meanwhile, for more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Water-based Lubricant vs Silicon-based Lubricant – Which is Healthier? (counterintuitively, it’s the silicon! But do give it a quick read, because here be science)
- How To Avoid Urinary Tract Infections (may be relevant; always good to know)
- Come As You Are – by Dr. Emily Nagoski (book; if we could only recommend one book on responsible vagina ownership, this would be the one)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Studies of Parkinson’s disease have long overlooked Pacific populations – our work shows why that must change

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A form of Parkinson’s disease caused by mutations in a gene known as PINK1 has long been labelled rare. But our research shows it’s anything but – at least for some populations.
Our meta-analysis revealed that people in specific Polynesian communities have a much higher rate of PINK1-linked Parkinson’s than expected. This finding reshapes not only our understanding of who is most at risk, but also how soon symptoms may appear and what that might mean for treatment and testing.
Parkinson’s disease is often thought of as a single condition. In reality, it is better understood as a group of syndromes caused by different factors – genetic, environmental or a combination of both.
These varying causes lead to differences in disease patterns, progression and subsequent diagnosis. Recognising this distinction is crucial as it paves the way for targeted interventions and may even help prevent the disease altogether.

Shutterstock/sfam_photo Why we focus on PINK1-linked Parkinson’s
We became interested in this gene after a 2021 study highlighted five people of Samoan and Tongan descent living in New Zealand who shared the same PINK1 mutation.
Previously, this mutation had been spotted only in a few more distant places –Malaysia, Guam and the Philippines. The fact it appeared in people from Samoan and Tongan backgrounds suggested a historical connection dating back to early Polynesian migrations.
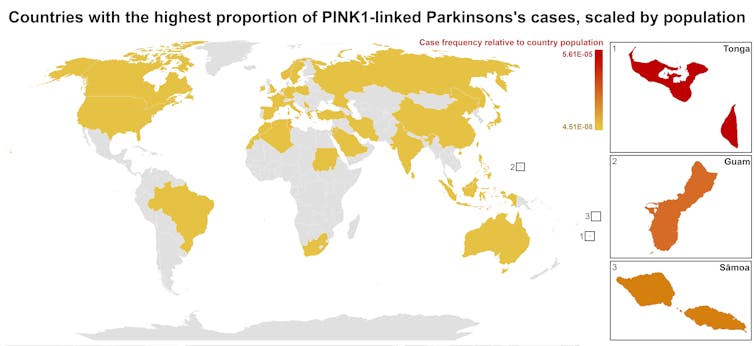
One person in 1,300 West Polynesians carries this mutation. This is a frequency well above what scientists usually classify as rare (below one in 2,200). This discovery means we may be overlooking entire communities in Parkinson’s research if we continue to assume PINK1-linked cases are uncommon.
This world map shows people in some Polynesian communities have a much higher rate of PINK1-linked Parkinson’s than the global population. Eden Yin, CC BY-SA Traditional understanding says PINK1-linked Parkinson’s is both rare and typically strikes younger people, mostly in their 30s or 40s, if they inherit two faulty copies of the gene. In other words, it’s considered a recessive condition, needing two matching puzzle pieces before the disease can unfold.
Our work challenges this view. We show that even one defective PINK1 gene can cause Parkinson’s at an average age of 43, much earlier than the typical onset after 65. That’s a significant departure from the standard belief that only people with two defective gene copies are at risk.
Why this matters for people with the disease
It’s not just genetics that challenge long-held views. Historically, PINK1-linked Parkinson’s was thought to lack some of the classic features of the disease, such as toxic clumps of alpha-synuclein protein.
In typical Parkinson’s, alpha-synuclein builds up in the brain, forming sticky clumps known as Lewy bodies. Our results, contrary to prior beliefs, show that alpha-synuclein pathology is present in 87.5% of PINK1 cases. This finding opens up a promising new avenue for future treatment development.
The biggest concern is early onset. PINK1-linked Parkinson’s can begin as early as 11 years old, although a more common starting point is around the mid-30s. This early onset means living longer with the disease, which can profoundly affect education, work opportunities and family life.
Current treatments (such as levodopa, a precursor of dopamine) help manage symptoms, but they’re not designed to address the root cause. If we know someone has a PINK1 mutation, scientists and clinicians can explore therapies for specific genetic pathways, potentially delivering relief beyond symptom management.
Sex differences add a layer of complexity
In Parkinson’s, generally, men are at higher risk and tend to develop symptoms earlier. However, our findings suggest the opposite pattern for PINK1-linked cases. Particularly, women with two defective copies of the gene experience onset earlier than men.
This highlights the need to consider sex-related factors in Parkinson’s research. Overlooking them risks missing key elements of the disease.
Genetic testing could be a game-changer for PINK1-linked Parkinson’s. Because it often appears earlier, doctors may not recognise it immediately, especially if they are more familiar with the common, later-onset form of Parkinson’s.
Early genetic testing could lead to a faster, more accurate diagnosis, allowing treatment to begin when interventions are most effective. It would help families understand how the disease is inherited, enabling relatives to get tested.
In some cases, where appropriate and culturally acceptable, embryo screening may be considered to prevent the passing of the faulty gene.
Knowing you have a PINK1 mutation could also make finding the right treatment more efficient. Instead of a lengthy trial-and-error process with different medications, doctors could use emerging therapies designed to target the underlying PINK1 mutation rather than relying on general Parkinson’s treatments meant for the broader population.
Addressing research gaps
These findings underscore how crucial it is to include diverse populations in health research.
Many communities, such as those in Samoa, Tonga and other Pacific nations, have had little to no involvement in global Parkinson’s genetics studies. This has created gaps in knowledge and real-world consequences for people who may not receive timely or accurate diagnoses.
Researchers, funding bodies and policymakers must prioritise projects beyond the usual focus on European or industrialised countries to ensure research findings and treatments are relevant to all affected populations.
To better diagnose and treat Parkinson’s, we need a more inclusive approach. Recognising that PINK1-linked Parkinson’s is not as rare as previously thought – and that genetics, sex differences and cultural factors all play a role – allows us to improve care for everyone.
By expanding genetic testing, refining treatments and ensuring research reflects the full spectrum of Parkinson’s, we can move closer to more precise diagnoses, targeted therapies and better support systems for all.
Victor Dieriks, Research Fellow in Health Sciences, University of Auckland, Waipapa Taumata Rau and Eden Paige Yin, PhD candidate in Health Sciences, University of Auckland, Waipapa Taumata Rau
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Early Bird Or Night Owl? Genes vs Environment
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Sliding Slope?

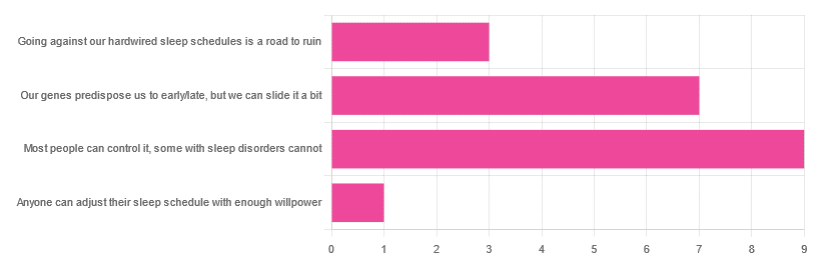
In Tuesday’s newsletter, we asked you how much control you believe we have over our sleep schedule, and got the above-depicted, below-described, set of responses:
- 45% said “most people can control it; some people with sleep disorders cannot
- 35% said “our genes predispose us to early/late, but we can slide it a bit
- 15% said: “going against our hardwired sleep schedules is a road to ruin”
- 5% said “anyone can adjust their sleep schedule with enough willpower”
You may be wondering: what’s with those single-digit numbers in the graph there? And the answer is: Tuesday’s email didn’t go out at the usual time due to a scheduling mistake (sorry!), which is probably what affected the number of responses (poll response levels vary, but are usually a lot higher than this).
Note: yes, this does mean most people who read our newsletter don’t vote. So, not to sound like a politician on the campaign trail, but… Your vote counts! We always love reading your comments when you add those, too—often they provide context that allow us to tailor what we focus on in our articles
However, those are the responses we got, so here we are!
What does the science say?
Anyone can adjust their sleep with enough willpower: True or False?
False, simply. It’s difficult for most people, but for many people with sleep disorders, it is outright impossible.
In a battle of narcolepsy vs willpower, for example, no amount of willpower will stop the brain from switching to sleep mode when it thinks it’s time to sleep:
❝Narcolepsy is the most common neurological cause of chronic sleepiness. The discovery about 20 years ago that narcolepsy is caused by selective loss of the neurons producing orexins sparked great advances in the field
[There is also] developing evidence that narcolepsy is an autoimmune disorder that may be caused by a T cell-mediated attack on the orexin neurons and explain how these new perspectives can inform better therapeutic approaches.❞
~ Dr. Carrie Mahoney et al. (lightly edited for brevity)
Source: The neurobiological basis of narcolepsy
For further reading, especially if this applies to you or a loved one:
Our genes predispose us to early/late, but we can slide it a bit: True or False?
True! First, about our genes predisposing us:
…and also:
Gene distinguishes early birds from night owls and helps predict time of death
Now, as for the “can slide it a bit”, this is really just a function of the general categories of “early bird” and “night owl” spanning periods of time that allow for a few hours’ wiggle-room at either side.
However, it is recommended to make any actual changes more gradually, with the Sleep Foundation going so far as to recommend 30 minutes, or even just 15 minutes, of change per day:
Sleep Foundation | How to Fix Your Sleep Schedule
Going against our hardwired sleep schedule is a road to ruin: True or False?
False, contextually. By this we mean: our “hardwired” sleep schedule is (for most of us), genetically predisposed but not predetermined.
Also, genetic predispositions are not necessarily always good for us; one would not argue, for example, for avoiding going against a genetic predisposition to addiction.
Some genetic predispositions are just plain bad for us, and genes can be a bit of a lottery.
That said, we do recommend getting some insider knowledge (literally), by getting personal genomics tests done, if that’s a viable option for you, so you know what’s really a genetic trait (and what to do with that information) and what’s probably caused by something else (and what to do with that information):
Genetic Testing: Health Benefits & Methods
Take care!
Share This Post
-

What’s behind rising heart attack rates in younger adults
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Deaths from heart attacks have been in decline for decades, thanks to improved diagnosis and treatments. But, among younger adults under 50 and those from communities that have been marginalized, the trend has reversed.
More young people have suffered heart attacks each year since the 2000s—and the reasons why aren’t always clear.
Here’s what you need to know about heart attack trends in younger adults.
Heart attack deaths began declining in the 1980s
Heart disease has been a leading cause of death in the United States for more than a century, but rates have declined for decades as diagnosis and treatments improved. In the 1950s, half of all Americans who had heart attacks died, compared to one in eight today.
A 2023 study found that heart attack deaths declined 4 percent a year between 1999 and 2020.
The downward trend plateaued in the 2000s as heart attacks in young adults rose
In 2012, the decline in heart disease deaths in the U.S. began to slow. A 2018 study revealed that a growing number of younger adults were suffering heart attacks, with women more affected than men. Additionally, younger adults made up one-third of heart attack hospitalizations, with one in five heart attack patients being under 40.
The following year, data showed that heart attack rates among adults under 40 had increased steadily since 2006. Even more troubling, young patients were just as likely to die from heart attacks as patients more than a decade older.
Why are more younger adults having heart attacks?
Heart attacks have historically been viewed as a condition that primarily affects older adults. So, what has changed in recent decades that puts younger adults at higher risk?
Higher rates of obesity, diabetes, and high blood pressure
Several leading risk factors for heart attacks are rising among younger adults.
Between 2009 and 2020, diabetes and obesity rates increased in Americans ages 20 to 44.During the same period, hypertension, or high blood pressure, rates did not improve in younger adults overall and worsened in young Hispanic people. Notably, young Black adults had hypertension rates nearly twice as high as the general population.
Hypertension significantly increases the risk of heart attack and cardiovascular death in young adults.
Increased substance use
Substance use of all kinds increases the risk of cardiovascular issues, including heart attacks. A recent study found that cardiovascular deaths associated with substance use increased by 4 percent annually between 1999 and 2019.
The rise in substance use-related deaths has accelerated since 2012 and was particularly pronounced among women, younger adults (25-39), American Indians and Alaska Natives, and those in rural areas.
Alcohol was linked to 65 percent of the deaths, but stimulants (like methamphetamine) and cannabis were the substances associated with the greatest increase in cardiovascular deaths during the study period.
Poor mental health
Depression and poor mental health have been linked to cardiovascular issues in young adults. A 2023 study of nearly 600,000 adults under 50 found that depression and self-reported poor mental health are a risk factor for heart disease, regardless of socioeconomic or other cardiovascular risk factors.
Adults under 50 years consistently report mental health conditions at around twice the rate of older adults. Additionally, U.S. depression rates have trended up and reached an all-time high in 2023, when 17.8 percent of adults reported having depression.
Depression rates are rising fastest among women, adults under 44, and Black and Hispanic populations.
COVID-19
COVID-19 can cause real, lasting damage to the heart, increasing the risk of certain cardiovascular diseases for up to a year after infection. Vaccination reduces the risk of heart attack and other cardiovascular events caused by COVID-19 infection.
The first year of the pandemic marked the largest single-year spike in heart-related deaths in five years, including a 14 percent increase in heart attacks. In the second year of the pandemic, heart attacks in young adults increased by 30 percent.
Heart attack prevention
Not every heart attack is preventable, but everyone can take steps to reduce their risks. The American Heart Association recommends managing health conditions that increase heart disease risk, including diabetes, obesity, and high blood pressure.
Lifestyle changes like improving diet, reducing substance use, and increasing physical activity can also help reduce heart attack risk.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post


Related Posts
-

Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?

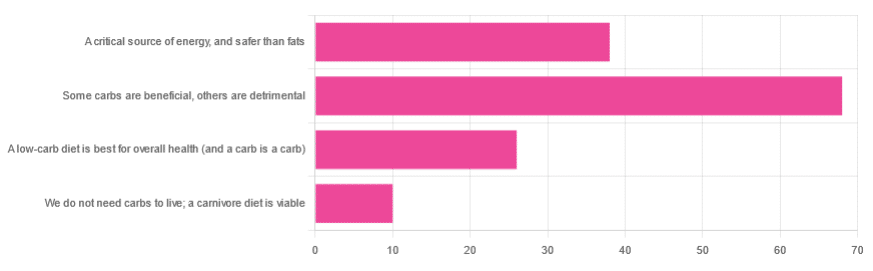
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Better Blood Sugar – by Dale Pinnock
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Previously featured as “The Medicinal Chef”, the author (a nutritionist) continues his mission to enable people to eat to beat whatever ails them. In this case, it’s about improving blood sugar stability—and by stability, of course we mean stability within a healthy range.
He talks us through why blood sugar matters, how insulin resistance occurs, the relationship between blood sugar and obesity, and then its connections with other systems and conditions—cardiovascular health, brain health, and even cancer.
Naturally (for a nutritionist) the tools he offers are mostly dietary tweaks (and other suggestions are closely related, such as supplements that can help), and his method does not involve drastic actions, so much as just improving one thing here, one thing there, etc until one is in good health in a sustainable fashion.
There are recipes, but this is not primarily a recipe book; rather, they are all contained in one chapter (specifically, chapter 10 of 11), and are indeed healthy options that’ll do what’s promised.
The style is strongly science-oriented, without being science-dense, and any scientific terms used are explained as we go along.
Bottom line: if you’d like healthier blood sugar levels, this book can help!
Click here to check out Better Blood Sugar, and get/keep yours at a healthy level!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Peaches vs Plums – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing peaches to plums, we picked the peaches.
Why?
Both are great! But there is a clear winner out of these two botanically-similar fruits:
In terms of macronutrients they are very similar. Peaches have slightly more protein and plums have slightly more carbs, but the numbers are close enough to make no meaningful difference; they’re both mostly water.
They’re also not too far from each other in the category of vitamins; peaches have more of vitamins B2, B3, B5, E, and choline, while plums have more of vitamins B1, B6, B9, C, and K. They’re equal on vitamin A, by the way, and the vitamins they do differ in, differ by around the same margins, so this category is a clear tie.
When it comes to minerals, however, peaches win easily with more copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. The two fruits are equal on calcium, and plum is not higher in any minerals.
While they already won easily because of the mineral situation, it should be noted that peaches also have the lower glycemic index. But honestly, plums are fine too; peaches are just even lower.
So: enjoy both, but if you’re going to pick one, peaches boast the most!
Want to learn more?
You might like to read:
- Top 8 Fruits That Prevent & Kill Cancer
- Apricots vs Peaches – Which is Healthier?
- Dried Apricots vs Dried Prunes – Which is Healthier? (prunes are dried plums, usually partially rehydrated)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: