Want the health benefits of strength training but not keen on the gym? Try ‘exercise snacking’
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The science is clear: resistance training is crucial to ageing well. Lifting weights (or doing bodyweight exercises like lunges, squats or push-ups) can help you live independently for longer, make your bones stronger, reduce your risk of diseases such as diabetes, and may even improve your sleep and mental health.
But not everyone loves the gym. Perhaps you feel you’re not a “gym person” and never will be, or you’re too old to start. Being a gym-goer can be expensive and time-consuming, and some people report feeling unwelcome or awkward at the gym.
The good news is you don’t need the gym, or lots of free time, to get the health benefits resistance training can offer.
You can try “exercise snacking” instead.

What is exercise snacking?
Exercise snacking involves doing multiple shorter bouts (as little as 20 seconds) of exercise throughout the day – often with minimal or no equipment. It’s OK to have several hours of rest between.
You could do simple bodyweight exercises such as:
- chair sit-to-stand (squats)
- lunges
- box step-ups
- calf raises
- push-ups.
Exercise snacking like this can help improve muscle mass, strength and physical function.
It’s OK to hold onto a nearby object for balance, if you need. And doing these exercises regularly will also improve your balance. That, in turn, reduces your risk of falls and fractures.
OK I have done all those, now what?
Great! You can also try using resistance bands or dumbbells to do the previously mentioned five exercises as well as some of the following exercises:
When using resistance bands, make sure you hold them tightly and that they’re securely attached to an immovable object.
Exercise snacking works well when you pair it with an activity you do often throughout the day. Perhaps you could:
- do a few extra squats every time you get up from a bed or chair
- do some lunges during a TV ad break
- chuck in a few half squats while you’re waiting for your kettle to boil
- do a couple of elevated push-ups (where you support your body with your hands on a chair or a bench while doing the push-up) before tucking into lunch
- sneak in a couple of calf raises while you’re brushing your teeth.

What does the evidence say about exercise snacking?
One study had older adults without a history of resistance training do exercise snacks at home twice per day for four weeks.
Each session involved five simple bodyweight exercises (chair sit-to-stand, seated knee extension, standing knee bends, marching on the spot, and standing calf raises). The participants did each exercise continuously for one minute, with a one-minute break between exercises.
These short and simple exercise sessions, which lasted just nine minutes, were enough to improve a person’s ability to stand up from a chair by 31% after four weeks (compared to a control group who didn’t exercise). Leg power and thigh muscle size improved, too.
Research involving one of us (Jackson Fyfe) has also shown older adults found “exercise snacking” feasible and enjoyable when done at home either once, twice, or three times per day for four weeks.
Exercise snacking may be a more sustainable approach to improve muscle health in those who don’t want to – or can’t – lift heavier weights in a gym.
A little can yield a lot
We know from other research that the more you exercise, the more likely it is you will keep exercising in future.
Very brief resistance training, albeit with heavier weights, may be more enjoyable than traditional approaches where people aim to do many, many sets.
We also know brief-and-frequent exercise sessions can break up periods of sedentary behaviour (which usually means sitting too much). Too much sitting increases your risk of chronic diseases such as diabetes, whereas exercise snacking can help keep your blood sugar levels steady.
Of course, longer-term studies are needed. But the evidence we do have suggests exercise snacking really helps.

Why does any of this matter?
As you age, you lose strength and mass in the muscles you use to walk, or stand up. Everyday tasks can become a struggle.
All this contributes to disability, hospitalisation, chronic disease, and reliance on community and residential aged care support.
By preserving your muscle mass and strength, you can:
- reduce joint pain
- get on with activities you enjoy
- live independently in your own home
- delay or even eliminate the need for expensive health care or residential aged care.
What if I walk a lot – is that enough?
Walking may maintain some level of lower body muscle mass, but it won’t preserve your upper body muscles.
If you find it difficult to get out of a chair, or can only walk short distances without getting out of breath, resistance training is the best way to regain some of the independence and function you’ve lost.
It’s even more important for women, as muscle mass and strength are typically lower in older women than men. And if you’ve been diagnosed with osteoporosis, which is more common in older women than men, resistance exercise snacking at home can improve your balance, strength, and bone mineral density. All of this reduces the risk of falls and fractures.
You don’t need heavy weights or fancy equipment to benefit from resistance training.
So, will you start exercise snacking today?
Justin Keogh, Associate Dean of Research, Faculty of Health Sciences and Medicine, Bond University and Jackson Fyfe, Senior Lecturer, Strength and Conditioning Sciences, Deakin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Beetroot Benefits That Depend On Your Age

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve written before about beetroot’s considerable health benefits: Beetroot For More Than Just Your Blood Pressure
We even covered how to make it better in a surprising way: Beetroot Juice & Caffeine Work Better Than Either Alone
But what’s this about age differences?
Different for younger and older people
Researchers (Dr. Anni Vanhatalo et al.) investigated this, and wondered how much of beetroot’s beneficial effect is due to boosting nitric oxide (NO) production, something that aging typically reduces, but that nitrate-rich beetroot improves.
To test this, they did a randomized, placebo-controlled, double-blind crossover trial with young adults (18–30) and older adults (67–79). They excluded participants with cardiovascular, metabolic, pulmonary, or oral disease; smokers; anyone with high blood pressure (here defined as >140/90, notwithstanding that the usual standard is >130/90), and anyone who had recently used antibiotics.
The interventions were:
- nitrate-rich beetroot juice (2 × 70 ml/day, ~595 mg nitrate each)
- nitrate-depleted beetroot juice (same quantity of juice, no nitrate, functioning as placebo)
- antiseptic mouthwash (because they suspected that oral bacteria played a role)
These they tested with two-week treatment phases, with washout periods between (since the groups switched roles, being as it was a crossover trial, it was important to ensure that each group was not still being affected by the previous intervention).
What they measured: they did tongue swabs for microbiome sequencing, they checked plasma nitrate/nitrite for NO bioavailability, they also recorded blood pressure (brachial and central), endothelial function (flow-mediated dilation), and arterial stiffness.
What they found:
- Endothelial function and arterial stiffness remained unchanged in all groups. It seems this is simply not something that beetroot juice affects.
- The older adults had higher baseline blood pressure, and/but nitrate-rich beetroot juice lowered brachial mean arterial pressure in older adults while it had no significant effect in younger adults.
- In the category of oral microbiome changes, they found that in older adults, beetroot juice reduced Prevotella-dominated bacterial linked with DNRA (which diverts nitrite away from NO production), and that reduction in Prevotella correlated with higher plasma nitrite and lower blood pressure; nitrate-rich beetroot juice increased nitrate-reducing genera Neisseria and Rothia, especially in older adults, having only modest benefits for younger adults. Antiseptic mouthwash reduced microbial diversity (shocking nobody) and impaired vascular function.
- Nitrate-depleted juice still raised plasma nitrate/nitrite modestly and had a small lowering effect on blood pressure in older adults. This may have been because of:
- placebo effect doing its thing
- imperfect depletion of nitrates
- other unknown factors
- a combination of the above
In summary: in older adults, beetroot juice improves the oral microbiome and, partly because of that, lowers blood pressure. Younger adults get only marginal benefits at best, and use of antiseptic mouthwash completely wipes out the benefits.
You can read the paper itself, here: Ageing modifies the oral microbiome, nitric oxide bioavailability and vascular responses to dietary nitrate supplementation
Before you get juicing, there are some things you should be aware of: 3 Day Juice Fasting? Not So Fast! ← this isn’t even just about the glycemic index issue (juices being stripped of fiber), and is rather mostly about the microbiome problems juices can cause without sufficient dietary fiber (so, not so much a problem if, for example, you have a juice after a fibrous meal).
Not a fan of juices? This writer doesn’t love juices most of the time either, but we can enjoy: Hearty Healthy Ukrainian Borscht ← from our recipes archive!
Remember when…
…we talked about Dr. Ellie Phillips’ advices with regard to oral health?
In few words, Dr. Phillips promotes protecting oral microbial diversity by avoiding antibacterial mouthwashes; the study we talked about today also validated that, showing how antiseptic mouthwash (unsurprisingly) reduced microbial diversity and (importantly and relevantly) impaired vascular function.
Now, she often points to imbalances where certain bacteria overgrow; this study showed Prevotella dominance (i.e., harmful bacteria being too plentiful) diverts nitrite away from NO production, worsening cardiovascular function—a good example of how oral imbalances have systemic effects.
So, how to kill the bad bacteria without harming the good ones? Critically, diet can feed the protective oral bacteria; here, nitrate-rich beetroot juice improved blood pressure by shifting the oral microbiome towards beneficial nitrate-reducing genera (e.g. the Neisseria and Rothia in this study). As for the rest, Dr. Phillips advocates simple, natural methods (xylitol, remineralizing foods, protective rinses) instead of harsh chemicals. As we’ve learned today, dietary strategies (like beetroot juice) can also play their part as a natural, safe way to help your oral microbiome to help you.
For research on this by a third source, see: Make Your Saliva Better For Your Health
Want to learn more?
With regard to nitrates and health, you might like:
The Nitric Oxide (NO) Solution – by Dr. Nathan Bryan & Janet Zand
…and, with a focus on beets (roots and leaves):
Beet The Odds – by Dr. Nathan Bryan & Carolyn Pierini
Enjoy!
Share This Post
-

The Good Life – by Robert Waldinger, MD, and Marc Schulz, PhD
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For any who have thought “there must be some middle-ground between entirely subjective self-help books advising how to feel better, and sifting through clinical data on what actually affects people’s moods“, this book is exactly that middle-ground!
Drs. Waldinger and Schultz went through the 80-year-long Harvard Study of Adult Development with a fine-toothed comb, and this book details—more readably—what they found.
There are frequent references to data from the study. Not just numbers, though, people’s answers to questions, too. And how different factors about people’s lives affected their answers to the same questions.
We hear from all ages, from young adults to octagenarians, and learn how attitudes (including: of the same people) change over time. Not because people are fickle, but because people grow… or become disillusioned. Or sometimes, both.
We learn about the importance of money… And where that importance ends.
We learn importance of relationships of various kinds, and this is certainly a recurring theme throughout the study—and thus, throughout the book.
The book doesn’t just present data, though, it also presents actionable insights along the way.
Bottom line: the combined wisdom and life-experiences of a lot of people provide a very “big picture” view of life, and what makes us happy, really. We highly recommend it!
Share This Post
-

Body on Fire – by Dr. Monica Aggarwal and Dr. Jyothi Rao
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are times when you do really need a doctor, not a dietician. But there are also times when a doctor will prescribe something for the symptom, leaving the underlying issue untouched. If only there were a way to have the best of both worlds!
That’s where Drs. Rao and Aggarwal come in. They’re both medical doctors… with a keen interest in nutrition and healthy lifestyle changes to make us less sick such that we have less need to go to the doctor at all.
Best of all, they understand—while some things are true for everyone—there’s not a one-size-fits all diet or exercise regime or even sleep setup.
So instead, they take us hand-in-hand (chapter by chapter!) through the various parts of our life (including our diet) that might need tweaking. Each of these changes, if taken up, promise a net improvement that becomes synergistic with the other changes. There’s a degree of biofeedback involved, and listening to your body, to be sure of what’s really best for you, not what merely should be best for you on paper.
The writing style is accessible while science-heavy. They don’t assume prior knowledge, and/but they sure deliver a lot. The book is more text than images, but there are plenty of medical diagrams, explanations, charts, and the like. You will feed like a medical student! And it’s very much worth studying.
Bottom line: highly recommendable even if you don’t have inflammation issues, and worth its weight in gold if you do.
Share This Post

Related Posts
-

Optimism Seriously Increases Longevity!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Always look on the bright side for life
❝I’m not a pessimist; I’m a realist!❞
~ every pessimist ever
To believe self-reports, the world is divided between optimists and realists. But how does your outlook measure up, really?
Below, we’ve included a link to a test, and like most free online tests, this is offered “as-is” with the usual caveats about not being a clinical diagnostic tool, this one actually has a fair amount of scientific weight behind it:
❝Empirical testing has indicated the validity of the Optimism Pessimism Instrument as published in the scientific journal Current Psychology: Research and Reviews.
The IDRlabs Optimism/Pessimism Test (IDR-OPT) was developed by IDRlabs. The IDR-OPT is based on the Optimism/Pessimism Instrument (OPI) developed by Dr. William Dember, Dr. Stephanie Martin, Dr. Mary Hummer, Dr. Steven Howe, and Dr. Richard Melton, at the University of Cincinnati.❞
Take This Short (1–2 mins) Test
How did you score? And what could you do to improve on that score?
We said before that we’d do a main feature on this sometime, and today’s the day! Fits with the theme of Easter too, as for those who observe, this is a time for a celebration of hope, new beginnings, and life stepping out of the shadows.
On which note, before we go any further, let’s look at a very big “why” of optimism…
There have been many studies done regards optimism and health, and they generally come to the same conclusion: optimism is simply good for the health.
Here’s an example. It’s a longitudinal study, and it followed 121,700 women (what a sample size!) for eight years. It controlled for all kinds of other lifestyle factors (especially smoking, drinking, diet, and exercise habits, as well as pre-existing medical conditions), so this wasn’t a case of “people who are healthy are more optimistic as a result. And, in the researchers’ own words…
❝We found strong and statistically significant associations of increasing levels of optimism with decreasing risks of mortality, including mortality due each major cause of death, such as cancer, heart disease, stroke, respiratory disease, and infection.
Importantly, findings were maintained after close control for potential confounding factors, including sociodemographic characteristics and depression❞
Read: Optimism and Cause-Specific Mortality: A Prospective Cohort Study
So that’s the why. Now for the how…
Positive thinking is not what you think it is
A lot of people think of “think positive thoughts” as a very wishy-washy platitude, but positive thinking isn’t about ignoring what’s wrong, or burying every negative emotion.
Rather, it is taking advantage of the basic CBT, DBT, and, for that matter, NLP principles:
- Our feelings are driven by our thoughts
- Our thoughts can be changed by how we frame things
This is a lot like the idea that “there’s not such thing as bad weather; only the wrong clothes”. Clearly written by someone who’s never been in a hurricane, but by and large, the principle stands true.
For example…
- Most problems can be reframed as opportunities
- Replace “I have to…” with “I get to…”
- Will the task be arduous? It’ll be all the better looking back on it.
- Did you fail abjectly? Be proud that you lived true to your values anyway.
A lot of this is about focusing on what you can control. If you live your life by your values (first figure out what they are, if you haven’t already), then that will become a reassuring thing that you can always count on, no matter what.
Practice positive self-talk (eliminate the negative)
We often learn, usually as children, to be self deprecatory so as to not appear immodest. While modesty certainly has its place, we don’t have to trash ourselves to do that!
There are various approaches to this, for example:
- Replacing a self-criticism (whether it was true or not) with a neutral or positive statement that you know is true. “I suck at xyz” is just putting yourself down, “Xyz is a challenge for me” asks the question, how will you rise to it?
- Replacing a self-criticism with irony. It doesn’t matter how dripping with sarcasm your inner voice is, the words will still be better. “Glamorous as ever!” after accidentally putting mascara in your eye. “So elegant and graceful!” after walking into furniture. And so on.
Practice radical acceptance
This evokes the “optimistic nihilism” approach to life. It’s perhaps not best in all scenarios, but if you’re consciously and rationally pretty sure something is going to be terrible (and/or know it’s completely outside of your control), acknowledging that possibility (or even, likelihood) cheerfully. Borrowing from the last tip, this can be done with as much irony as you find necessary. For example:
Facing a surgery the recovery from which you know categorically will be very painful: with a big smile “Yep, I am going to be in a lot of pain, so that’s going to be fun!” (fun fact: psychological misery will not make the physical pain any less painful, so you might as well see the funny side) ← see link for additional benefits laughter can add to health-related quality of life)
Plan for the future with love
You know the whole “planting trees in whose shade you’ll never sit”, thing, but: actually for yourself too. Plan (and act!) now, out of love and compassion for your future self.
Simple example: preparing (or semi-preparing, if appropriate) breakfast for yourself the night before, when you know in the morning you’ll be tired, hungry, and/or pressed for time. You’ll wake up, remember that you did that, and…
Tip: at moments like that, take a moment to think “Thanks, past me”. (Or call yourself by your name, whatever works for you. For example I, your writer here, might say to myself “Thanks, past Nastja!”)
This helps to build a habit of gratitude for your past self and love for your future self.
This goes for little things like the above, but it also goes for things whereby there’s much longer-term delayed gratification, such as:
- Healthy lifestyle changes (usually these see slow, cumulative progress)
- Good financial strategies (usually these see slow, cumulative progress)
- Long educational courses (usually these see slow, cumulative progress)
Basically: pay it forward to your future self, and thank yourself later!
Some quick ideas of systems and apps that go hard on the “long slow cumulative progress” approach that you can look back on with pride:
- Noom—nutritional program with a psychology-based approach to help you attain and maintain your goals, long term
- You Need A Budget—we’ve recommended it before and we’ll recommend it again. This is so good. If you click through, you can see a short explanation of what makes it so different to other budgeting apps.
- Duolingo—the famously persistence-motivational language learning app
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Brain As A Work-In-Progress
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
And The Brain Goes Marching On!

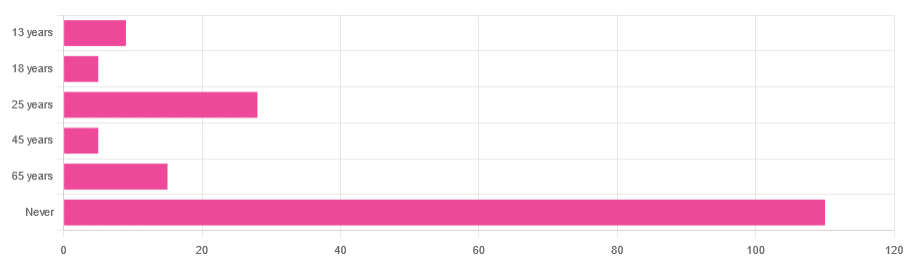
In Tuesday’s newsletter, we asked you “when does the human brain stop developing?” and got the above-depicted, below-described, set of responses:
- About 64% of people said “Never”
- About 16% of people said “25 years”
- About 9% of people said “65 years”
- About 5% of people said “13 years”
- About 3% of people said “18 years”
- About 3% of people said “45 years”
Some thoughts, before we get into the science:
An alternative wording for the original question was “when does the human brain finish developing”; the meaning is the same but the feeling is slightly different:
- “When does the human brain stop developing?” focuses attention on the idea of cessation, and will skew responses to later ages
- When does the human brain finish developing?” focuses on attention on a kind of “is it done yet?” and will skew responses to earlier ages
Ultimately, since we had to chose one word or another, we picked the shortest one, but it would have been interesting if we could have done an A/B test, and asked half one way, and half the other way!
Why we picked those ages
We picked those ages as poll options for reasons people might be drawn to them:
- 13 years: in English-speaking cultures, an important milestone of entering adolescence (note that the concept of a “teenager” is not precisely universal as most languages do not have “-teen” numbers in the same way; the concept of “adolescent” may thus be tied to other milestones)
- 18 years: age of legal majority in N. America and many other places
- 25 years: age popularly believed to be when the brain is finished developing, due to a study that we’ll talk about shortly (we guess that’s why there’s a spike in our results for this, too!)
- 45 years: age where many midlife hormonal changes occur, and many professionals are considered to have peaked in competence and start looking towards retirement
- 65 years: age considered “senior” in much of N. America and many other places, as well as the cut-off and/or starting point for a lot of medical research
Notice, therefore, how a lot of things are coming from places they really shouldn’t. For example, because there are many studies saying “n% of people over 65 get Alzheimer’s” or “n% of people over 65 get age-related cognitive decline”, etc, 65 becomes the age where we start expecting this—because of an arbitrary human choice of where to draw the cut-off for the study enrollment!
Similarly, we may look at common ages of legal majority, or retirement pensions, and assume “well it must be for a good reason”, and dear reader, those reasons are more often economically motivated than they are biologically reasoned.
So, what does the science say?
Our brains are never finished developing: True or False?
True! If we define “finished developing” as “we cease doing neurogenesis and neuroplasticity is no longer in effect”.
Glossary:
- Neurogenesis: the process of creating new brain cells
- Neuroplasticity: the process of the brain adapting to changes by essentially rebuilding itself to suit our perceived current needs
We say “perceived” because sometimes neuroplasticity can do very unhelpful things to us (e.g: psychological trauma, or even just bad habits), but on a biological level, it is always doing its best to serve our overall success as an organism.
For a long time it was thought that we don’t do neurogenesis at all as adults, but this was found to be untrue:
How To Grow New Brain Cells (At Any Age)
Summary of conclusions of the above: we’re all growing new brain cells at every age, even if we be in our 80s and with Alzheimer’s disease, but there are things we can do to enhance our neurogenic potential along the way.
Neuroplasticity will always be somewhat enhanced by neurogenesis (after all, new neurons get given jobs to do), and we reviewed a great book about the marvels of neuroplasticity including in older age:
Our brains are still developing up to the age of 25: True or False?
True! And then it keeps on developing after that, too. Now this is abundantly obvious considering what we just talked about, but see what a difference the phrasing makes? Now it makes it sound like it stops at 25, which this statement doesn’t claim at all—it only speaks for the time up to that age.
A lot of the popular press about “the brain isn’t fully mature until the age of 25” stems from a 2006 study that found:
❝For instance, frontal gray matter volume peaks at about age 11.0 years in girls and 12.1 years in boys, whereas temporal gray matter volume peaks at about age at 16.7 years in girls and 16.2 years in boys. The dorsal lateral prefrontal cortex, important for controlling impulses, is among the latest brain regions to mature without reaching adult dimensions until the early 20s.❞
Source: Structural Magnetic Resonance Imaging of the Adolescent Brain
There are several things to note here:
- The above statement is talking about the physical size of the brain growing
- Nowhere does he say “and stops developing at 25”
However… The study only looked at brains up to the age of 25. After that, they stopped looking, because the study was about “the adolescent brain” so there has to be a cut-off somewhere, and that was the cut-off they chose.
This is the equivalent of saying “it didn’t stop raining until four o’clock” when the reality is that four o’clock is simply when you gave up on checking.
The study didn’t misrepresent this, by the way, but the popular press did!
Another 2012 study looked at various metrics of brain development, and found:
- Synapse overproduction into the teens
- Cortex pruning into the late 20s
- Prefrontal pruning into middle age at least (they stopped looking)
- Myelination beyond middle age (they stopped looking)
Source: Experience and the developing prefrontal cortex ← check out figure 1, and make sure you’re looking at the human data not the rat data
So how’s the most recent research looking?
Here’s a 2022 study that looked at 123,984 brain scans spanning the age range from mid-gestation to 100 postnatal years, and as you can see from its own figure 1… Most (if not all) brain-things keep growing for life, even though most slow down at some point, they don’t stop:
Brain charts for the human lifespan ← check out figure 1; don’t get too excited about the ventricular volume column as that is basically “brain that isn’t being a brain”. Do get excited about the rest, though!
Want to know how not to get caught out by science being misrepresented by the popular press? Check out:
How Science News Outlets Can Lie To You (Yes, Even If They Cite Studies!)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
What should I do if I can’t see a psychiatrist?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
People presenting at emergency with mental health concerns are experiencing the longest wait times in Australia for admission to a ward, according to a new report from the Australasian College of Emergency Medicine.
But with half of New South Wales’ public psychiatrists set to resign next week after ongoing pay disputes – and amid national shortages in the mental health workforce – Australians who rely on psychiatry support may be wondering where else to go.
If you can’t get in to see a psychiatrist and you need help, there are some other options. However in an emergency, you should call 000.
Why do people see a psychiatrist?
Psychiatrists are doctors who specialise in mental health and can prescribe medication.
People seek or require psychiatry support for many reasons. These may include:
- severe depression, including suicidal thoughts or behaviours
- severe anxiety, panic attacks or phobias
- post-traumatic stress disorder (PTSD)
- eating disorders, such as anorexia or bulimia
- attention deficit hyperactivity disorder (ADHD).
Psychiatrists complement other mental health clinicians by prescribing certain medications and making decisions about hospital admission. But when psychiatry support is not available a range of team members can contribute to a person’s mental health care.
Can my GP help?
Depending on your mental health concerns, your GP may be able to offer alternatives while you await formal psychiatry care.
GPs provide support for a range of mental health concerns, regardless of formal diagnosis. They can help address the causes and impact of issues including mental distress, changes in sleep, thinking, mood or behaviour.
The GP Psychiatry Support Line also provides doctors advice on care, prescription medication and how support can work.
It’s a good idea to book a long consult and consider taking a trusted person. Be explicit about how you’ve been feeling and what previous supports or medication you’ve accessed.
What about psychologists, counsellors or community services?
Your GP should also be aware of supports available locally and online.
For example, Head to Health is a government initiative, including information, a nationwide phone line, and in-person clinics in Victoria. It aims to improve mental health advice, assessment and access to treatment.
Medicare Mental Health Centres provide in-person care and are expanding across Australia.
There are also virtual care services in some areas. This includes advice on individualised assessment including whether to go to hospital.
Some community groups are led by peers rather than clinicians, such as Alternatives to Suicide.
How about if I’m rural or regional?
Accessing support in rural or regional areas is particularly tough.
Beyond helplines and formal supports, other options include local Suicide Prevention Networks and community initiatives such as ifarmwell and Men’s sheds.
Should I go to emergency?
As the new report shows, people who present at hospital emergency departments for mental health should expect long wait times before being admitted to a ward.
But going to a hospital emergency department will be essential for some who are experiencing a physical or mental health crisis.
Managing suicide-related distress
With the mass resignation of NSW psychiatrists looming, and amid shortages and blown-out emergency waiting times, people in suicide-related distress must receive the best available care and support.
Roughly nine Australians die by suicide each day. One in six have had thoughts of suicide at some point in their lives.
Suicidal thoughts can pass. There are evidence-based strategies people can immediately turn to when distressed and in need of ongoing care.
Safety planning is a popular suicide prevention strategy to help you stay safe.
What is a safety plan?
This is a personalised, step-by-step plan to remain safe during the onset or worsening of suicidal urges.
You can develop a safety plan collaboratively with a clinician and/or peer worker, or with loved ones. You can also make one on your own – many people like to use the Beyond Now app.
Safety plans usually include:
- recognising personal warning signs of a crisis (for example, feeling like a burden)
- identifying and using internal coping strategies (such as distracting yourself by listening to favourite music)
- seeking social supports for distraction (for example, visiting your local library)
- letting trusted family or friends know how you’re feeling – ideally, they should know they’re in your safety plan
- knowing contact details of specific mental health services (your GP, mental health supports, local hospital)
- making the environment safer by removing or limiting access to lethal means
- identifying specific and personalised reasons for living.
Our research shows safety planning is linked to reduced suicidal thoughts and behaviour, as well as feelings of depression and hopelessness, among adults.
Evidence from people with lived experience shows safety planning helps people to understand their warning signs and practice coping strategies.

Sharing your safety plan with loved ones may help understand warning signs of a crisis. Dragana Gordic/Shutterstock Are there helplines I can call?
There are people ready to listen, by phone or online chat, Australia-wide. You can try any of the following (most are available 24 hours a day, seven days a week):
Suicide helplines:
- Lifeline 13 11 14
- Suicide Call Back Service 1300 659 467
There is also specialised support:
- for men: MensLine Australia 1300 78 99 78
- children and young people: Kids’ Helpline 1800 55 1800
- Aboriginal and Torres Strait Islander people: 13YARN 13 92 76
- veterans and their families: Open Arms 1800 011 046
- LGBTQIA+ community: QLife 1300 184 527
- new and expecting parents: PANDA 1300 726 306
- people experiencing eating disorders: Butterfly Foundation 1800 33 4673.
Additionally, each state and territory will have its own list of mental health resources.
With uncertain access to services, it’s helpful to remember that there are people who care. You don’t have to go it alone.
Monika Ferguson, Senior Lecturer in Mental Health, University of South Australia and Nicholas Procter, Professor and Chair: Mental Health Nursing, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: