What is ‘doll therapy’ for people with dementia? And is it backed by science?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The way people living with dementia experience the world can change as the disease progresses. Their sense of reality or place in time can become distorted, which can cause agitation and distress.
One of the best ways to support people experiencing changes in perception and behaviour is to manage their environment. This can have profound benefits including reducing the need for sedatives.
One such strategy is the use of dolls as comfort aids.

What is ‘doll therapy’?
More appropriately referred to as “child representation”, lifelike dolls (also known as empathy dolls) can provide comfort for some people with dementia.
Memories from the distant past are often more salient than more recent events in dementia. This means that past experiences of parenthood and caring for young children may feel more “real” to a person with dementia than where they are now.
Hallucinations or delusions may also occur, where a person hears a baby crying or fears they have lost their baby.
Providing a doll can be a tangible way of reducing distress without invalidating the experience of the person with dementia.
Some people believe the doll is real
A recent case involving an aged care nurse mistreating a dementia patient’s therapy doll highlights the importance of appropriate training and support for care workers in this area.
For those who do become attached to a therapeutic doll, they will treat the doll as a real baby needing care and may therefore have a profound emotional response if the doll is mishandled.
It’s important to be guided by the person with dementia and only act as if it’s a real baby if the person themselves believes that is the case.
What does the evidence say about their use?
Evidence shows the use of empathy dolls may help reduce agitation and anxiety and improve overall quality of life in people living with dementia.
Child representation therapy falls under the banner of non-pharmacological approaches to dementia care. More specifically, the attachment to the doll may act as a form of reminiscence therapy, which involves using prompts to reconnect with past experiences.
Interacting with the dolls may also act as a form of sensory stimulation, where the person with dementia may gain comfort from touching and holding the doll. Sensory stimulation may support emotional well-being and aid commnication.
However, not all people living with dementia will respond to an empathy doll.

The introduction of a therapeutic doll needs to be done in conjunction with careful observation and consideration of the person’s background.
Empathy dolls may be inappropriate or less effective for those who have not previously cared for children or who may have experienced past birth trauma or the loss of a child.
Be guided by the person with dementia and how they respond to the doll.
Are there downsides?
The approach has attracted some controversy. It has been suggested that child representation therapy “infantilises” people living with dementia and may increase negative stigma.
Further, the attachment may become so strong that the person with dementia will become upset if someone else picks the doll up. This may create some difficulties in the presence of grandchildren or when cleaning the doll.
The introduction of child representation therapy may also require additional staff training and time. Non-pharmacological interventions such as child representation, however, have been shown to be cost-effective.
Could robots be the future?
The use of more interactive empathy dolls and pet-like robots is also gaining popularity.
While robots have been shown to be feasible and acceptable in dementia care, there remains some contention about their benefits.
While some studies have shown positive outcomes, including reduced agitation, others show no improvement in cognition, behaviour or quality of life among people with dementia.
Advances in artificial intelligence are also being used to help support people living with dementia and inform the community.
Viv and Friends, for example, are AI companions who appear on a screen and can interact with the person with dementia in real time. The AI character Viv has dementia and was co-created with women living with dementia using verbatim scripts of their words, insights and experiences. While Viv can share her experience of living with dementia, she can also be programmed to talk about common interests, such as gardening.
These companions are currently being trialled in some residential aged care facilities and to help educate people on the lived experience of dementia.
How should you respond to your loved one’s empathy doll?
While child representation can be a useful adjunct in dementia care, it requires sensitivity and appropriate consideration of the person’s needs.
People living with dementia may not perceive the social world the same way as a person without dementia. But a person living with dementia is not a child and should never be treated as one.
Ensure all family, friends and care workers are informed about the attachment to the empathy doll to help avoid unintentionally causing distress from inappropriate handling of the doll.
If using an interactive doll, ensure spare batteries are on hand.
Finally, it is important to reassess the attachment over time as the person’s response to the empathy doll may change.
Nikki-Anne Wilson, Postdoctoral Research Fellow, Neuroscience Research Australia (NeuRA), UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Parents are increasingly saying their child is ‘dysregulated’. What does that actually mean?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Welcome aboard the roller coaster of parenthood, where emotions run wild, tantrums reign supreme and love flows deep.
As children reach toddlerhood and beyond, parents adapt to manage their child’s big emotions and meltdowns. Parenting terminology has adapted too, with more parents describing their child as “dysregulated”.
But what does this actually mean?

ShUStudio/Shutterstock More than an emotion
Emotional dysregulation refers to challenges a child faces in recognising and expressing emotions, and managing emotional reactions in social settings.
This may involve either suppressing emotions or displaying exaggerated and intense emotional responses that get in the way of the child doing what they want or need to do.
“Dysregulation” is more than just feeling an emotion. An emotion is a signal, or cue, that can give us important insights to ourselves and our preferences, desires and goals.
An emotionally dysregulated brain is overwhelmed and overloaded (often, with distressing emotions like frustration, disappointment and fear) and is ready to fight, flight or freeze.
Developing emotional regulation
Emotion regulation is a skill that develops across childhood and is influenced by factors such as the child’s temperament and the emotional environment in which they are raised.
In the stage of emotional development where emotion regulation is a primary goal (around 3–5 years old), children begin exploring their surroundings and asserting their desires more actively.
A child’s temperament and upbringing affect how they regulate emotions. bluedog studio/Shutterstock It’s typical for them to experience emotional dysregulation when their initiatives are thwarted or criticised, leading to occasional tantrums or outbursts.
A typically developing child will see these types of outbursts reduce as their cognitive abilities become more sophisticated, usually around the age they start school.
Express, don’t suppress
Expressing emotions in childhood is crucial for social and emotional development. It involves the ability to convey feelings verbally and through facial expressions and body language.
When children struggle with emotional expression, it can manifest in various ways, such as difficulty in being understood, flat facial expressions even in emotionally charged situations, challenges in forming close relationships, and indecisiveness.
Several factors, including anxiety, attention-deficit hyperactivity disorder (ADHD), autism, giftedness, rigidity and both mild and significant trauma experiences, can contribute to these issues.
Common mistakes parents can make is dismissing emotions, or distracting children away from how they feel.
These strategies don’t work and increase feelings of overwhelm. In the long term, they fail to equip children with the skills to identify, express and communicate their emotions, making them vulnerable to future emotional difficulties.
We need to help children move compassionately towards their difficulties, rather than away from them. Parents need to do this for themselves too.
Caregiving and skill modelling
Parents are responsible for creating an emotional climate that facilitates the development of emotion regulation skills.
Parents’ own modelling of emotion regulation when they feel distressed. The way they respond to the expression of emotions in their children, contributes to how children understand and regulate their own emotions.
Children are hardwired to be attuned to their caregivers’ emotions, moods, and coping as this is integral to their survival. In fact, their biggest threat to a child is their caregiver not being OK.
Unsafe, unpredictable, or chaotic home environments rarely give children exposure to healthy emotion expression and regulation. Children who go through maltreatment have a harder time controlling their emotions, needing more brainpower for tasks that involve managing feelings. This struggle could lead to more problems with emotions later on, like feeling anxious and hypervigilant to potential threats.
Recognising and addressing these challenges early on is essential for supporting children’s emotional wellbeing and development.
A dysregulated brain and body
When kids enter “fight or flight” mode, they often struggle to cope or listen to reason. When children experience acute stress, they may respond instinctively without pausing to consider strategies or logic.
If your child is in fight mode, you might observe behaviours such as crying , clenching fists or jaw, kicking, punching, biting, swearing, spitting or screaming.
In flight mode, they may appear restless, have darting eyes, exhibit excessive fidgeting, breathe rapidly, or try to run away.
A shut-down response may look like fainting or a panic attack.
When a child feels threatened, their brain’s frontal lobe, responsible for rational thinking and problem-solving, essentially goes offline.
The amygdala, shown here in red, triggers survival mode. pikovit/Shutterstock This happens when the amygdala, the brain’s alarm system, sends out a false alarm, triggering the survival instinct.
In this state, a child may not be able to access higher functions like reasoning or decision-making.
While our instinct might be to immediately fix the problem, staying present with our child during these moments is more effective. It’s about providing support and understanding until they feel safe enough to engage their higher brain functions again.
Reframe your thinking so you see your child as having a problem – not being the problem.
Tips for parents
Take turns discussing the highs and lows of the day at meal times. This is a chance for you to be curious, acknowledge and label feelings, and model that you, too, experience a range of emotions that require you to put into practice skills to cope and has shown evidence in numerous physical, social-emotional, academic and behavioural benefits.
Talk about your day over dinner. Monkey Business Images/Shutterstock Spending even small amounts (five minutes a day!) of quality one-on-one time with your child is an investment in your child’s emotional wellbeing. Let them pick the activity, do your best to follow their lead, and try to notice and comment on the things they do well, like creative ideas, persevering when things are difficult, and being gentle or kind.
Take a tip from parents of children with neurodiversity: learn about your unique child. Approaching your child’s emotions, temperament, and behaviours with curiosity can help you to help them develop emotion regulation skills.
When to get help
If emotion dysregulation is a persistent issue that is getting in the way of your child feeling happy, calm, or confident – or interfering with learning or important relationships with family members or peers – talk to their GP about engaging with a mental health professional.
Many families have found parenting programs helpful in creating a climate where emotions can be safely expressed and shared.
Remember, you can’t pour from an empty cup. Parenting requires you to be your best self and tend to your needs first to see your child flourish.
Cher McGillivray, Assistant Professor Psychology Department, Bond University and Shawna Mastro Campbell, Assistant Professor Psychology, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Beyond Guarding Against Dementia
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Age’s Brain-Changes Come Knocking

This is Dr. Amy Friday. She’s a psychologist, specializing in geropsychology and neuropsychological assessments.
In other words, she helps people optimize their aging experience, particularly in the context of brain changes as we get older.
What does she want us to know?
First: be not afraid
Ominous first words, but the fact is, there’s a lot to find scary about the prospect of memory loss, dementia, and death.
However, as she points out:
- Death will come for us all sooner or later, barring technology as yet unknown
- Dementia can be avoided, or at least stalled, or at least worked around
- Memory loss, as per the above, can be avoided/stalled/managed
We’ve written a little on these topics too:
…or if the death is not yours:
As for avoiding dementia, the below-linked feature is about Alzheimer’s in particular (which accounts for more than half of all cases of dementia), but the advice goes for most of the other kinds too:
How To Reduce Your Alzheimer’s Risk
And finally, about memory loss specifically:
How To Boost Your Memory Immediately (Without Supplements)
this one is especially about cementing into one’s brain the kinds of memories that people most fear losing with age. People don’t worry about forgetting their PIN codes; they worry about forgetting their cherished memories with loved ones. So, if that’s important to you, do consider checking out this one!
What is that about managing or working around the symptoms?
If we’re missing a limb, we (usually) get a prosthetic, and/or learn how to operate without that limb.
If we’re missing sight or hearing, partially or fully, there are disability aids for those kinds of things too (glasses are a disability aid! Something being very common does not make it not a disability; you literally have less of an ability—in this case, the ability to see), and/or we learn how to operate with our different (or missing) sense.
Dr. Friday makes the case for this being the same with memory loss, dementia, and other age-related symptoms (reduced focus, increased mental fatigue, etc):
❝We are all screwed up. Here’s my flavor … what’s yours? This is a favorite saying of mine, because we ARE all screwed up in one way or another, and when we acknowledge it we can feel closer in our screwed-up-edness.
We are all experiencing “normal aging,” so that tip-of-the-tongue phenomenon that starts in our thirties and slowly gets worse is REAL. But what if you’re having more problems than normal aging? Is it time to throw in the towel and hide? I’m hoping that there is a group of people who say HELL NO to that idea.
Let’s use lessons from research and clinical practice to help all of us work around our weaknesses, and capitalize on our strengths. ❞
Examples of this might include:
- Writing down the things most important to you (a short list of information and/or statements that you feel define you and what matters most to you), so that you can read it later
- Making sure you have support (partner, family, friends, etc) who are on the same page about this topic—and thus will actually support you and advocate for you, instead of arguing about what is in your best interest without consulting you.
- Labelling stuff around the house, so that you get less confused about what is what and where it is
- Having a named go-to advocate that you can call / ask to be called, if you are in trouble somewhere and need help that you can rely on
- Getting a specialized, simpler bank account; hiring an accountant if relevant and practicable.
The thing is, we all want to keep control. Sometimes we can do that! Sometimes we can’t, and if we’re going to lose some aspect of control, it’ll generally go a lot better if we do it on our own terms, so that we ourselves can look out for future-us in our planning.
Want to know more?
You might enjoy her blog, which includes also links to her many videos on the topic, including such items as:
- Neuroplasticity – #1 Way To Increase Brain Health
- Which Diet PREVENTS Alzheimer’s? | Best Brain Health Diet
- Stop Anxiety About Dementia & Do I Have Dementia?
For the rest, see:
This Beautiful Brain | The Science Of Brain Health
Enjoy!
Share This Post
-

The Evidence-Based Skincare That Beats Product-Specific Hype
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A million videos on YouTube will try to sell you a 17-step skincare routine, or a 1-ingredient magical fix that’s messy and inconvenient enough you’ll do it once and then discard it. This one takes a simple, scientific approach instead.
The Basics That Count
Ali Abdaal, known for his productivity hacks channel, enlisted the help of his friend, dermatologist Dr. Usama Syed, who recommends the following 3–4 things:
- Moisturize twice per day. Skin acts as a barrier, locking in moisture and protecting against irritants. Moisturizers replenish fats and proteins, maintaining this barrier and preventing dry, inflamed, and itchy skin. He uses CeraVe, but if you have one you know works well with your skin, stick with that, because skin comes in many varieties and yours might not be like his.
- Use sunscreen every day. Your phone’s weather app should comment on your local UV index. If it’s “moderate” or above, then sunscreen is a must—even if you aren’t someone who burns easily at all, the critical thing here is avoiding UV radiation causing DNA mutations in skin cells, leading to wrinkles, dark spots, and potentially skin cancer. Use a broad-spectrum sunscreen, ideally SPF 50.
- Use a retinoid. Retinoids are vitamin A-based and offer anti-aging benefits by promoting collagen growth, reducing pigmentation, and accelerating skin cell regeneration. Retinols are weaker, over-the-counter options, while stronger retinoids may require a prescription. Start gently with low dosage, whatever you choose, as initially they can cause dryness or sensitivity, before making everything better. He recommends adapalene as a starter retinoid (such as Differen gel, to give an example brand name).
- Optional: use a cleanser. Cleansers remove oils and dirt that water alone can’t. He recommends using a hydrating cleanser, to avoid stripping natural healthy oils as well as unwanted ones. That said, a cleanser is probably only beneficial if your skin tends towards the oily end of the dry-to-oily spectrum.
For more on all of these, plus an example routine, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post




-
Ozempic’s cousin drug liraglutide is about to get cheaper. But how does it stack up?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Fourteen years ago, the older drug cousin of semaglutide (Ozempic and Wegovy) came onto the market. The drug, liraglutide, is sold under the brand names Victoza and Saxenda.
Patents for Victoza and Saxenda have now expried. So other drug companies are working to develop “generic” versions. These are likely be a fraction of current cost, which is around A$400 a month.
So how does liraglutide compare with semaglutide?
Halfpoint/Shutterstock How do these drugs work?
Liraglutide was not originally developed as a weight-loss treatment. Like semaglutide (Ozempic), it originally treated type 2 diabetes.
The class of drugs liraglutide and semaglutide belong to are known as GLP-1 mimetics, meaning they mimic the natural hormone GLP-1. This hormone is released from your small intestines in response to food and acts in several ways to improve the way your body handles glucose (sugar).
How do they stop hunger?
Liraglutide acts in several regions of the unconscious part of your brain, specifically the hypothalamus, which controls metabolism, and parts of the brain stem responsible for communicating your body’s nutrient status to the hypothalamus.
Its actions here appear to reduce hunger in two different ways. First, it helps you to feel full earlier, making smaller meals more satisfying. Second, it alters your “motivational salience” towards food, meaning it reduces the amount of food you seek out.
Liraglutide’s original formulation, designed to treat type 2 diabetes, was marketed as Victoza. Its ability to cause weight loss was evident soon after it entered the market.
Shortly after, a stronger formulation, called Saxenda, was released, which was intended for weight loss in people with obesity.
How much weight can you lose with liraglutide?
People respond differently and will lose different amounts of weight. But here, we’ll note the average weight loss users can expect. Some will lose more (sometimes much more), others will lose less, and a small proportion won’t respond.
The first GLP-1 mimicking drug was exenatide (Bayetta). It’s still available for treating type 2 diabetes, but there are currently no generics. Exenatide does provide some weight loss, but this is quite modest, typically around 3-5% of body weight.
For liraglutide, those using the drug to treat obesity will use the stronger one (Saxenda), which typically gives about 10% weight loss.
Semaglutide, with the stronger formulation called Wegovy, typically results in 15% weight loss.
The newest GLP-1 mimicking drug on the market, tirzepatide (Mounjaro for type 2 diabetes and Zepbound for weight loss), results in weight loss of around 25% of body weight.
What happens when you stop taking them?
Despite the effectiveness of these medications in helping with weight loss, they do not appear to change people’s weight set-point.
So in many cases, when people stop taking them, they experience a rebound toward their original weight.
People often regain weight when when they stop taking the drug. Mohammed_Al_Ali/Shutterstock What is the dose and how often do you need to take it?
Liraglutide (Victoza) for type 2 diabetes is exactly the same drug as Saxenda for weight loss, but Saxenda is a higher dose.
Although the target for each formulation is the same (the GLP-1 receptor), for glucose control in type 2 diabetes, liraglutide has to (mainly) reach the pancreas.
But to achieve weight loss, it has to reach parts of the brain. This means crossing the blood-brain barrier – and not all of it makes it, meaning more has to be taken.
All the current formulations of GLP-1 mimicking drug are injectables. This won’t change when liraglutide generics hit the market.
However, they differ in how frequently they need to be injected. Liraglutide is a once-daily injection, whereas semaglutide and tirzepatide are once-weekly. (That makes semaglutide and tirzepatide much more attractive, but we won’t see semaglutide as a generic until 2033.)
What are the side effects?
Because all these medicines have the same target in the body, they mostly have the same side effects.
The most common are a range of gastrointestinal upsets including nausea, vomiting, bloating, constipation and diarrhoea. These occur, in part, because these medications slow the movement of food out of the stomach, but are generally managed by increasing the dose slowly.
Recent clinical data suggests the slowing in emptying of the stomach can be problematic for some people, and may increase the risk of of food entering the lungs during operations, so it is important to let your doctor know if you are taking any of these drugs.
Because these are injectables, they can also lead to injection-site reactions.
Gastrointestinal side effects are most common. Halfpoint/Shutterstock During clinical trials, there were some reports of thyroid disease and pancreatitis (inflammation of the pancreas). However, it is not clear that these can be attributed to GLP-1 mimicking drugs.
In animals, GLP-1 mimicking drugs drugs have been found to negatively alter the growth of the embryo. There is currently no controlled clinical trial data on their use during pregnancy, but based on animal data, these medicines should not be used during pregnancy.
Who can use them?
The GLP-1 mimicking drugs for weight loss (Wegovy, Saxenda, Zepbound/Mounjaro) are approved for use by people with obesity and are meant to only be used in conjunction with diet and exercise.
These drugs must be prescribed by a doctor and for obesity are not covered by the Pharmaceutical Benefits Scheme, which is one of the reasons why they are expensive. But in time, generic versions of liraglutide are likely to be more affordable.
Sebastian Furness, ARC Future Fellow, School of Biomedical Sciences, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
World Menopause Day Health News Round-Up
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In order to provide variety in this week’s round-up, not all of this is menopause-related, but it is all important:
Menopause & CVD
Untreated menopause is associated with higher incidence of heart disease, and higher mortality. People often forget about how much estrogen does for us (well, for those of us with a physiology running on estrogen, anyway; gentlemen, your testosterone is fine for you), and think it is “just” a sex hormone, but it’s a lot more.
Read in full: Menopause transition linked to increased heart disease risk
Related: What Menopause Does To The Heart
Extraterrestrial medical technology
The much lower gravity in Earth orbit has allowed for tissue engineering techniques that Earth’s normal gravity imposes limitations on. This is big news, because it means that rather than replacing a whole liver, tissue implants could be grafted, allowing the extant liver to repair itself (something livers are famously good at, but they need enough undamaged base material to work with).
Read in full: How liver tissue from the International Space Station may transform tissue engineering
Related: How To Unfatty A Fatty Liver
One thing and then another
As if endometriosis weren’t unpleasant enough in and of itself, the endothelial dysfunction inherent to it also raises cardiovascular disease risk. This is important, because while endometriosis has (like many maladies predominantly affecting women) generally been shrugged off by the medical world as an unhappy inconvenience but not life-threatening, now we know it comes with extra existential risks too:
Read in full: Understanding cardiovascular risks in endometriosis patients
Related: What You Need To Know About Endometriosis
Push-button meditation
Unlike mindfulness meditation, listening to music is a very passive experience, and thus requires less effort from the user. And yet, it has been associated with lower perceived pain levels, lower self-reported anxiety levels, less opioid use, and measurably lower heart-rate.
Read in full: Listening to music may speed up recovery from surgery, research suggests
Related: Nobody Likes Surgery, But Here’s How To Make It Much Less Bad
Cholesterol in menopause: quality over quantity
Much like previous research has shown that the quantity of LDL is not nearly so predictive of health outcomes in women as it is in men, this study into HDL and menopausal women shows that quantity of HDL does not matter nearly so much as the quality of it.
Read in full: HDL quality, not quantity, contribute to the first sign of Alzheimer’s disease in women
Related: Statins: His & Hers? ← consistent with the above, statins (to lower LDL cholesterol) generally help more for men and produce more adverse side effects for women. So again, a case of “the actual amount of cholesterol isn’t so important for women as for men”.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between shyness and social anxiety?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
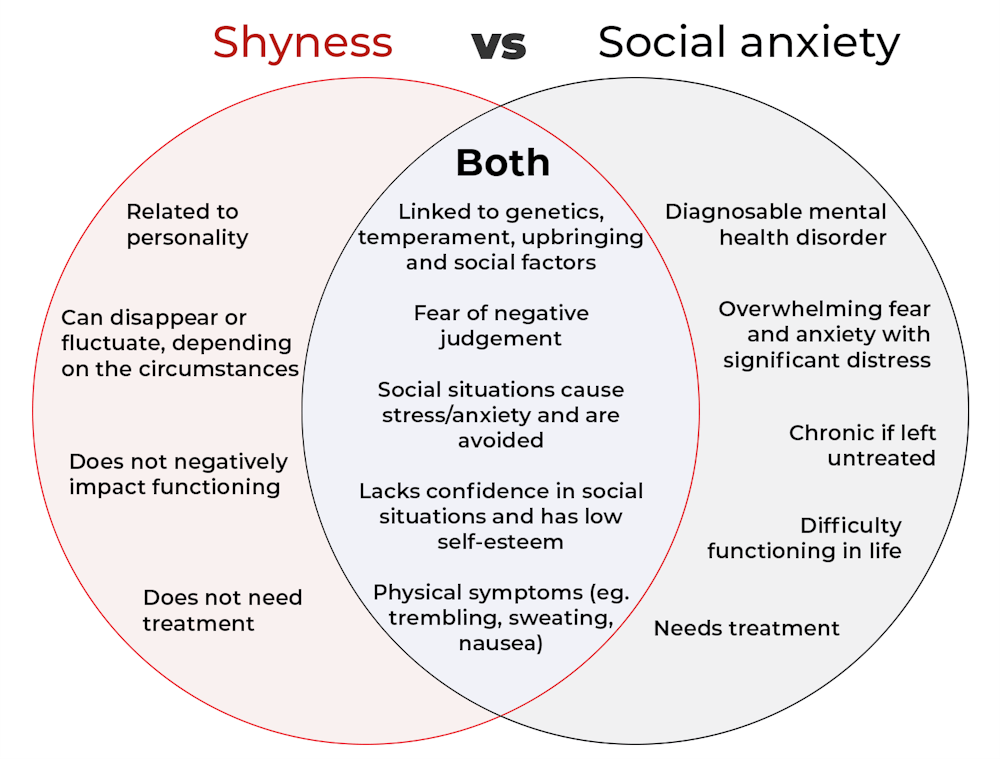
The terms “shyness” and “social anxiety” are often used interchangeably because they both involve feeling uncomfortable in social situations.
However, feeling shy, or having a shy personality, is not the same as experiencing social anxiety (short for “social anxiety disorder”).
Here are some of the similarities and differences, and what the distinction means.
pathdoc/Shutterstock How are they similar?
It can be normal to feel nervous or even stressed in new social situations or when interacting with new people. And everyone differs in how comfortable they feel when interacting with others.
For people who are shy or socially anxious, social situations can be very uncomfortable, stressful or even threatening. There can be a strong desire to avoid these situations.
People who are shy or socially anxious may respond with “flight” (by withdrawing from the situation or avoiding it entirely), “freeze” (by detaching themselves or feeling disconnected from their body), or “fawn” (by trying to appease or placate others).
A complex interaction of biological and environmental factors is also thought to influence the development of shyness and social anxiety.
For example, both shy children and adults with social anxiety have neural circuits that respond strongly to stressful social situations, such as being excluded or left out.
People who are shy or socially anxious commonly report physical symptoms of stress in certain situations, or even when anticipating them. These include sweating, blushing, trembling, an increased heart rate or hyperventilation.
How are they different?
Social anxiety is a diagnosable mental health condition and is an example of an anxiety disorder.
For people who struggle with social anxiety, social situations – including social interactions, being observed and performing in front of others – trigger intense fear or anxiety about being judged, criticised or rejected.
To be diagnosed with social anxiety disorder, social anxiety needs to be persistent (lasting more than six months) and have a significant negative impact on important areas of life such as work, school, relationships, and identity or sense of self.
Many adults with social anxiety report feeling shy, timid and lacking in confidence when they were a child. However, not all shy children go on to develop social anxiety. Also, feeling shy does not necessarily mean a person meets the criteria for social anxiety disorder.
People vary in how shy or outgoing they are, depending on where they are, who they are with and how comfortable they feel in the situation. This is particularly true for children, who sometimes appear reserved and shy with strangers and peers, and outgoing with known and trusted adults.
Individual differences in temperament, personality traits, early childhood experiences, family upbringing and environment, and parenting style, can also influence the extent to which people feel shy across social situations.
Not all shy children go on to develop social anxiety. 249 Anurak/Shutterstock However, people with social anxiety have overwhelming fears about embarrassing themselves or being negatively judged by others; they experience these fears consistently and across multiple social situations.
The intensity of this fear or anxiety often leads people to avoid situations. If avoiding a situation is not possible, they may engage in safety behaviours, such as looking at their phone, wearing sunglasses or rehearsing conversation topics.
The effect social anxiety can have on a person’s life can be far-reaching. It may include low self-esteem, breakdown of friendships or romantic relationships, difficulties pursuing and progressing in a career, and dropping out of study.
The impact this has on a person’s ability to lead a meaningful and fulfilling life, and the distress this causes, differentiates social anxiety from shyness.
Children can show similar signs or symptoms of social anxiety to adults. But they may also feel upset and teary, irritable, have temper tantrums, cling to their parents, or refuse to speak in certain situations.
If left untreated, social anxiety can set children and young people up for a future of missed opportunities, so early intervention is key. With professional and parental support, patience and guidance, children can be taught strategies to overcome social anxiety.
Why does the distinction matter?
Social anxiety disorder is a mental health condition that persists for people who do not receive adequate support or treatment.
Without treatment, it can lead to difficulties in education and at work, and in developing meaningful relationships.
Receiving a diagnosis of social anxiety disorder can be validating for some people as it recognises the level of distress and that its impact is more intense than shyness.
A diagnosis can also be an important first step in accessing appropriate, evidence-based treatment.
Different people have different support needs. However, clinical practice guidelines recommend cognitive-behavioural therapy (a kind of psychological therapy that teaches people practical coping skills). This is often used with exposure therapy (a kind of psychological therapy that helps people face their fears by breaking them down into a series of step-by-step activities). This combination is effective in-person, online and in brief treatments.
Treatment is available online as well as in-person. ImYanis/Shutterstock For more support or further reading
Online resources about social anxiety include:
- This Way Up’s online program for managing excessive shyness and fear of social situations
- Beyond Blue’s resources on social anxiety
- a guide to looking after yourself if you have social anxiety, from the Western Australian health department
- social anxiety online program for children and teens from the University of Queensland
- inroads, a self-guided online program for young adults who drink alcohol to manage their anxiety.
We thank the Black Dog Institute Lived Experience Advisory Network members for providing feedback and input for this article and our research.
Kayla Steele, Postdoctoral research fellow and clinical psychologist, UNSW Sydney and Jill Newby, Professor, NHMRC Emerging Leader & Clinical Psychologist, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: