What’s the difference between period pain and endometriosis pain?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Menstruation, or a period, is the bleeding that occurs about monthly in healthy people born with a uterus, from puberty to menopause. This happens when the endometrium, the tissue that lines the inside of the uterus, is shed.
Endometriosis is a condition that occurs when endometrium-like tissue is found outside the uterus, usually within the pelvic cavity. It is often considered a major cause of pelvic pain.
Pelvic pain significantly impacts quality of life. But how can you tell the difference between period pain and endometriosis?

Periods and period pain
Periods involve shedding the 4-6 millimetre-thick endometrial lining from the inside of the uterus.
As the lining detaches from the wall of the uterus, the blood vessels which previously supplied the lining bleed. The uterine muscles contract, expelling the blood and crumbled endometrium.
The crumbled endometrium and blood mostly pass through the cervix and vagina. But almost everyone back-bleeds via their fallopian tubes into their pelvic cavity. This is known as “retrograde menstruation”.

The process of menstrual shedding is caused by inflammatory substances, which also cause nausea, vomiting, diarrhoea, headaches, aches, pains, dizziness, feeling faint, as well as stimulating pain receptors.
These inflammatory substances are responsible for the pain and symptoms in the week before a period and the first few days.
For women with heavy periods, their worst days of pain are usually the heaviest days of their period, coinciding with more cramps to expel clots and more retrograde bleeding.
Many women also have pain when they are releasing an egg from their ovary at the time of ovulation. Ovulation or mid-cycle pain can be worse in those who bleed more, as those women are more likely to bleed into the ovulation follicle.
Around 90% of adolescents experience period pain. Among these adolescents, 20% will experience such severe period pain they need time off from school and miss activities. These symptoms are too often normalised, without validation or acknowledgement.
What about endometriosis?
Many symptoms have been attributed to endometriosis, including painful periods, pain with sex, bladder and bowel-related pain, low back pain and thigh pain.
Other pain-related conditions such migraines and chronic fatigue have also been linked to endometriosis. But these other pain-related symptoms occur equally often in people with pelvic pain who don’t have endometriosis.

Repeated, significant period and ovulation pain can eventually lead some people to develop persistent or chronic pelvic pain, which lasts longer than six months. This appears to occur through a process known as central sensitisation, where the brain becomes more sensitive to pain and other sensory stimuli.
Central sensitisation can occur in people with persistent pain, independent of the presence or absence of endometriosis.
Eventually, many people with period and/or persistent pelvic pain will have an operation called a laparoscopy, which allows surgeons to examine organs in the pelvis and abdomen, and diagnose and treat endometriosis.
Yet only 50% of those with identical pain symptoms who undergo a laparoscopy will end up having endometriosis.
Endometriosis is also found in pain-free women. So we cannot predict who does and doesn’t have endometriosis from symptoms alone.
How is this pain managed?
Endometriosis surgery usually involves removing lesions and adhesions. But at least 30% of people return to pre-surgery pain levels within six months or have more pain than before.
After surgery, emergency department presentations for pain are unchanged and 50% have repeat surgery within a few years.
Suppressing periods using hormonal therapies (such as continuous oral contraceptive pills or progesterone-only approaches) can suppress endometriosis and reduce or eliminate pain, independent of the presence or absence of endometriosis.
Not every type or dose of hormonal medications suits everyone, so medications need to be individualised.
The current gold-standard approach to manage persistent pelvic pain involves a multidisciplinary team approach, with the aim of achieving sustained remission and improving quality of life. This may include:
- physiotherapy for pelvic floor and other musculoskeletal problems
- management of bladder and bowel symptoms
- support for self-managing pain
- lifestyle changes including diet and exercise
- psychological or group therapy, as our moods, stress levels and childhood events can affect how we feel and experience pain.
Whether you have period pain, chronic pelvic pain or pain you think is associated with endometriosis, if you feel pain, it’s real. If it’s disrupting your life, you deserve to be taken seriously and treated as the whole person you are.
Sonia R. Grover, Senior Research Fellow, Murdoch Children’s Research Institute; Clinical Professor of Gynaecology, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is it dangerous to kiss someone who’s eaten gluten if you have coeliac disease?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Coeliac disease is not a food allergy or intolerance. It’s an autoimmune disease that makes the body attack the small intestine if gluten (a protein found in wheat, rye and barley) reaches the gut. Even a small amount – a tiny bread crumb – can cause damage and inflammation.
The only treatment is a gluten-free diet. This means completely eliminating foods containing the protein, such as pasta, bread, noodles and many processed products, and preparing food carefully to avoid cross-contamination.
But what about other forms of cross-contamination? One study surveyed 538 adults with coeliac disease about their dating habits and found 39% were hesitant to kiss their partners because of the disease.
But can gluten really be transferred this way, with a kiss? Research is only just beginning to look at this question – here’s what we know.

Lordn/Shutterstock How harmful is gluten for people with coeliac disease?
Coeliac disease is common: surveys representative of the population estimate it affects one in 70 Australians. However, it tends to be under-diagnosed. Research suggests only 20% of those with coeliac disease have a medical diagnosis.
This means most sufferers are unaware they have coeliac disease, despite experiencing unpleasant symptoms.
When untreated, coeliac disease can stop the small intestine absorbing nutrients and lead to gut symptoms such as diarrhoea, abdominal pain, bloating and flatulence. It can also result in non-gut symptoms such as fatigue, skin rashes and brain fog.
However, touching gluten won’t have any effect. Gluten only causes damage to people with coeliac disease if it enters the gut. This is why it can be effectively treated with a strict gluten-free diet.
How much gluten is harmful?
Researchers have investigated how much gluten can result in harm to people with coeliac disease. One study found some people with coeliac disease experienced damage to their small intestine with as little as 10 milligrams of gluten per day.
For context, one slice of bread contains 2.5 grams of gluten. A very small amount can cause damage if eaten, such a tiny crumb accidentally transferred from a chopping board or plate.
Australian researchers have determined that a dose of gluten below 3mg does not cause an immune response on very sensitive blood tests.
Even a bread crumb can be harmful to people with coeliac disease, if it’s eaten. Master1305/Shutterstock Food regulatory authorities look at how much gluten is concentrated in particular foods to decide what is “gluten free”. In most countries a diet containing gluten at less than 20 parts per million (or 20mg per kilogram) is considered to be safe for people with coeliac disease.
But Australia and New Zealand have much stricter requirements for labelling a food as “gluten free”. Testing methods in Australia allow for detection as low as three parts per million – this is known as the “limit of detection”. Foods below this limit contain no detectable gluten and can be labelled gluten free.
So, what about kissing?
What does this mean for kissing? Can enough gluten be transmitted from one person to another via saliva to cause problems? To date, there is very limited data.
New US research presented today looked at ten couples, each with one partner who had coeliac disease.
In the study, the non-coeliac partner ate ten crackers containing gluten before the couple kissed for ten seconds.
The researchers found gluten transfer was minimal in the saliva. When the non-coeliac partner had a glass of water after eating the crackers, the gluten in their saliva was less than 20 parts per million (the international limit for gluten-free products).
While this data has not yet been peer-reviewed, their preliminary finding seems to support similar research from 2022 which looked at peanut allergy and saliva to estimate gluten levels in saliva.
It estimated that saliva after eating gluten could contain around 250 micrograms of gluten – one-twelfth of the minimum amount (3mg) believed to cause an immune response.
This means, for people with coeliac disease, kissing should not be an issue to worry about.
Cross-contamination from foods containing gluten is the biggest risk for people with coeliac disease. Jacob Lund/Shutterstock Other risks
The bigger risk for people with coeliac disease continues to be exposure to gluten from food – even food labelled “gluten free”.
One study found seven out of 256 manufactured food products sold as gluten free had detectable levels of gluten, in some cases as much as 3mg in a single serving.
In 2018 another study found almost 10% of food sold as gluten free at cafes and restaurants across Melbourne actually contained gluten. One food sample contained a gluten concentration of more than 80 parts per million.
Still, given Australia has strictest regulations in the world, the risk of getting sick from eating gluten-free foods is quite low.
The risk from kissing? Even lower.
If you want to look out for your loved one with coeliac disease, how you prepare food is more important. This includes preventing cross-contamination by storing and preparing gluten-free foods well away from foods containing gluten, and thoroughly cleaning equipment and utensils after they’ve been in contact with food containing gluten.
And next time you’re on a date at your favourite eatery – whether they advertise as gluten free, or just have gluten-free items on the menu – it’s a good idea to politely ask about their food handling practices.
Vincent Ho, Associate Professor and Clinical Academic Gastroenterologist, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Shame and blame can create barriers to vaccination
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Understanding the stigma surrounding infectious diseases like HIV and mpox may help community health workers break down barriers that hinder access to care.
Looking back in history can provide valuable lessons to confront stigma in health care today, especially toward Black, Latine, LGBTQ+, and other historically underserved communities disproportionately affected by COVID-19 and HIV.
Public Good News spoke with Sam Brown, HIV prevention and wellness program manager at Civic Heart, a community-based organization in Houston’s historic Third Ward, to understand the effects of stigma around sexual health and vaccine uptake.
Brown shared more about Civic Heart’s efforts to provide free confidential testing for sexually transmitted infections, counseling and referrals, and information about COVID-19, flu, and mpox vaccinations, as well as the lessons they’re learning as they strive for vaccine equity.
Here’s what Brown said.
[Editor’s note: This content has been edited for clarity and length.]
PGN: Some people on social media have spread the myth that vaccines cause AIDS or other immune deficiencies when the opposite is true: Vaccines strengthen our immune systems to help protect against disease. Despite being frequently debunked, how do false claims like these impact the communities you serve?
Sam Brown: Misinformation like that is so hard to combat. And it makes the work and the path to overall community health hard because people will believe it. In the work that we do, 80 percent of it is changing people’s perspective on something they thought they knew.
You know, people don’t even transmit AIDS. People transmit HIV. So, a vaccine causing immunodeficiency doesn’t make sense.
With the communities we serve, we might have a person that will believe the myth, and because they believe it, they won’t get vaccinated. Then later, they may test positive for COVID-19.
And depending on social determinants of health, it can impact them in a whole heap of ways: That person is now missing work, they’re not able to provide for their family—if they have a family. It’s this mindset that can impact a person’s life, their income, their ability to function.
So, to not take advantage of something like a vaccine that’s affordable, or free for the most part, just because of misinformation or a misunderstanding—that’s detrimental, you know.
For example, when we talk to people in the community, many don’t know that they can get mpox from their pet, or that it’s zoonotic—that means that it can be transferred between different species or different beings, from animals to people. I see a lot of surprise and shock [when people learn this].
It’s difficult because we have to fight the misinformation and the stigma that comes with it. And it can be a big barrier.
People misunderstand. [They] think that “this is something that gay people or the LGBTQ+ community get,” which is stigmatizing and comes off as blaming. And blaming is the thing that leads us to be misinformed.
PGN: In the last couple years, your organization’s HIV Wellness program has taken on promoting COVID-19, flu, and mpox vaccines to the communities you serve. How do you navigate conversations between sexual health and infectious diseases? Can you share more about your messaging strategies?
S.B.: As we promoted positive sexual health and HIV prevention, we saw people were tired of hearing about HIV. They were tired of hearing about how PrEP works, or how to prevent HIV.
But, when we had an outbreak of syphilis in Houston just last year, people were more inclined to test because of the severity of the outbreak.
So, what our team learned is that sometimes you have to change the message to get people what they need.
We changed our message to highlight more syphilis information and saw that we were able to get more people tested for HIV because we correlated how syphilis and HIV are connected and how a person can be susceptible to both.
Using messages that the community wants and pairing them with what the community needs has been better for us. And we see that same thing with COVID-19, the flu, and RSV. Sometimes you just can’t be married to a message. We’ve had to be flexible to meet our clients where they are to help them move from unsafe practices to practices that are healthy and good for them and their communities.
PGN: You’ve mentioned how hard it is to combat stigma in your work. How do you effectively address it when talking to people one-on-one?
S.B.: What I understand is that no one wants to feel shame. What I see people respond to is, “Here’s an opportunity to do something different. Maybe there was information that you didn’t know that caused you to make a bad decision. And now here’s an opportunity to gain information so that you can make a better decision.”
People want to do what they want to do; they want to live how they want to live. And we all should be able to do that as long as it’s not hurting anyone, but also being responsible enough to understand that, you know, COVID-19 is here.
So, instead of shaming and blaming, it’s best to make yourself aware and understand what it is and how to treat it. Because the real enemy is the virus—it’s the infection, not the people.
When we do our work, we want to make sure that we come from a strengths-based approach. We always look at what a client can do, what that client has. We want to make sure that we’re empowering them from that point. So, even if they choose not to prioritize our message right now, we can’t take that personally. We’ll just use it as a chance to try a new way of framing it to help people understand what we’re trying to say.
And sometimes that can be difficult, even for organizations. But getting past that difficulty comes with a greater opportunity to impact someone else.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Share This Post
-

The Other Significant Others – by Rhaina Cohen
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As we get older, it’s a function of statistics that increasingly many of us are divorced or widowed. While some will—after whatever time seems right to them—get back into dating, what about those of us who decide that we won’t?
Rhaina Cohen explores the importance of friendship, mutual support, and (Platonic!) closeness and yes, even kinds of intimacy (for that too can be Platonic!) as we go on.
Even from a purely evolutionary approach, we are fundamentally social creatures, and while as individuals we may exist on a spectrum from reclusive to extroverted, we all thrive better when we at least have access to community and friends.
The style of the book is easy-reading and exploratory, and is very compelling as a call-to-arms for those who may wish to give/receive support to/from those with whom we are not necessarily sleeping.
Because at the end of the day, why should sex and/or romance be a required feature for legal protections? Aren’t we adults who can make our own decisions about whom we trust to care for us?
Bottom line: if you’re happily partnered and expect to pre-decease your partner, this book might not be directly important for you (it might for your partner, though). Everyone else? This book may be important at some point. That point might even be now already; only you know.
Click here to check out The Other Significant Others, and make your own choices in life!
Share This Post





Related Posts
-

What’s the difference between vegan and vegetarian?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
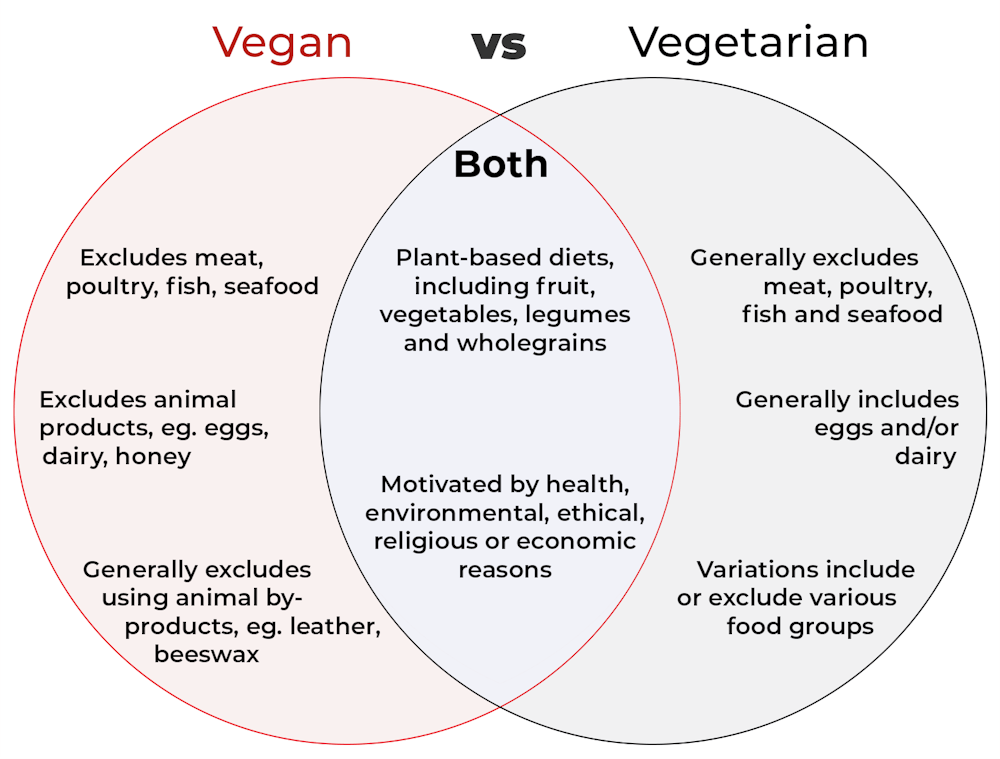
Vegan and vegetarian diets are plant-based diets. Both include plant foods, such as fruits, vegetables, legumes and whole grains.
But there are important differences, and knowing what you can and can’t eat when it comes to a vegan and vegetarian diet can be confusing.
So, what’s the main difference?
Creative Cat Studio/Shutterstock What’s a vegan diet?
A vegan diet is an entirely plant-based diet. It doesn’t include any meat and animal products. So, no meat, poultry, fish, seafood, eggs, dairy or honey.
What’s a vegetarian diet?
A vegetarian diet is a plant-based diet that generally excludes meat, poultry, fish and seafood, but can include animal products. So, unlike a vegan diet, a vegetarian diet can include eggs, dairy and honey.
But you may be wondering why you’ve heard of vegetarians who eat fish, vegetarians who don’t eat eggs, vegetarians who don’t eat dairy, and even vegetarians who eat some meat. Well, it’s because there are variations on a vegetarian diet:
- a lacto-ovo vegetarian diet excludes meat, poultry, fish and seafood, but includes eggs, dairy and honey
- an ovo-vegetarian diet excludes meat, poultry, fish, seafood and dairy, but includes eggs and honey
- a lacto-vegetarian diet excludes meat, poultry, fish, seafood and eggs, but includes dairy and honey
- a pescatarian diet excludes meat and poultry, but includes eggs, dairy, honey, fish and seafood
- a flexitarian, or semi-vegetarian diet, includes eggs, dairy and honey and may include small amounts of meat, poultry, fish and seafood.
Are these diets healthy?
A 2023 review looked at the health effects of vegetarian and vegan diets from two types of study.
Observational studies followed people over the years to see how their diets were linked to their health. In these studies, eating a vegetarian diet was associated with a lower risk of developing cardiovascular disease (such as heart disease or a stroke), diabetes, hypertension (high blood pressure), dementia and cancer.
For example, in a study of 44,561 participants, the risk of heart disease was 32% lower in vegetarians than non-vegetarians after an average follow-up of nearly 12 years.
Further evidence came from randomised controlled trials. These instruct study participants to eat a specific diet for a specific period of time and monitor their health throughout. These studies showed eating a vegetarian or vegan diet led to reductions in weight, blood pressure, and levels of unhealthy cholesterol.
For example, one analysis combined data from seven randomised controlled trials. This so-called meta-analysis included data from 311 participants. It showed eating a vegetarian diet was associated with a systolic blood pressure (the first number in your blood pressure reading) an average 5 mmHg lower compared with non-vegetarian diets.
It seems vegetarian diets are more likely to be healthier, across a number of measures.
For example, a 2022 meta-analysis combined the results of several observational studies. It concluded a vegetarian diet, rather than vegan diet, was recommended to prevent heart disease.
There is also evidence vegans are more likely to have bone fractures than vegetarians. This could be partly due to a lower body-mass index and a lower intake of nutrients such as calcium, vitamin D and protein.
But it can be about more than just food
Many vegans, where possible, do not use products that directly or indirectly involve using animals.
So vegans would not wear leather, wool or silk clothing, for example. And they would not use soaps or candles made from beeswax, or use products tested on animals.
The motivation for following a vegan or vegetarian diet can vary from person to person. Common motivations include health, environmental, ethical, religious or economic reasons.
And for many people who follow a vegan or vegetarian diet, this forms a central part of their identity.
More than a diet: veganism can form part of someone’s identity. Shutterstock So, should I adopt a vegan or vegetarian diet?
If you are thinking about a vegan or vegetarian diet, here are some things to consider:
- eating more plant foods does not automatically mean you are eating a healthier diet. Hot chips, biscuits and soft drinks can all be vegan or vegetarian foods. And many plant-based alternatives, such as plant-based sausages, can be high in added salt
- meeting the nutrient intake targets for vitamin B12, iron, calcium, and iodine requires more careful planning while on a vegan or vegetarian diet. This is because meat, seafood and animal products are good sources of these vitamins and minerals
- eating a plant-based diet doesn’t necessarily mean excluding all meat and animal products. A healthy flexitarian diet prioritises eating more whole plant-foods, such as vegetables and beans, and less processed meat, such as bacon and sausages
- the Australian Dietary Guidelines recommend eating a wide variety of foods from the five food groups (fruit, vegetables, cereals, lean meat and/or their alternatives and reduced-fat dairy products and/or their alternatives). So if you are eating animal products, choose lean, reduced-fat meats and dairy products and limit processed meats.
Katherine Livingstone, NHMRC Emerging Leadership Fellow and Senior Research Fellow at the Institute for Physical Activity and Nutrition, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Okra vs Peas – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing okra to peas, we picked the peas.
Why?
Both are great, but…
In terms of macros, peas have nearly 2x the fiber, 2x the carbs, and 3x the protein, winning this round.
In the category of vitamins, okra has more of vitmains B5, B6, E, and K, while peas have more of vitamins A, B1, B3, B3, B7, B9, C, and choline, winning another round.
Looking at minerals, okra has more calcium, magnesium, manganese, and potassium, while peas have more copper, iron, phosphorus, selenium, and zinc, for a marginal victory in the third round.
Adding up the sections makes for a clear overall win for peas, but by all means enjoy either or both; diversity is good!
Want to learn more?
You might like:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Procrastination Cure – by Jeffery Combs
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Why do we procrastinate? It’s not usually because we are lazy, and in fact we can often make ourselves very busy while procrastinating. And at some point, the bad feelings about procrastinating become worse than the experience of actually doing the thing. And still we often procrastinate. So, why?
Jeffery Combs notes that the reasons can vary, but generally fall into six mostly-distinct categories. He calls them:
- The neurotic perfectionist
- The big deal chaser
- The chronic worrier
- The rebellious rebel
- The drama addict
- The angry giver
These may overlap somewhat, but the differences are important when it comes to differences of tackling them.
Giving many illustrative examples, Combs gives the reader all we’ll need to know which category (or categories!) we fall into.
Then, he draws heavily on the work of Dr. Albert Ellis to find ways to change the feelings that we have that are holding us back.
Those feelings might be fear, shame, resentment, overwhelm, or something else entirely, but the tools are in this book.
A particular strength of this book is that it takes an approach that’s essentially Rational Emotive Behavior Therapy (REBT) repackaged for a less clinically-inclined audience (Combs’ own background is in marketing, not pyschology). Thus, for many readers, this will tend to make the ideas more relatable, and the implementations more accessible.
Bottom line: if you’ve been meaning to figure out how to beat your procrastination, but have been putting it off, now’s the time to do it.
Click here to check out The Procrastination Cure sooner rather than later!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: