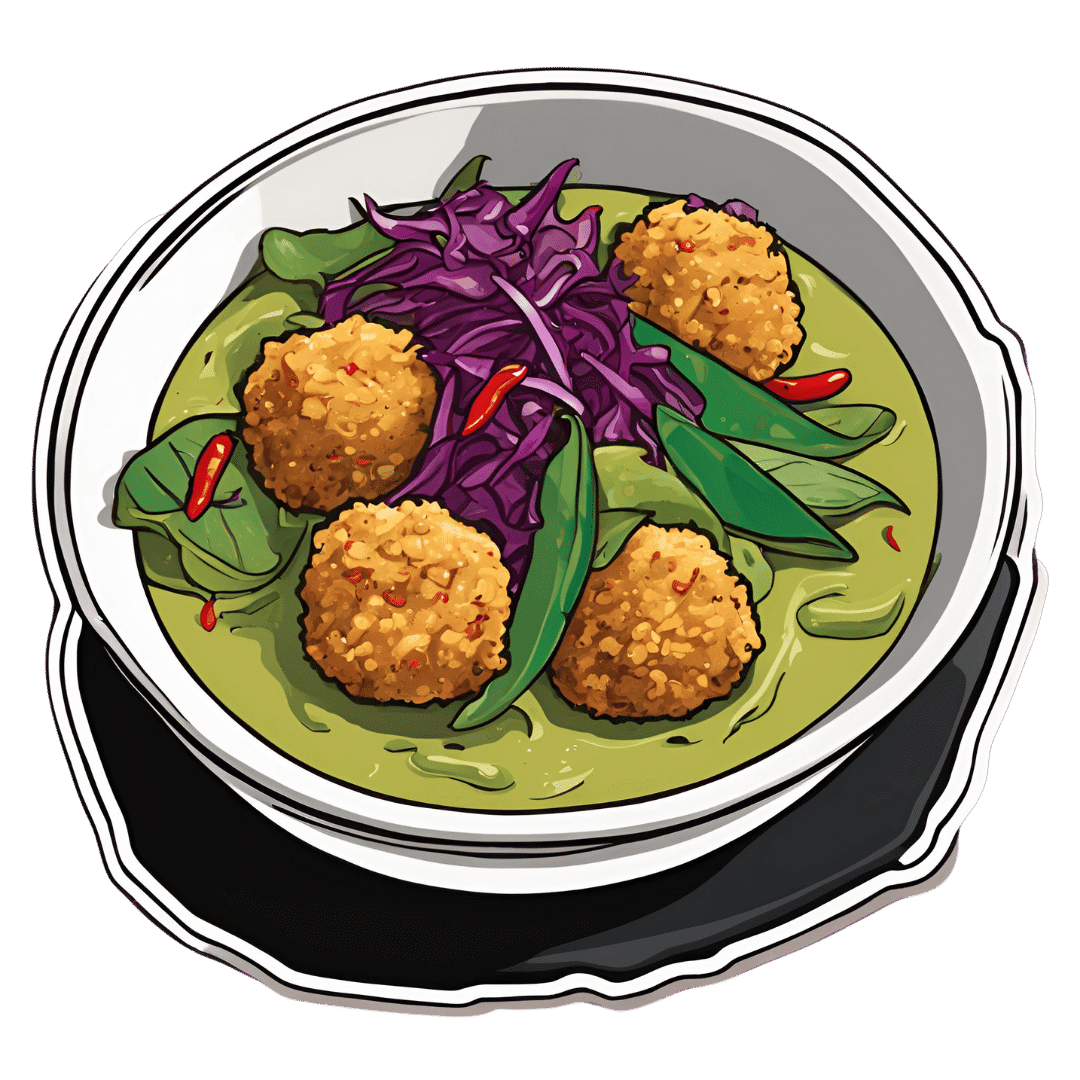
Thai Green Curry With Crispy Tofu Balls
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Diversity is key here, with a wide range of mostly plants, offering an even wider range of phytochemical benefits:
You will need
- 7 oz firm tofu
- 1 oz cashew nuts (don’t soak them)
- 1 tbsp nutritional yeast
- 1 tsp turmeric
- 4 scallions, sliced
- 7 oz mangetout
- 7 oz fermented red cabbage (i.e., from a jar)
- 1 cup coconut milk
- Juice of ½ lime
- 2 tsp light soy sauce
- 1 handful fresh cilantro, or if you have the “cilantro tastes like soap” gene, then parsley
- 1 handful fresh basil
- 1 green chili, chopped (multiply per heat preference)
- 1″ piece fresh ginger, roughly chopped
- ¼ bulb garlic, crushed
- 1 tsp red chili flakes
- 1 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
- Avocado oil for frying
- Recommended, to serve: lime wedges
- Recommended, to serve: your carbohydrate of choice, such as soba noodles or perhaps our Tasty Versatile Rice.
Method
(we suggest you read everything at least once before doing anything)
1) Heat the oven to 350℉ / 180℃, and bake the cashews on a baking tray for about 8 minutes until lightly toasted. Remove from the oven and allow to cool a little.
2) Combine the nuts, tofu, nutritional yeast, turmeric, and scallions in a food processor, and process until the ingredients begin to clump together. Shape into about 20 small balls.
3) Heat some oil in a skillet and fry the tofu balls, jiggling frequently to get all sides; it should take about 5 minutes to see them lightly browned. Set aside.
4) Combine the coconut milk, lime juice, soy sauce, cilantro/parsley, basil, scallions, green chili, ginger, garlic, and MSG/salt in a high-speed blender, and blend until a smooth liquid.
5) Transfer the liquid to a saucepan, and bring to the boil. Reduce the heat, add the mangetout, and simmer for about 5 minutes to reduce slightly. Stir in the red chili flakes and black pepper.
6) Serve with your preferred carbohydrate, adding the fermented red cabbage and the crispy tofu balls you set aside, along with any garnish you might like to add.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Capsaicin For Weight Loss And Against Inflammation
- Ginger Does A Lot More Than You Think
- Why Curcumin (Turmeric) Is Worth Its Weight In Gold
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Making Friends With Your Gut (You Can Thank Us Later)
- What’s Your Plant Diversity Score? ← a score of 8.25 for this dish, not counting whatever carbs you might add. Remember, herbs/spices* count for ¼ of a point each!
*but not MSG or salt, as while they may in culinary terms get lumped in with spices, they are of course not plants. Nor is nutritional yeast (nor any other yeast, for that matter). However, mushrooms (not seen in this recipe, though to be honest they would be a respectable addition) would get included for a whole point per mushroom type, since while they are not technically plants but fungi, the nutritional profile is plantlike.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Could Just Two Hours Sleep Per Day Be Enough?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Polyphasic Sleep… Super-Schedule Or An Idea Best Put To Rest?
What is it?
Let’s start by defining some terms:
- Monophasic sleep—sleeping in one “chunk” per day. For example, a good night’s “normal” sleep.
- Biphasic sleep—sleeping in two “chunks” per day. Typically, a shorter night’s sleep, with a nap usually around the middle of the day / early afternoon.
- Polyphasic sleep—sleeping in two or more “chunks per day”. Some people do this in order to have more hours awake per day, to do things. The idea is that sleeping this way is more efficient, and one can get enough rest in less time. The most popular schedules used are:
- The Überman schedule—six evenly-spaced 20-minute naps, one every four hours, throughout the 24-hour day. The name is a semi-anglicized version of the German word Übermensch, “Superman”.
- The Everyman schedule—a less extreme schedule, that has a three-hours “long sleep” during the night, and three evenly-spaced 20-minute naps during the day, for a total of 4 hours sleep.
There are other schedules, but we’ll focus on the most popular ones here.
Want to learn about the others? Visit: Polyphasic.Net (a website by and for polyphasic sleep enthusiasts)
Some people have pointed to evidence that suggests humans are naturally polyphasic sleepers, and that it is only modern lifestyles that have forced us to be (mostly) monophasic.
There is at least some evidence to suggest that when environmental light/dark conditions are changed (because of extreme seasonal variation at the poles, or, as in this case, because of artificial changes as part of a sleep science experiment), we adjust our sleeping patterns accordingly.
The counterpoint, of course, is that perhaps when at the mercy of long days/nights at the poles, or no air-conditioning to deal with the heat of the day in the tropics, that perhaps we were forced to be polyphasic, and now, with modern technology and greater control, we are free to be monophasic.
Either way, there are plenty of people who take up the practice of polyphasic sleep.
Ok, But… Why?
The main motivation for trying polyphasic sleep is simply to have more hours in the day! It’s exciting, the prospect of having 22 hours per day to be so productive and still have time over for leisure.
A secondary motivation for trying polyphasic sleep is that when the brain is sleep-deprived, it will prioritize REM sleep. Here’s where the Überman schedule becomes perhaps most interesting:
The six evenly-spaced naps of the Überman schedule are each 20 minutes long. This corresponds to the approximate length of a normal REM cycle.
Consequently, when your head hits the pillow, you’ll immediately begin dreaming, and at the end of your dream, the alarm will go off.
Waking up at the end of a dream, when one hasn’t yet entered a non-REM phase of sleep, will make you more likely to remember it. Similarly, going straight into REM sleep will make you more likely to be aware of it, thus, lucid dreaming.
Read: Sleep fragmentation and lucid dreaming (actually a very interesting and informative lucid dreaming study even if you don’t want to take up polyphasic sleep)
Six 20-minute lucid-dreaming sessions per day?! While awake for the other 22 hours?! That’s… 24 hours per day of wakefulness to use as you please! What sorcery is this?
Hence, it has quite an understandable appeal.
Next Question: Does it work?
Can we get by without the other (non-REM) kinds of sleep?
According to Überman cycle enthusiasts: Yes! The body and brain will adapt.
According to sleep scientists: No! The non-REM slow-wave phases of sleep are essential
Read: Adverse impact of polyphasic sleep patterns in humans—Report of the National Sleep Foundation sleep timing and variability consensus panel
(if you want to know just how bad it is… the top-listed “similar article” is entitled “Suicidal Ideation”)
But what about, for example, the Everman schedule? Three hours at night is enough for some non-REM sleep, right?
It is, and so it’s not as quickly deleterious to the health as the Überman schedule. But, unless you are blessed with rare genes that allow you to operate comfortably on 4 hours per day (you’ll know already if that describes you, without having to run any experiment), it’s still bad.
Adults typically need 7–9 hours of sleep per night, and if you don’t get it, you’ll accumulate a sleep debt. And, importantly:
When you accumulate sleep debt, you are borrowing time at a very high rate of interest!
And, at risk of laboring the metaphor, but this is important too:
Not only will you have to pay it back soon (with interest), you will be hounded by the debt collection agents—decreased cognitive ability and decreased physical ability—until you pay up.
In summary:
- Polyphasic sleep is really very tempting
- It will give you more hours per day (for a while)
- It will give the promised lucid dreaming benefits (which is great until you start micronapping between naps, this is effectively a mini psychotic break from reality lasting split seconds each—can be deadly if behind the wheel of a car, for instance!)
- It is unequivocally bad for the health and we do not recommend it
Bottom line:
Some of the claimed benefits are real, but are incredibly short-term, unsustainable, and come at a cost that’s far too high. We get why it’s tempting, but ultimately, it’s self-sabotage.
(Sadly! We really wanted it to work, too…)
Share This Post
-

Calm For Surgery – by Dr Chris Bonney
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As a general rule of thumb, nobody likes having surgery. We may like the results of the surgery, we may like having the surgery done and behind us, but surgery itself is not most people’s idea of fun, and honestly, the recovery period afterwards can be a pain in every sense of the word.
Dr. Chris Bonney, an anesthesiologist, gives us the industry-secrets low-down, and is the voice of experience when it comes to the things to know about and/or prepare in advance—the little things that make a world of difference to your in-hospital experience and afterwards.
Think of it like “frequent flyer traveller tips” but for surgeries, whereupon knowing a given tip can mean the difference between deeply traumatic suffering and merely not being at your usual best. We think that’s worth it.
Share This Post
-

Beta-Blockers: Useless vs Heart Attacks & Worse For Women?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Currently, more than 80% of uncomplicated heart attack patients are discharged on beta-blockers—this has been the go-to standard of care for the past 40 years—notwithstanding that there are common side effects such as bradycardia (slow heart rate), and resultant fatigue and sexual dysfunction.
However, researchers (Dr. Borja Ibanez et al.) have turned that on its head with a sweeping study involving 8,505 patients enrolled across 109 hospitals in Spain and Italy, randomized to receive or not receive beta-blockers, with a median follow-up of a little under 4 years.
What they found
In few words: overall, there was no significant differences between groups in death, recurrent heart attack, or hospitalization for heart failure.
However, for women specifically, they did find that there was (in the beta-blocker group), a slightly higher absolute risk of death over 3.7 years, plus higher rates of heart attack or heart failure hospitalization—specifically, they more often had heart attacks without obstructive coronary arteries.
Some of this disparity may be explained by the fact that women were less often prescribed recommended secondary prevention therapies (e.g. antiplatelet therapies, ACE inhibitors/ARBs, and cardiac rehabilitation) despite high overall prescription rates, but not all of it, because those receiving higher beta-blocker doses also saw a correspondingly higher risk.
You can find the paper itself here: Beta-Blockers after Myocardial Infarction without Reduced Ejection Fraction
And further modelling of more or less the same data here: Beta-blockers after myocardial infarction: effects according to sex in the REBOOT trial
You may be wondering: why “more or else”? Because they are both running numbers from the same trial, but the latter used only the intention-to-treat population, which was 8,438 out of the 8,505 patients.
One more thing…
While beta-blockers are generally considered “calming” (indeed, historically they’ve sometimes been prescribed for anxiety; less so nowadays), hence the bradycardia we mentioned in the introduction, this does mean that they can also promote depression—without actually alleviating anxiety:
❝At baseline, 27% of patients were possible cases of anxiety (m, 5.6; SD, 3.9) and 14% were possible cases of depression (m, 3.9; SD, 3.2). Beta-blocker treatment had a [worsening] effect on depressive symptoms at both follow-ups 1 (β = 0.48; 95% CI 09–0.86; P = 0.015) and 2 (β = 0.41; 95% CI = 0.01–0.81; P = 0.047), but no effect on anxiety.❞
Want to learn more?
For more on sex differences in this matter, see:
- Statins: His & Hers ← for women, statins are (in most cases) less useful and more potentially harmful
- Heart Attacks: His & Hers
And for why a lot of this kind of medical disparity occurs when it comes to outcomes:
Unwell Women: Misdiagnosis and Myth in a Man-Made World – by Elinor Cleghorn
Take care!
Share This Post

Related Posts
-

The Age of Scientific Wellness – by Dr. Leroy Hood & Dr. Nathan Price
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t usually do an author bio beyond mentioning their professional background, but in this case it’s worth mentioning that the first-listed author, Dr. Leroy Hood, is the one who invented the automated gene sequencing technology that made the Human Genome Project possible. In terms of awards, he’s won everything short of a Nobel Prize, and that’s probably less a snub and more a matter of how there isn’t a Nobel Prize for Engineering—his field is molecular biotechnology, but what he solved was an engineering problem.
In this book, the authors set out to make the case that “find it and fix it” medicine has done a respectable job of getting us where we are, but what we need now is P4 medicine:
- Predict
- Prevent
- Personalize
- Participate
The idea is that with adequate data (genomic, phenomic, and digital), we can predict the course of health sufficiently well to interrupt the process of disease at its actual (previously unseen) starting point, instead of waiting for symptoms to show up, thus preventing it proactively. The personalization is because this will not be a “one size fits all” approach, since our physiologies are different, our markers of health and disease will be somewhat too. And the participatory aspect? That’s because the only way to get enough data to do this for an entire population is with—more or less—an entire population’s involvement.
This is what happens when, for example, your fitness tracker asks if it can share anonymized health metrics for research purposes and you allow it—you are becoming part of the science (a noble and worthy act!).
You may be wondering whether this book has health advice, or is more about the big picture. And, the answer is both. It’s mostly about the big picture but it does have a lot of (data-driven!) health advice too, especially towards the end.
The style is largely narrative, talking the reader through the progresses (and setbacks) that have marked the path so far, and projecting the next part of the journey, in the hope that we can avoid being part of a generation born just too late to take advantage of this revolutionary approach to health.
Bottom line: this isn’t a very light read, but it is a worthwhile one, and it’ll surely inspire you to increase the extent to which you are proactive about your health!
Click here to check out The Age Of Scientific Wellness, and be part of it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Insider’s Guide To Making Hospital As Comfortable As Possible
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Nobody Likes Surgery, But Here’s How To Make It Much Less Bad

This is Dr. Chris Bonney. He’s an anesthesiologist. If you have a surgery, he wants you to go in feeling calm, and make a quick recovery afterwards, with minimal suffering in between.
Being a patient in a hospital is a bit like being a passenger in an airplane:
- Almost nobody enjoys the thing itself, but we very much want to get to the other side of the experience.
- We have limited freedoms and comforts, and small things can make a big difference between misery and tolerability.
- There are professionals present to look after us, but they are busy and have a lot of other people to tend to too.
So why is it that there are so many resources available full of “tips for travelers” and so few “tips for hospital patients”?
Especially given the relative risks of each, and likelihood, or even near-certainty of coming to at least some harm… One would think “tips for patients” would be more in demand!
Tips for surgery patients, from an insider expert
First, he advises us: empower yourself.
Empowering yourself in this context means:
- Relax—doctors really want you to feel better, quickly. They’re on your side.
- Research—knowledge is power, so research the procedure (and its risks!). Dr. Bonney, himself an anesthesiologist, particularly recommends you learn what specific anesthetic will be used (there are many, and they’re all a bit different!), and what effects (and/or after-effects) that may have.
- Reframe—you’re not just a patient; you’re a customer/client. Many people suffer from MDeity syndrome, and view doctors as authority figures, rather than what they are: service providers.
- Request—if something would make you feel better, ask for it. If it’s information, they will be not only obliged, but also enthusiastic, to give it. If it’s something else, they’ll oblige if they can, and the worst case scenario is something won’t be possible, but you won’t know if you don’t ask.
Next up, help them to help you
There are various ways you can be a useful member of your own care team:
- Go into surgery as healthy as you can. If there’s ever a time to get a little fitter, eat a little healthier, prioritize good quality sleep more, the time approaching your surgery is the time to do this.
- This will help to minimize complications and maximize recovery.
- Take with you any meds you’re taking, or at least have an up-to-date list of what you’re taking. Dr. Bonney has very many times had patients tell him such things as “Well, let me see. I have two little pink ones and a little white one…” and when asked what they’re for they tell him “I have no idea, you’d need to ask my doctor”.
- Help them to help you; have your meds with you, or at least a comprehensive list (including: medication name, dosage, frequency, any special instructions)
- Don’t stop taking your meds unless told to do so. Many people have heard that one should stop taking meds before a surgery, and sometimes that’s true, but often it isn’t. Keep taking them, unless told otherwise.
- If unsure, ask your surgical team in advance (not your own doctor, who will not be as familiar with what will or won’t interfere with a surgery).
Do any preparatory organization well in advance
Consider the following:
- What do you need to take with you? Medications, clothes, toiletries, phone charger, entertainment, headphones, paperwork, cash for the vending machine?
- Will the surgeons need to shave anywhere, and if so, might you prefer doing some other form of depilation (e.g. waxing etc) yourself in advance?
- Is your list of medications ready?
- Who will take you to the hospital and who will bring you back?
- Who will stay with you for the first 24 hours after you’re sent home?
- Is someone available to look after your kids/pets/plants etc?
Be aware of how you do (and don’t) need to fast before surgery
The American Society of Anesthesiologists gives the following fasting guidelines:
- Non-food liquids: fast for at least 2 hours before surgery
- Food liquids or light snacks: fast for at least 6 hours before surgery
- Fried foods, fatty foods, meat: fast for at least 8 hours before surgery
(see the above link for more details)
Dr. Bonney notes that many times he’s had patients who’ve had the worst thirst, or caffeine headache, because of abstaining unnecessarily for the day of the surgery.
Unless told otherwise by your surgical team, you can have black coffee/tea up until two hours before your surgery, and you can and should have water up until two hours before surgery.
Hydration is good for you and you will feel the difference!
Want to know more?
Dr. Bonney has his own website and blog, where he offers lots of advice, including for specific conditions and specific surgeries, with advice for before/during/after your hospital stay.
He also has a book with many more tips like those we shared today:
Calm For Surgery: Supertips For A Smooth Recovery
Take good care of yourself!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Red Lentils vs Oats – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red lentils to oats, we picked the oats.
Why?
In terms of macros, oats have more protein, carbs, fiber, and even a little fat—mostly healthy mono- and polyunsaturated fats, thus making them the more nutritionally dense. That said, red lentils have the lower glycemic index, (low GI compared to oats’ medium GI) which offsets that, so we’ll call this category a tie.
In the category of vitamins, red lentils have more of vitamins B6, B9, and choline, while oats have more of vitamins B1, B2, and B5. Another tie!
When it comes to minerals, however, we have a tiebreaker category: red lentils have more selenium, while oats have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc. An easy win for oats this time!
So, thanks to the minerals, oats are the clear winner in total. But by all means, enjoy either or both; diversity is good!
Want to learn more?
You might like to read:
The Best Kind Of Fiber For Overall Health? ← it’s β-glucan, the kind find in oats!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: