What are ‘Ozempic babies’? Can the drug really increase your chance of pregnancy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hundreds of thousands of people worldwide are taking drugs like Ozempic to lose weight. But what do we actually know about them? This month, The Conversation’s experts explore their rise, impact and potential consequences.
We’ve heard a lot about the impacts of Ozempic recently, from rapid weight loss and lowered blood pressure, to persistent vomiting and “Ozempic face”.
Now we’re seeing a rise in stories about “Ozempic babies”, where women who use drugs like Ozempic (semaglutide) report unexpected pregnancies.
But does semaglutide (also sold as Wegovy) improve fertility? And if so, how? Here’s what we know so far.
Remind me, what is Ozempic?
Ozempic and related drugs (glucagon-like peptide-1 receptor agonists or GLP-1-RAs) were developed to help control blood glucose levels in people with type 2 diabetes.
But the reason for Ozempic’s huge popularity worldwide is that it promotes weight loss by slowing stomach emptying and reducing appetite.
Ozempic is prescribed in Australia as a diabetes treatment. It’s not currently approved to treat obesity but some doctors prescribe it “off label” to help people lose weight. Wegovy (a higher dose of semaglutide) is approved for use in Australia to treat obesity but it’s not yet available.
How does obesity affect fertility?
Obesity affects the fine-tuned hormonal balance that regulates the menstrual cycle.
Women with a body mass index (BMI) above 27 are three times more likely than women in the normal weight range to be unable to conceive because they are less likely to ovulate.
The metabolic conditions of type 2 diabetes and polycystic ovary syndrome (PCOS) are both linked to obesity and fertility difficulties.
Women with type 2 diabetes are more likely than other women to have obesity and to experience fertility difficulties and miscarriage.
Similarly, women with PCOS are more likely to have obesity and trouble conceiving than other women because of hormonal imbalances that cause irregular menstrual cycles.
In men, obesity, diabetes and metabolic syndrome (a cluster of conditions that increase the risk of heart disease and stroke) have negative effects on fertility.
Low testosterone levels caused by obesity or type 2 diabetes can affect the quality of sperm.
So how might Ozempic affect fertility?
Weight loss is recommended for people with obesity to reduce the risk of health problems. As weight loss can improve menstrual irregularities, it may also increase the chance of pregnancy in women with obesity.
This is why weight loss and metabolic improvement are the most likely reasons why women who use Ozempic report unexpected pregnancies.
But unexpected pregnancies have also been reported by women who use Ozempic and the contraceptive pill. This has led some experts to suggest that some GLP-1-RAs might affect the absorption of the pill and make it less effective. However, it’s uncertain whether there is a connection between Ozempic and contraceptive failure.

In men with type 2 diabetes, obesity and low testosterone, drugs like Ozempic have shown promising results for weight loss and increasing testosterone levels.
Avoid Ozempic if you’re trying to conceive
It’s unclear if semaglutide can be harmful in pregnancy. But data from animal studies suggest it should not be used in pregnancy due to potential risks of fetal abnormalities.
That’s why the Therapeutic Goods Administration recommends women of childbearing potential use contraception when taking semaglutide.
Similarly, PCOS guidelines state health professionals should ensure women with PCOS who use Ozempic have effective contraception.
Guidelines recommended stopping semaglutide at least two months before planning pregnancy.
For women who use Ozempic to manage diabetes, it’s important to seek advice on other options to control blood glucose levels when trying for pregnancy.
What if you get pregnant while taking Ozempic?
For those who conceive while using Ozempic, deciding what to do can be difficult. This decision may be even more complicated considering the unknown potential effects of the drug on the fetus.
While there is little scientific data available, the findings of an observational study of pregnant women with type 2 diabetes who were on diabetes medication, including GLP-1-RAs, are reassuring. This study did not indicate a large increased risk of major congenital malformations in the babies born.
Women considering or currently using semaglutide before, during, or after pregnancy should consult with a health provider about how to best manage their condition.
When pregnancies are planned, women can take steps to improve their baby’s health, such as taking folic acid before conception to reduce the risk of neural tube defects, and stopping smoking and consuming alcohol.
While unexpected pregnancies and “Ozempic babies” may be welcomed, their mothers have not had the opportunity to take these steps and give them the best start in life.
Read the other articles in The Conversation’s Ozempic series here.
Karin Hammarberg, Senior Research Fellow, Global and Women’s Health, School of Public Health & Preventive Medicine, Monash University and Robert Norman, Emeritus Professor of Reproductive and Periconceptual Medicine, The Robinson Research Institute, University of Adelaide
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Small Pleasures – by Ryan Riley

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Hippocrates said “let food be thy medicine, and let medicine be thy food”, he may or may not have had this book in mind.
In terms of healthiness, this one’s not the very most nutritionist-approved recipe book we’ve ever reviewed. It’s not bad, to be clear!
But the physical health aspect is secondary to the mental health aspects, in this one, as you’ll see. And as we say, “mental health is also just health”.
The book is divided into three sections:
- Comfort—for when you feel at your worst, for when eating is a chore, for when something familiar and reassuring will bring you solace. Here we find flavor and simplicity; pastas, eggs, stews, potato dishes, and the like.
- Restoration—for when your energy needs reawakening. Here we find flavors fresh and tangy, enlivening and bright. Things to make you feel alive.
- Pleasure—while there’s little in the way of health-food here, the author describes the dishes in this section as “a love letter to yourself; they tell you that you’re special as you ready yourself to return to the world”.
And sometimes, just sometimes, we probably all need a little of that.
Bottom line: if you’d like to bring a little more joie de vivre to your cuisine, this book can do that.
Click here to check out Small Pleasures, and rekindle joy in your kitchen!
Share This Post
-

The Squat Bible – by Dr. Aaron Horschig
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You probably know the following three things about squats:
- Squatting is great for the health in many ways
- There are many different ways to squat
- Not all of them are correct, and some may even do harm
Dr. Aaron Horschig makes the case for squats being a movement first, and an exercise second. To this end, he takes us on a joint-by-joint tour of the anatomy of squatting, so that we get it right from top to toe.
Or rather: from toe to top, since he starts with the best foundation.
What this means is that if you’ve struggled to squat because you find some discomfort in your ankles, or a weakness in the knees, or you can’t get your back quite right, Dr. Horschig will have a fix for you. He also takes a realistic look about how people’s anatomy varies from person to person, and what differences this makes to how we each should best squat.
The explanations are clear and so are the pictures—we recommend getting the color print edition (linked), as the image quality is better than the black and white and/or Kindle edition.
Bottom-line: squats are one of the single best exercises we can do for our health—but we can miss out on benefits (or even do ourselves harm) if we don’t do them well. This book is a comprehensive reference resource for making sure we get the most out of our squatting ability.
Click here to check out The Squat Bible, and master this all-important movement!
Share This Post
-

Why is toddler milk so popular? Follow the money
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Toddler milk is popular and becoming more so. Just over a third of Australian toddlers drink it. Parents spend hundreds of millions of dollars on it globally. Around the world, toddler milk makes up nearly half of total formula milk sales, with a 200% growth since 2005. Growth is expected to continue.
We’re concerned about the growing popularity of toddler milk – about its nutritional content, cost, how it’s marketed, and about the impact on the health and feeding of young children. Some of us voiced our concerns on the ABC’s 7.30 program recently.
But what’s in toddler milk? How does it compare to cow’s milk? How did it become so popular?
What is toddler milk? Is it healthy?
Toddler milk is marketed as appropriate for children aged one to three years. This ultra-processed food contains:
- skim milk powder (cow, soy or goat)
- vegetable oil
- sugars (including added sugars)
- emulsifiers (to help bind the ingredients and improve the texture)
added vitamins and minerals.
Toddler milk is usually lower in calcium and protein, and higher in sugar and calories than regular cow’s milk. Depending on the brand, a serve of toddler milk can contain as much sugar as a soft drink.
Even though toddler milks have added vitamins and minerals, these are found in and better absorbed from regular foods and breastmilk. Toddlers do not need the level of nutrients found in these products if they are eating a varied diet.
Global health authorities, including the World Health Organization (WHO), and Australia’s National Health and Medical Research Council, do not recommend toddler milk for healthy toddlers.
Some children with specific metabolic or dietary medical problems might need tailored alternatives to cow’s milk. However, these products generally are not toddler milks and would be a specific product prescribed by a health-care provider.
Toddler milk is also up to four to five times more expensive than regular cow’s milk. “Premium” toddler milk (the same product, with higher levels of vitamins and minerals) is more expensive.
With the cost-of-living crisis, this means families might choose to go without other essentials to afford toddler milk.

Toddler milk is more expensive than cow’s milk and contains more sugar.
Dragana Gordic/ShutterstockHow toddler milk was invented
Toddler milk was created so infant formula companies could get around rules preventing them from advertising their infant formula.
When manufacturers claim benefits of their toddler milk, many parents assume these claimed benefits apply to infant formula (known as cross-promotion). In other words, marketing toddler milks also boosts interest in their infant formula.
Manufacturers also create brand loyalty and recognition by making the labels of their toddler milk look similar to their infant formula. For parents who used infant formula, toddler milk is positioned as the next stage in feeding.
How toddler milk became so popular
Toddler milk is heavily marketed. Parents are told toddler milk is healthy and provides extra nutrition. Marketing tells parents it will benefit their child’s growth and development, their brain function and their immune system.
Toddler milk is also presented as a solution to fussy eating, which is common in toddlers.
However, regularly drinking toddler milk could increase the risk of fussiness as it reduces opportunities for toddlers to try new foods. It’s also sweet, needs no chewing, and essentially displaces energy and nutrients that whole foods provide.
Toddler milk is said to help fussy eating, but it may make things worse.
zlikovec/ShutterstockGrowing concern
The WHO, along with public health academics, has been raising concerns about the marketing of toddler milk for years.
In Australia, moves to curb how toddler milk is promoted have gone nowhere. Toddler milk is in a category of foods that are allowed to be fortified (to have vitamins and minerals added), with no marketing restrictions. The Australian Competition & Consumer Commission also has concerns about the rise of toddler milk marketing. Despite this, there is no change in how it’s regulated.
This is in contrast to voluntary marketing restrictions in Australia for infant formula.
What needs to happen?
There is enough evidence to show the marketing of commercial milk formula, including toddler milk, influences parents and undermines child health.
So governments need to act to protect parents from this marketing, and to put child health over profits.
Public health authorities and advocates, including us, are calling for the restriction of marketing (not selling) of all formula products for infants and toddlers from birth through to age three years.
Ideally, this would be mandatory, government-enforced marketing restrictions as opposed to industry self-regulation in place currently for infant formulas.
We musn’t blame parents
Toddlers are eating more processed foods (including toddler milk) than ever because time-poor parents are seeking a convenient option to ensure their child is getting adequate nutrition.
Formula manufacturers have used this information, and created a demand for an unnecessary product.
Parents want to do the best for their toddlers, but they need to know the marketing behind toddler milks is misleading.
Toddler milk is an unnecessary, unhealthy, expensive product. Toddlers just need whole foods and breastmilk, and/or cow’s milk or a non-dairy, milk alternative.
If parents are worried about their child’s eating, they should see a health-care professional.
Anthea Rhodes, a paediatrician from Royal Children’s Hospital Melbourne and a lecturer at the University of Melbourne, co-authored this article.

Jennifer McCann, Lecturer Nutrition Sciences, Institute for Physical Activity and Nutrition, Deakin University; Karleen Gribble, Adjunct Associate Professor, School of Nursing and Midwifery, Western Sydney University, and Naomi Hull, PhD candidate, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-

The Five Invitations – by Frank Ostaseski
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book covers exactly what its subtitle promises, and encourages the reader to truly live life fully, something that Ostaseski believes cannot be done in ignorance of death.
Instead, he argues from his experience of decades working at a hospice, we must be mindful of death not only to appreciate life, but also to make the right decisions in life—which means responding well to what he calls, as per the title of this book, “the five invitations”.
We will not keep them a mystery; they are:
- Don’t wait; do the important things now
- Welcome everything; push away nothing
- Bring your whole self to the experience
- Find a place in the middle of things
- Cultivate a “don’t know” mind
Note, for example, that “do the important things now” requires knowing what is important. For example, ensuring a loved one knows how you feel about them, might be more important than scratching some item off a bucket list. And “push away nothing” does mean bad things too; rather, of course try to make life better rather than worse, but accept the lessons and learnings of the bad too, and see the beauty that can be found in contrast to it. Enjoying the fullness of life without getting lost in it; carrying consciousness through the highs and lows. And yes, approaching the unknown (which means not only death, but also the large majority of life) with open-minded curiosity and wonder.
The style of the book is narrative and personal, without feeling like a collection of anecdotes, but rather, taking the reader on a journey, prompting reflection and introspection along the way.
Bottom line: if you’d like to minimize the regrets you have in life, this book is a fine choice.
Click here to check out The Five Invitations, and answer with a “yes” to the call of life!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What does lion’s mane mushroom actually do, anyway?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may know it as an ingredient in nootropic supplements. You may have heard of lion’s mane mushroom coffee. You may know it as the big shaggy white mushroom that grows in nature and can look very impressive.
What’s special about it?
The lion’s mane mushroom, or Hericium erinaceus (we mention, as studies we’ll cite often use the botanical name) is an adaptogenic agent that has an established ability to promote nerve regeneration through nerve growth factor neurotrophic activity. In other words, it helps (re)grow neurons.
In a 2023 study, researchers wondered if its abilities (well-established in the peripheral nervous system) would work in the central nervous system too, namely the brain, specifically the hippocampus (responsible for memory).
To boil what they found down to a single line, they concluded:
❝[Lion’s mane extract] therefore acts through a novel pan-neurotrophic signaling pathway, leading to improved cognitive performance.❞
You can read the full study for yourself (with pictures!) here:
Limitations of the study
It’s worth noting that the above study was performed on mice brains, not those of humans. As there is a shortage of human volunteers willing to have their brains sliced and examined under microscopes, we do not expect this study to be repeated with humans any time soon.
So, are there human studies that have been done?
There are! Particularly promising was this 2020 study of people with Alzheimer’s disease, wherein supplementation with 1g of lion’s mane mushroom daily for 49 weeks significantly increased cognitive test scores compared with a placebo; you can read about it here:
Additionally, this 2019 study showed that taking 1.2g daily for eight weeks helped relieve depression, anxiety, and sleep disorders in overweight or obese patiences:
Are there other health benefits?
It seems so! Unfortunately, most of its other health claims are only supported by animal studies so far, aside from one small study funded by a supplement company for their supplement that contained mostly Agaricus blazei (a different mushroom) with 14% lion’s mane.
However, in animal studies, lion’s mane has also shown promise:
- For digestion
- Against inflammation
- For cardiovascular health
- For diabetes management
- Against cancer
- Against aging
Where can I get it?
We don’t sell it (or anything else, for that matter) but if you’d like to try it, here’s an example product for your convenience:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Mythbusting Cookware Materials
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

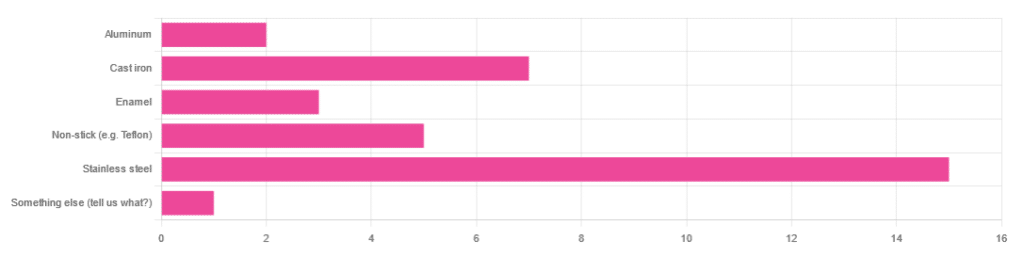
In Wednesday’s newsletter, we asked you what kind of cookware you mostly use, and got the above-depicted, below-described, set of responses:
- About 45% said stainless steel
- About 21% said cast iron
- About 15% said non-stick (e.g. Teflon)
- About 9% said enamel
- About 6% said aluminum
- And 1 person selected “something else”, but then commented to the contrary, writing “I use all of the above”
So, what does the science say about these options?
Stainless steel cookware is safe: True or False?
True! Assuming good quality and normal use, anyway. There really isn’t a lot to say about this, because it’s very unexciting. So long as it is what it is labelled as: there’s nothing coating it, nothing comes out of it unless you go to extremes*, and it’s easy to clean.
*If you cook for long durations at very high temperatures, it can leach nickel and chromium into food. What this means in practical terms: if you are using stainless steel to do deep-frying, then maybe stop that, and also consider going easy on deep-frying in general anyway, because obviously deep-frying is unhealthy for other reasons.
Per normal use, however: pretty much the only way (good quality) stainless steel cookware will harm you is if you touch it while it’s hot, or if it falls off a shelf onto your head.
That said, do watch out for cheap stainless steel cookware that can contain a lot of impurities, including heavy metals. Since you probably don’t have a mass spectrometer and/or chemistry lab at home to check for those impurities, your best guard here is simply to buy from a reputable brand with credible certifications.
Ceramic cookware is safe: True or False?
True… Most of the time! Ceramic pans usually have metal parts and a ceramic cooking surface coated with a very thin layer of silicon. Those metal parts will be as safe as the metals used, so if that’s stainless steel, you’re just as safe as the above. As for the silicon, it is famously inert and body-safe (which is why it’s used in body implants).
However: ceramic cookware that doesn’t have an obvious metal part and is marketed as being pure ceramic, will generally be sealed with some kind of glaze that can leach heavy metals contaminants into the food; here’s an example:
Lead toxicity from glazed ceramic cookware
Copper cookware is safe: True or False?
False! This is one we forgot to mention in the poll, as one doesn’t see a lot of it nowadays. The copper from copper pans can leach into food. Now, of course copper is an important mineral that we must get from our diet, but the amount of copper that that can leach into food from copper pans is far too much, and can induce copper toxicity.
In addition, copper cookware has been found to be, on average, highly contaminated with lead:
Non-stick cookware contaminates the food with microplastics: True or False?
True! If we were to discuss all the common non-stick contaminants here, this email would no longer fit (there’s a size limit before it gets clipped by most email services).
Suffice it to say: the non-stick coating, polytetrafluoroethylene, is itself a PFAS, that is to say, part of the category of chemicals considered environmental pollutants, and associated with a long list of health issues in humans (wherein the level of PFAS in our bloodstream is associated with higher incidence of many illnesses):
You may have noticed, of course, that the “non-stick” coating doesn’t stick very well to the pan, either, and will tend to come off over time, even if used carefully.
Also, any kind of wet cooking (e.g. saucepans, skillets, rice cooker inserts) will leach PFAS into the food. In contrast, a non-stick baking tray lined with baking paper (thus: a barrier between the tray and your food) is really not such an issue.
We wrote about PFAS before, so if you’d like a more readable pop-science article than the scientific paper above, then check out:
PFAS Exposure & Cancer: The Numbers Are High
Aluminum cookware contaminates the food with aluminum: True or False?
True! But not usually in sufficient quantities to induce aluminum toxicity, unless you are aluminum pans Georg who eats half a gram of aluminum per day, who is a statistical outlier and should not be counted.
That’s a silly example, but an actual number; the dose required for aluminum toxicity in blood is 100mg/L, and you have about 5 liters of blood.
Unless you are on kidney dialysis (because 95% of aluminum is excreted by the kidneys, and kidney dialysis solution can itself contain aluminum), you will excrete aluminum a lot faster than you can possibly absorb it from cookware. On the other hand, you can get too much of it from it being a permitted additive in foods and medications, for example if you are taking antacids they often have a lot of aluminum oxide in them—but that is outside the scope of today’s article.
However, aluminum may not be the real problem in aluminum pans:
❝In addition, aluminum (3.2 ± 0.25 to 4.64 ± 0.20 g/kg) and copper cookware (2.90 ± 0.12 g/kg) were highly contaminated with lead.
The time and pH-dependent study revealed that leaching of metals (Al, Pb, Ni, Cr, Cd, Cu, and Fe, etc.) into food was predominantly from anodized and non-anodized aluminum cookware.
More metal leaching was observed from new aluminum cookware compared to old. Acidic food was found to cause more metals to leach during cooking.❞
~ the same paper we cited when talking about copper
Cast iron cookware contaminates the food with iron: True or False?
True, but unlike with the other metals discussed, this is purely a positive, and indeed, it’s even recommended as a good way to fortify one’s diet with iron:
The only notable counterpoint we could find for this is if you have hemochromatosis, a disorder in which the body is too good at absorbing iron and holding onto it.
Thinking of getting some new cookware?
Here are some example products of high-quality safe materials on Amazon, but of course feel free to shop around:
Stainless Steel | Ceramic* | Cast Iron
*it says “non-stick” in the description, but don’t worry, it’s ceramic, not Teflon etc, and is safe
Bonus: rice cooker with stainless steel inner pot
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: