10almonds Tells The Tea…
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s Bust Some Myths!
It’s too late after puberty, hormones won’t change xyz
While yes, many adult trans people dearly wish they’d been able to medically transition before going through the “wrong” puberty, the truth is that a lot of changes will still occur later… even to “unchangeable” things like the skeleton.
The body is remaking itself throughout life, and hormones tell it how to do that. Some parts are just quicker or slower than others. Also: the skeleton is pulled-on constantly by our muscles, and in a battle of muscle vs bone, muscle will always win over time.
Examples of this include:
- trans men building bigger bones to support their bigger muscles
- trans women getting smaller, with wider hips and a pelvic tilt
Trans people have sporting advantages
Assuming at least a year’s cross-sex hormonal treatment, there is no useful advantage to being trans when engaging in a sport. There are small advantages and disadvantages (which goes for any person’s body, really). For example:
- Trans women will tend to be taller than cis women on average…
- …but that larger frame is now being powered by smaller muscles, because they shrink much quicker than the skeleton.
- Trans men taking T are the only athletes allowed to take testosterone…
- …but they will still often be smaller than their fellow male competitors, for example.
Read: Do Trans Women Athletes Have Advantages? (A rather balanced expert overview, which does also cover trans men)
There’s a trans population explosion; it’s a social contagion epidemic!
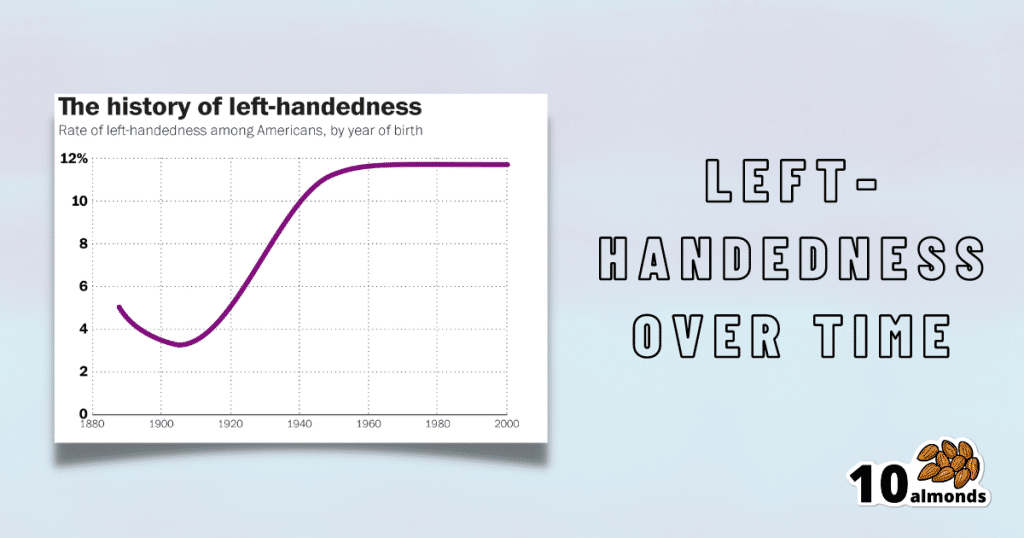
Source for figures: The Overall Rate Of Left-Handedness (Researchgate)
Left-handed people used to make up around 3% of the population… Until the 1920s, when that figure jumped sharply upwards, before plateauing at around 12% in around 1960, where it’s stayed since. What happened?! Simple, schools stopped forcing children to use their right hand.
Today, people ask for trans healthcare because they know it exists! Decades ago, it wasn’t such common knowledge.
The same explanation can be applied to other “population explosions” such as for autism and ADHD.
Fun fact: Mt. Everest was “discovered” in 1852, but scientists suspect it probably existed long before then! People whose ancestors were living on it long before 1852 also agree. Sometimes something exists for a long time, and only comes to wider public awareness later.
Transgender healthcare is too readily available, especially to children!
To believe some press outlets, you’d think:
- HRT is available from school vending machines,
- kids can get a walk-in top surgery at recess,
- and there’s an after-school sterilization club.
In reality, while availability varies from place to place, trans healthcare is heavily gatekept. Even adults have trouble getting it, often having to wait years and/or pay large sums of money… and get permission from a flock of doctors, psychologists, and the like. For those under the age of 18, it’s almost impossible in many places, even with parental support.
Puberty-blockers shouldn’t be given to teenagers, as the effects are irreversible
Quick question: who do you think should be given puberty-blockers? For whom do you think they were developed? Not adults, for sure! They were not developed for trans teens either, but for cis pre-teens with precocious puberty, to keep puberty at bay, to do it correctly later. Nobody argues they’re unsafe for much younger cis children, and only object when it’s trans teens.
They’re not only safe and reversible, but also self-reversing. Stop taking them, and the normally scheduled puberty promptly ensues by itself. For trans kids, the desired effect is to buy the kid time to make an informed and well-considered decision. After all, the effects of the wrong puberty are really difficult to undo!
A lot of people rush medical transition and regret it!
Trans people wish it could be rushed! It’s a lot harder to get gender-affirming care as a trans person, than it is to get the same (or comparable) care as a cis person. Yes, cis people get gender-affirming care, from hormones to surgeries, and have done for a long time.
As for regret… Medical transition has around a 1% regret rate. For comparison, hip replacement has a 4.8% regret rate and knee replacement has a 17.1% regret rate.
A medical procedure with a 99% success rate would generally be considered a miracle cure!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Tight Hamstrings? Here’s A Test To Know If It’s Actually Your Sciatic Nerve

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Tight hamstrings are often not actually due to hamstring issues, but rather, are often being limited by the sciatic nerve. This video offers a home test to determine if the sciatic nerve is causing mobility problems (and how to improve it, if so):
The Connection
Try this test:
- Sit down with a slumped posture.
- Extend one leg with the ankle flexed.
- Note any stretching or pulling sensation behind the knee or in the calf.
- Bring your head down to your chest
If this increases the sensation, it likely indicates sciatic nerve involvement.
If only the hamstrings are tight, head movement won’t change the stretch sensation.
This is because the nervous system is a continuous structure, so head movement can affect nerve tension throughout the body. While this can cause problems, it can also be integral in the solution. Here are two ways:
- Flossing method: sit with “poor” slumped posture, extend the knee, keep the ankle flexed, and lift the head to relieve nerve tension. This movement helps the sciatic nerve slide without stretching it.
- Even easier method: lie on your back, grab behind the knee, and extend the leg while extending the neck. This position avoids compression in the gluteal area, making it suitable for severely compromised nerves. Perform the movement without significant stretching or pain.
In both cases: move gently to avoid straining the nerve, which can worsen muscle tension. Do 10 repetitions per leg, multiple times a day; after a week, increase to 20 reps.
A word of caution: speak with your doctor before trying these exercises if you have underlying neurological diseases, cut or infected nerves, or other severe conditions.
For more on all of this, plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Exercises for Sciatica Pain Relief
Take care!
Share This Post
-
Dentists Debunk 15 Teeth Myths
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dentists Dr. John Yoo and Dr. Jason Lin leave no gaps in the truth:
The tooth, the whole tooth, and nothing but the tooth
Not only is there no tooth fairy (we are shocked), but also…
- “Baby teeth aren’t important.”
False! Baby teeth act as space holders for permanent teeth, affect speech development, and influence a child’s psychological well-being. - “Acidic fruits will whiten your smile.”
False! In any practical sense, anyway: acidic fruits may temporarily make teeth appear whiter by dispersing stains but cause enamel erosion and weaken teeth over time. - “Fillings last forever.”
False! Fillings can wear down, fail, or develop cavities underneath if oral hygiene isn’t maintained, requiring replacement over time. - “Cavities are irreversible.”
False! Cavities in the enamel can be reversed with fluoride and good oral hygiene, but cavities that reach the dentin are typically irreversible. - “Braces are just for crooked teeth.”
False! Braces also correct functional issues like overbites, underbites, crossbites, and prevent future complications like tooth impaction. - “A knocked-out tooth is gone for good.”
False! A knocked-out tooth can be reimplanted if done quickly (ideally within an hour); storing it in whole milk or saliva helps preserve it. - “Diet sodas won’t give you cavities.”
False! Diet sodas can still cause cavities due to their acidic pH, which erodes enamel, even without sugar. - “Dental cleanings aren’t necessary.”
False! Dental cleanings help remove plaque and tartar that regular brushing can’t, and allow for regular oral health checkups. - “Retainers aren’t for life.”
False! To maintain teeth alignment after braces, retainers should be worn long-term as teeth can shift even years later. - “You should floss before brushing.”
False! The order doesn’t matter, but do floss regularly. - “Everyone has wisdom teeth.”
False! Not everyone is born with wisdom teeth; they are the most commonly missing teeth, and not everyone needs them removed. - “Hydrogen peroxide and baking soda are good toothpaste replacements.”
False! While they are common components in toothpaste, they lack fluoride, which is essential for remineralizing and protecting enamel. - “You’re too old to get braces.”
False! There’s no age limit for braces or aligners; adults often seek them for both aesthetic and functional reasons. - “Teeth that have had root canals can’t feel.”
False! Teeth with root canals can’t feel pain from nerves, but you can still sense pressure due to surrounding ligaments. - “You’ll inevitably lose all your teeth when you’re old.”
False! Good oral hygiene and regular dental care can preserve natural teeth into old age, though genetics also play a role.
For more on each of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post
- “Baby teeth aren’t important.”
-
What Harm Can One Sleepless Night Do?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ll not bury the lede: a study found that just one night of 24-hour sleep deprivation can alter immune cell profiles in young, lean, healthy people to resemble those of people with obesity and chronic inflammation.
Chronic inflammation, in turn, causes very many other chronic diseases, and worsens most of the ones it doesn’t outright cause.
The reason this happens is because in principle, inflammation is supposed to be good for us—it’s our body’s defenses coming to the rescue. However, if we imagine our immune cells as firefighters, then compare:
- A team of firefighters who are in great shape and ready to deploy at a moment’s notice, are mostly allowed to rest, sometimes get training, and get called out to a fire from time time, just enough to keep them on their toes. Today, something in your house caught fire, and they showed up in 5 minutes and put it out safely.
- A team of firefighters who have been pulling 24-hour shifts every day for the past 20 years, getting called out constantly for lost cats, burned toast, wrong numbers, the neighbor’s music, a broken fridge, and even the occasional fire. Today, your printer got jammed so they broke down your door and also your windows just for good measure, and blasted your general desk area with a fire hose, which did not resolve the problem but now your computer itself is broken.
Which team would you rather have?
The former team is a healthy immune system; the latter is the immune system of someone with chronic inflammation.
But if it’s one night, it’s not chronic, right?
Contingently true. However, the problem is that because the immune profile was made to be like the bad team we described (imagine that chaos in your house, now remember that for this metaphor, it’s your body that that’s happening to), the immediate strong negative health impact will already have knock-on effects, which in turn make it more likely that you’ll struggle to get your sleep back on track quickly.
For example, the next night you may oversleep “to compensate”, but then the following day your sleep schedule is now slid back considerably; one thing leads to another, and a month later you’re thinking “I really must sort my sleep out”.
See also: How Regularity Of Sleep Can Be Even More Important Than Duration ← A recent, large (n=72,269) 8-year prospective* observational study of adults aged 40-79 found a strong association between irregular sleep and major cardiovascular events, to such an extent that it was worse than undersleeping.
*this means they started the study at a given point, and measured what happened for the next eight years—as opposed to a retrospective study, which would look at what had happened during the previous 8 years.
What about sleep fragmentation?
In other words: getting sleep, but heavily disrupted sleep.
The answer is: basically the same deal as with missed sleep.
Specifically, elevated proinflammatory cytokines (in this context, that’s bad) and an increase in nonclassical monocytes—as are typically seen in people with obesity and chronic inflammation.
Remember: these were young, lean, healthy participants going into the study, who signed up for a controlled sleep deprivation experiment.
This is important, because the unhealthy inflammatory profile means that people with such are a lot more likely to develop diabetes, heart disease, Alzheimer’s, and many more things besides. And, famously, most people in the industrialized world are not sleeping that well.
Even amongst 10almonds readers, a health-conscious demographic by nature, 62% of 10almonds readers do not regularly get the prescribed 7–9 hours sleep (i.e. they get under 7 hours).
You can see the data on this one, here: Why You Probably Need More Sleep ← yes, including if you are in the older age range; we bust that myth in the article too!*
*Unless you have a (rare!) mutated ADRB1 gene, which reduces that. But we also cover that in the article, and how to know whether you have it.
With regard to “most people in the industrialized world are not sleeping that well”, this means that most people in the industrialized world are subject to an unseen epidemic of sleep-deprivation-induced inflammation that is creating vulnerability to many other diseases. In short, the lifestyle of the industrialized world (especially: having to work certain hours) is making most of the working population sick.
Dr. Fatema Al-Rashed, lead researcher, concluded:
❝In the long term, we aim for this research to drive policies and strategies that recognize the critical role of sleep in public health.
We envision workplace reforms and educational campaigns promoting better sleep practices, particularly for populations at risk of sleep disruption due to technological and occupational demands.
Ultimately, this could help mitigate the burden of inflammatory diseases like obesity, diabetes, and cardiovascular diseases.❞
You can read the paper in full here: Impact of sleep deprivation on monocyte subclasses and function
What can we do about it?
With regard to sleep, we’ve written so much about this, but here are three key articles that contain a lot of valuable information:
- Get Better Sleep: Beyond The Basics
- Calculate (And Enjoy) The Perfect Night’s Sleep
- Safe Effective Sleep Aids For Seniors
…and with regard to inflammation, a good concise overview of how to dial it down is:
How To Prevent Or Reduce Inflammation
Take care!
Share This Post
Related Posts
-

Lemon vs Lime – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing lemons to limes, we picked the lemons.
Why?
This one’s simple today. They’re both comparable fruits in most ways, and their macro profiles are almost identical. When it comes to vitamins, however, they stand apart a little.
Both are most well-known for their vitamin C content, but lemons contain about 2x the vitamin C of limes.
In other vitamins, they’re not too far apart. Technically limes have 2x the vitamin A, but this doesn’t count for much because it’s a case of “two times almost nothing is still almost nothing”.
In the category of minerals, neither fruit is a very good source of most minerals, and the minerals they do have, are mostly more or less the same.
Both are acidic, and this can have blood sugar benefits in both cases (and, if not careful, damage tooth enamel in both cases). Nothing to set either apart from the other here.
So, it comes down to the vitamin C! In which category, lemons take the prize with their higher content.
Want to learn more?
You might like to read:
10 Ways To Balance Blood Sugars ← where it talks about the use of vinegar here, it’s about the acidity, so lemon juice or lime juice is an option too!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Kindness Method – by Shahroo Izadi
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Shahroo Izadi here covers everything from alcohol addiction to procrastination to weight loss. It’s a catch-all handbook for changing your habits—in general, and/or in whatever area of your life you most feel you want or need to.
She herself went from yo-yo dieting to a stable healthy lifestyle, and wants to share with us how she did it. So she took what worked for her, organized and dilstilled it, and named it “the kindness method”, which…
- promotes positivity not in a “head in the sand” sense but rather: you have strengths, let’s find them and use them
- offers many exploratory exercises to help you figure out what’s actually going to be best for you
- plans support in advance—you’re going to be your own greatest ally here
Basically it’s about:
- being kind to yourself rather than setting yourself up to fail, and “judging a fish by how well it can climb a tree”
- being kind to yourself by being compassionate towards your past self and moving on with lessons learned
- being kind to yourself by getting things in order for your future self, because you need to treat your future self like a loved one
In fact, why not buy a copy of this book as a gift for your future self?
Click Here To Order Your Copy of “The Kindness Method” on Amazon Today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How they did it: STAT reporters expose how ailing seniors suffer when Medicare Advantage plans use algorithms to deny care
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In a call with a long-time source, what stood out most to STAT reporters Bob Herman and Casey Ross was just how viscerally frustrated and angry the source was about an algorithm used by insurance companies to decide how long patients should stay in a nursing home or rehab facility before being sent home.
The STAT stories had a far-reaching impact:
- The U.S. Senate Committee on Homeland Security and Government Affairs took a rare step of launching a formal investigation into the use of algorithms by the country’s three largest Medicare Advantage insurers.
- Thirty-two House members urged the Centers for Medicare and Medicaid Services to increase the oversight of algorithms that health insurers use to make coverage decisions.
- In a rare step, CMS launched its own investigation into UnitedHealth. It also stiffened its regulations on the use of proprietary algorithms and introduced plans to audit denials across Medicare Advantage plans in 2024.
- Based on STAT’s reporting, Medicare Advantage beneficiaries filed two class-action lawsuits against UnitedHealth and its NaviHealth subsidiary, the maker of the algorithm, and against Humana, another major health insurance company that was also using the algorithm.
- Amid scrutiny, UnitedHealth renamed NaviHealth.
The companies never allowed an on-the-record interview with their executives, but they acknowledged that STAT’s reporting was true, according to the news organization.
Ross and Herman spoke with The Journalist’s Resource about their project and shared the following eight tips.
1. Search public comments on proposed federal rules to find sources.
Herman and Ross knew that the Centers for Medicare and Medicaid Services had put out a request for public comments, asking stakeholders within the Medicare Advantage industry how the system could improve.
There are two main ways to get Medicare coverage: original Medicare, which is a fee-for-service health plan, and Medicare Advantage, which is a type of Medicare health plan offered by private insurance companies that contract with Medicare. Medicare Advantage plans have increasingly become popular in recent years.
Under the Social Security Act, the public has the opportunity to submit comments on Medicare’s proposed national coverage determinations. CMS uses public comments to inform its proposed and final decisions. It responds in detail to all public comments when issuing a final decision.
The reporters began combing through hundreds of public comments attached to a proposed Medicare Advantage rule that was undergoing federal review. NaviHealth, the UnitedHealth subsidiary and the maker of the algorithm, came up in many of the comments, which include the submitters’ information.
“These are screaming all-caps comments to federal regulators about YOU NEED TO SOMETHING ABOUT THIS BECAUSE IT’S DISGUSTING,” Ross says.
“The federal government is proposing rules and regulations all the time,” adds Herman, STAT’s business of health care reporter. “If someone’s going to take the time and effort to comment on them, they must have at least some knowledge of what’s going on. It’s just a great tool for any journalist to use to figure out more and who to contact.”
The reporters also found several attorneys who had complained in the comments. They began reaching out to them, eventually gaining access to confidential documents and intermediaries who put them in touch with patients to show the human impact of the algorithm.
2. Harness the power of the reader submission box.
At the suggestion of an editor, the reporters added a reader submission box at the bottom of their first story, asking them to share their own experiences with Medicare Advantage denials.
The floodgates opened. Hundreds of submissions arrived.
By the end of their first story, Herman and Ross had confidential records and some patients, but they had no internal sources in the companies they were investigating, including Navihealth. The submission box led them to their first internal source.

(Screenshot of STAT’s submission box.) The journalists also combed through LinkedIn and reached out to former and current employees, but the response rate was much lower than what they received via the submission box.
The submission box “is just right there,” Herman says. “People who would want to reach out to us can do it right then and there after they read the story and it’s fresh in their minds.”
3. Mine podcasts relevant to your story.
The reporters weren’t sure if they could get interviews with some of the key figures in the story, including Tom Scully, the former head of the Centers for Medicare and Medicaid Services who drew up the initial plans for NaviHealth years before UnitedHealth acquired it.
But Herman and another colleague had written previously about Scully’s private equity firm and they had found a podcast where he talked about his work. So Herman went back to the podcast — where he discovered Scully had also discussed NaviHealth.
The reporters also used the podcast to get Scully on the phone for an interview.
“So we knew we had a good jumping off point there to be like, ‘OK, you’ve talked about NaviHealth on a podcast, let’s talk about this,’” Herman says. “I think that helped make him more willing to speak with us.”
4. When covering AI initiatives, proceed with caution.
“A source of mine once said to me, ‘AI is not magic,’” Ross says. “People need to just ask questions about it because AI has this aura about it that it’s objective, that it’s accurate, that it’s unquestionable, that it never fails. And that is not true.”
AI is not a neutral, objective machine, Ross says. “It’s based on data that’s fed into it and people need to ask questions about that data.”
He suggests several questions to ask about the data behind AI tools:
- Where does the data come from?
- Who does it represent?
- How is this tool being applied?
- Do the people to whom the tool is being applied match the data on which it was trained? “If racial groups or genders or age of economic situations are not adequately represented in the training set, then there can be an awful lot of bias in the output of the tool and how it’s applied,” Ross says.
- How is the tool applied within the institution? Are people being forced to forsake their judgment and their own ability to do their jobs to follow the algorithm?
5. Localize the story.
More than half of all Medicare beneficiaries have Medicare Advantage and there’s a high likelihood that there are multiple Medicare Advantage plans in every county across the nation.
“So it’s worth looking to see how Medicare Advantage plans are growing in your area,” Herman says.
Finding out about AI use will most likely rely on shoe-leather reporting of speaking with providers, nursing homes and rehab facilities, attorneys and patients in your community, he says. Another source is home health agencies, which may be caring for patients who were kicked out of nursing homes and rehab facilities too soon because of a decision by an algorithm.
The anecdote that opens their first story involves a small regional health insurer in Wisconsin, which was using NaviHealth and a contractor to manage post-acute care services, Ross says.
“It’s happening to people in small communities who have no idea that this insurer they’ve signed up with is using this tool made by this other company that operates nationally,” Ross says.
There are also plenty of other companies like NaviHealth that are being used by Medicare Advantage plans, Herman says. “So it’s understanding which Medicare Advantage plans are being sold in your area and then which post-acute management companies they’re using,” he adds.
Some regional insurers have online documents that show which contractors they use to evaluate post-acute care services.
6. Get familiar with Medicare’s appeals databases
Medicare beneficiaries can contest Medicare Advantage denials through a five-stage process, which can last months to years. The appeals can be filed via the Office of Medicare Hearings and Appeals.
“Between 2020 and 2022, the number of appeals filed to contest Medicare Advantage denials shot up 58%, with nearly 150,000 requests to review a denial filed in 2022, according to a federal database,” Ross and Herman write in their first story. “Federal records show most denials for skilled nursing care are eventually overturned, either by the plan itself or an independent body that adjudicates Medicare appeals.”
There are several sources to find appeals data. Be mindful that the cases themselves are not public to protect patient privacy, but you can find the number of appeals filed and the rationale for decisions.
CMS has two quality improvement organizations, or QIOs, Livanta and Kepro, which are required to file free, publicly-available annual reports, about the cases they handle, Ross says.
Another company, Maximus, a Quality Improvement Contractor, also files reports on prior authorization cases it adjudicates for Medicare. The free annual reports include data on raw numbers of cases and basic information about the percentage denials either overturned or upheld on appeal, Ross explains.
CMS also maintains its own database on appeals for Medicare Part C (Medicare Advantage plans) and Part D, which covers prescription drugs, although the data is not complete, Ross explains.
7. Give your editor regular updates.
“Sprinkle the breadcrumbs in front of your editors,” Ross says.
“If you wrap your editors in the process, you’re more likely to be able to get to the end of [the story] before they say, ‘That’s it! Give me your copy,’” Ross says.
8. Get that first story out.
“You don’t have to know everything before you write that first story,” Ross says. “Because with that first story, if it has credibility and it resonates with people, sources will come forward and sources will continue to come forward.”
Read the stories
Denied by AI: How Medicare Advantage plans use algorithms to cut off care for seniors in need
UnitedHealth pushed employees to follow an algorithm to cut off Medicare patients’ rehab care
UnitedHealth used secret rules to restrict rehab care for seriously ill Medicare Advantage patients
This article first appeared on The Journalist’s Resource and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: