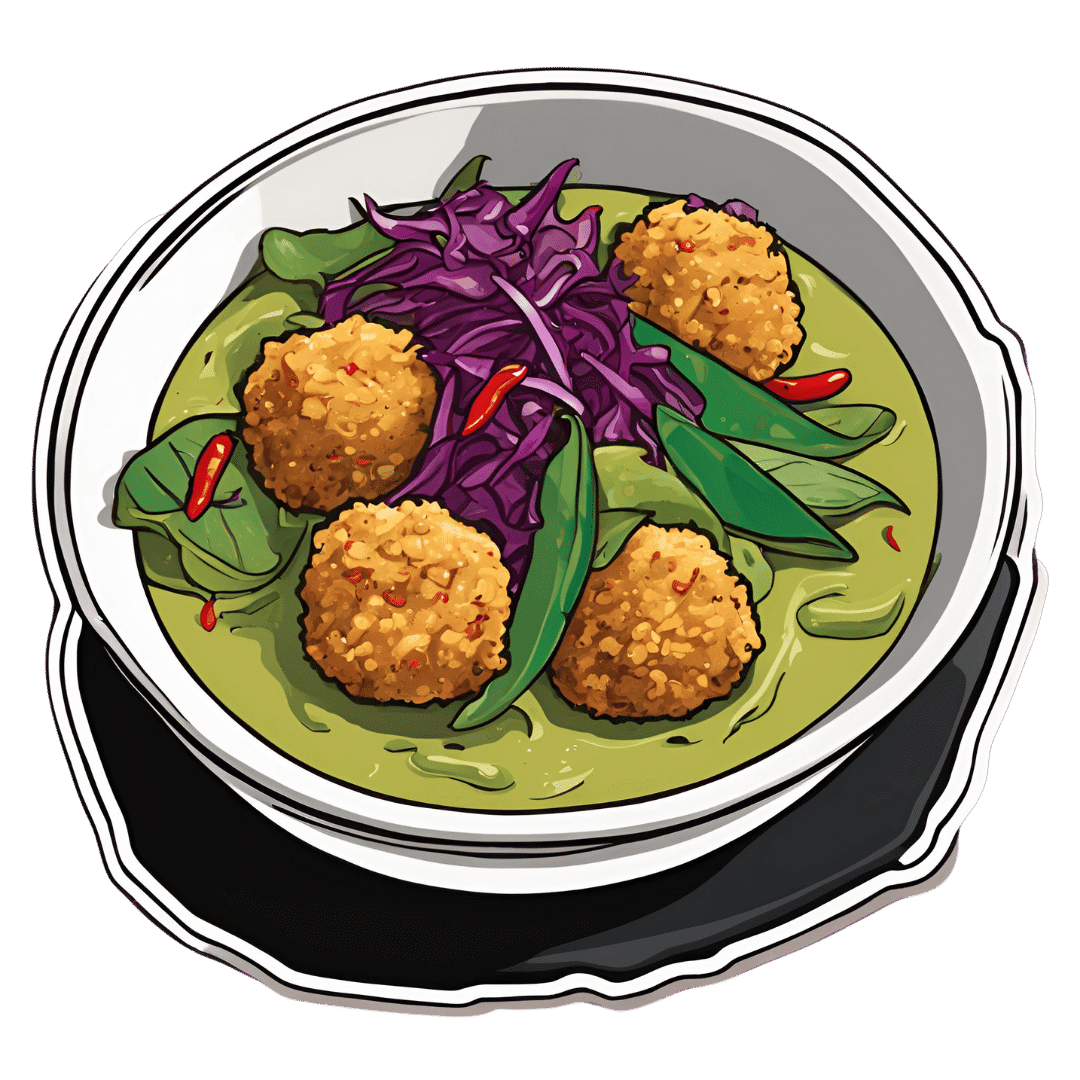
Thai Green Curry With Crispy Tofu Balls
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Diversity is key here, with a wide range of mostly plants, offering an even wider range of phytochemical benefits:
You will need
- 7 oz firm tofu
- 1 oz cashew nuts (don’t soak them)
- 1 tbsp nutritional yeast
- 1 tsp turmeric
- 4 scallions, sliced
- 7 oz mangetout
- 7 oz fermented red cabbage (i.e., from a jar)
- 1 cup coconut milk
- Juice of ½ lime
- 2 tsp light soy sauce
- 1 handful fresh cilantro, or if you have the “cilantro tastes like soap” gene, then parsley
- 1 handful fresh basil
- 1 green chili, chopped (multiply per heat preference)
- 1″ piece fresh ginger, roughly chopped
- ¼ bulb garlic, crushed
- 1 tsp red chili flakes
- 1 tsp black pepper, coarse ground
- ½ tsp MSG or 1 tsp low-sodium salt
- Avocado oil for frying
- Recommended, to serve: lime wedges
- Recommended, to serve: your carbohydrate of choice, such as soba noodles or perhaps our Tasty Versatile Rice.
Method
(we suggest you read everything at least once before doing anything)
1) Heat the oven to 350℉ / 180℃, and bake the cashews on a baking tray for about 8 minutes until lightly toasted. Remove from the oven and allow to cool a little.
2) Combine the nuts, tofu, nutritional yeast, turmeric, and scallions in a food processor, and process until the ingredients begin to clump together. Shape into about 20 small balls.
3) Heat some oil in a skillet and fry the tofu balls, jiggling frequently to get all sides; it should take about 5 minutes to see them lightly browned. Set aside.
4) Combine the coconut milk, lime juice, soy sauce, cilantro/parsley, basil, scallions, green chili, ginger, garlic, and MSG/salt in a high-speed blender, and blend until a smooth liquid.
5) Transfer the liquid to a saucepan, and bring to the boil. Reduce the heat, add the mangetout, and simmer for about 5 minutes to reduce slightly. Stir in the red chili flakes and black pepper.
6) Serve with your preferred carbohydrate, adding the fermented red cabbage and the crispy tofu balls you set aside, along with any garnish you might like to add.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Capsaicin For Weight Loss And Against Inflammation
- Ginger Does A Lot More Than You Think
- Why Curcumin (Turmeric) Is Worth Its Weight In Gold
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
- Making Friends With Your Gut (You Can Thank Us Later)
- What’s Your Plant Diversity Score? ← a score of 8.25 for this dish, not counting whatever carbs you might add. Remember, herbs/spices* count for ¼ of a point each!
*but not MSG or salt, as while they may in culinary terms get lumped in with spices, they are of course not plants. Nor is nutritional yeast (nor any other yeast, for that matter). However, mushrooms (not seen in this recipe, though to be honest they would be a respectable addition) would get included for a whole point per mushroom type, since while they are not technically plants but fungi, the nutritional profile is plantlike.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Intuitive Eating – by Evelyn Tribole and Elyse Resch

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may be given to wonder: if this is about intuitive eating, and an anti-diet approach, why a whole book?
There’s a clue in the other part of the title: “4th Edition”.
The reason there’s a 4th edition (and before it, a 3rd and 2nd edition) is because this book is very much full of science, and science begets more science, and the evidence just keeps on rolling in.
While neither author is a doctor, each has a sizeable portion of the alphabet after their name (more than a lot of doctors), and this is an incredibly well-evidenced book.
The basic premise from many studies is that restrictive dieting does not work well long-term for most people, and instead, better is to make use of our bodies’ own interoceptive feedback.
You see, intuitive eating is not “eat randomly”. We do not call a person “intuitive” because they speak or act randomly, do we? Same with diet.
Instead, the authors give us ten guiding principles (yes, still following the science) to allow us a consistent “finger on the pulse” of what our body has to say about what we have been eating, and what we should be eating.
Bottom line: if you want to be a lot more in tune with your body and thus better able to nourish it the way it needs, this book is literally on the syllabus for many nutritional science classes, and will stand you in very good stead!
Share This Post
-

The Distracted Mind – by Dr. Adam Gazzaley and Dr. Larry Rosen
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Yes, yes, we know, unplug once in a while. But what else do this highly-qualified pair of neuroscientists have to offer?
Rather than being a book for the sake of being a book, with lots of fluff and the usual advice about single-tasking, the authors start with a reframe:
Neurologically speaking, the hit of dopamine we get when looking for information is the exact same as the hit of dopamine that we, a couple of hundred thousand years ago, got when looking for nuts and berries.
- When we don’t find them, we become stressed, and search more.
- When we do find them, we are encouraged and search more nearby, and to the other side of nearby, and near around, to find more.
But in the case of information (be it useful information or celebrity gossip or anything in between), the Internet means that’s always available now.
So, we jitter around like squirrels, hopping from one to the next to the next.
A strength of this book is where it goes from there. Specifically, what evidence-based practices will actually keep our squirrel-brain focused… and which are wishful thinking for anyone who lives in this century.
Bringing original research from their own labs, as well as studies taken from elsewhere, the authors present a science-based toolkit of genuinely useful resources for actual focus.
Bottom line: if you think you could really optimize your life if you could just get on track and stay on track, this is the book for you.
Click here to check out The Distracted Mind, and get yours to focus!
Share This Post
-

The “Yes I Can” Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sometimes, we are given to ask ourselves: “Can I produce a healthy and tasty salad out of what I have in?” and today we show how, with a well-stocked pantry, the answer is “yes I can”, regardless of what is (or isn’t) in the fridge.
You will need
- 1 can cannellini beans, drained
- 1 can sardines (if vegetarian/vegan, substitute ½ can chickpeas, drained)
- 1 can mandarin segments
- 1 handful pitted black olives, from a jar (or from a can, if you want to keep the “yes I can” theme going)
- ½ red onion, thinly sliced (this can be from frozen, defrosted—sliced/chopped onion is always a good thing to have in your freezer, by the way; your writer here always has 1–6 lbs of chopped onions in hers, divided into 1lb bags)
- 1 oz lemon juice
- 1 tbsp chopped parsley (this can be freeze-dried, but fresh is good if you have it)
- 1 tbsp extra virgin olive oil
- 1 tbsp chia seeds
- 1 tsp miso paste
- 1 tsp honey (omit if you don’t care for sweetness; substitute with agave nectar if you do like sweetness but don’t want to use honey specifically)
- 1 tsp red chili flakes
Method
(we suggest you read everything at least once before doing anything)
1) Combine the onion and the lemon juice in a small bowl, massaging gently
2) Mix (in another bowl) the miso paste with the chili flakes, chia seeds, honey, olive oil, and the spare juice from the can of mandarin segments, and whisk it to make a dressing.
3) Add the cannellini beans, sardines (break them into bite-size chunks), mandarin segments, olives, and parsley, tossing them thoroughly (but gently) in the dressing.
4) Top with the sliced onion, discarding the excess lemon juice, and serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Three Daily Servings of Beans?
- We Are Such Stuff As Fish Are Made Of
- Chia: The Tiniest Seeds With The Most Value
Take care!
Share This Post


Related Posts
-

The Exercises That Can Fix Sinus Problems (And More)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Who nose what benefits you will gain today?

This is James Nestor, a science journalist and author. He’s written for many publications, including Scientific American, and written a number of books, most notably Breath: The New Science Of A Lost Art.
Today we’ll be looking at what he has to share about what has gone wrong with our breathing, what problems this causes, and how to fix it.
What has gone wrong?
When it comes to breathing, we humans are the pugs of the primate world. In a way, we have the opposite problem to the squashed-faced dogs, though. But, how and why?
When our ancestors learned first tenderize food, and later to cook it, this had two big effects:
- We could now get much more nutrition for much less hunting/gathering
- We now did not need to chew our food nearly so much
Getting much more nutrition for much less hunting/gathering is what allowed us to grow our brains so large—as a species, we have a singularly large brain-to-body size ratio.
Not needing to chew our food nearly so much, meanwhile, had even more effects… And these effects have become only more pronounced in recent decades with the rise of processed food making our food softer and softer.
It changed the shape of our jaw and cheekbones, just as the size of our brains taking up more space in our skull moved our breathing apparatus around. As a result, our nasal cavities are anatomically ridiculous, our sinuses are a crime against nature (not least of all because they drain backwards and get easily clogged), and our windpipes are very easily blocked and damaged due to the unique placement of our larynx; we’re the only species that has it there. It allowed us to develop speech, but at the cost of choking much more easily.
What problems does this cause?
Our (normal, to us) species-wide breathing problems have resulted in behavioral adaptations such as partial (or in some people’s cases, total or near-total) mouth-breathing. This in turn exacerbates the problems with our jaws and cheekbones, which in turn exacerbates the problems with our sinuses and nasal cavities in general.
Results include such very human-centric conditions as sleep apnea, as well as a tendency towards asthma, allergies, and autoimmune diseases. Improper breathing also brings about a rather sluggish metabolism for how many calories we consume.
How are we supposed to fix all that?!
First, close your mouth if you haven’t already, and breathe through your nose.
In and out.
Both are important, and unless you are engaging in peak exercise, both should be through your nose. If you’re not used to this, it may feel odd at first, but practice, and build up your breathing ability.
Six seconds in and six seconds out is a very good pace.
If you’re sitting doing a breathing exercise, also good is four seconds in, four seconds hold, four seconds out, four seconds hold, repeat.
But those frequent holds aren’t practical in general life, so: six seconds in, six seconds out.
Through your nose only.
This has benefits immediately, but there are other more long-term benefits from doing not just that, but also what has been called (by Nestor, amongst many others), “Mewing”, per the orthodontist, Dr. John Mew, who pioneered it.
How (and why) to “mew”:
Place your tongue against the roof of your mouth. It should be flat against the palate; you’re not touching it with the tip here; you’re creating a flat seal.
Note: if you were mouth-breathing, you will now be unable to breathe. So, important to make sure you can breathe adequately through your nose first.
This does two things:
- It obliges nose-breathing rather than mouth-breathing
- It creates a change in how the muscles of your face interact with the bones of your face
In a battle between muscle and bone, muscle will always win.
Aim to keep your tongue there as much as possible; make it your new best habit. If you’re not eating, talking, or otherwise using your tongue to do something, it should be flat against the roof of your mouth.
You don’t have to exert pressure; this isn’t an exercise regime. Think of it more as a postural exercise, just, inside your mouth.
Quick note: read the above line again, because it’s important. Doing it too hard could cause the opposite problems, and you don’t want that. You cannot rush this by doing it harder; it takes time and gentleness.
Why would we want to do that?
The result, over time, will tend to be much healthier breathing, better sinus health, freer airways, reduced or eliminated sleep apnea, and, as a bonus, what is generally considered a more attractive face in terms of bone structure. We’re talking more defined cheekbones, straighter teeth, and a better mouth position.
Want to learn more?
This is the “Mewing” technique that Nestor encourages us to try:
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Built to Move – by Kelly starrett & Juliet Starrett
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In our everyday lives, for most of us anyway, it’s not too important to be able to run a marathon or leg-press a car. Rather more important, however, are such things as:
- being able to get up from the floor comfortably
- reach something on a high shelf without twinging a shoulder
- being able to put our socks on without making a whole plan around this task
- get accidentally knocked by an energetic dog or child and not put our back out
- etc
Starrett and Starrett, of “becoming a supple leopard” fame, lay out for us how to make sure our mobility stays great. And, if it’s not already where it needs to be, how to get there.
The “ten essential habits” mentioned in the subtitle “ten essential habits to help you move freely and live fully”, in fact also come with ten tests. No, not in the sense of arduous trials, but rather, mobility tests.
For each test, it’s explained to us how to score it out of ten (this is an objective assessment, not subjective). It’s then explained how to “level up” whatever score we got, with different advices for different levels of mobility or immobility. And if we got a ten, then of course, we just build the appropriate recommended habit into our daily life, to keep it that way.
The writing style is casual throughout, and a strong point of the book is its very clear illustrations, too.
Bottom line: if you’d like to gain/maintain good mobility (at any age), this book gives a very reliable outline for doing so.
Click here to check out Built to Move, and take care of your body!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Leek vs Scallions – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing leek to scallions, we picked the leek.
Why?
In terms of macros, scallions might have a point: scallions have the lower glycemic index, thanks to leek having more carbs for the same amount of fiber. That said, leek already has a low glycemic index, so this is not a big deal.
When it comes to vitamins, leek has more of vitamins B1, B2, B3, B5, B6, B9, E, and choline, while scallions have more of vitamins A, C, and K. Noteworthily, a cup of chopped leek already provides the daily dose of vitamins A and K, and the difference in levels of vitamin C is minimal. All in all, an easy 8:3 win for leeks here, even without taking that into account.
In the category of minerals, leek has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and selenium, while scallions have a little more zinc.
Both of these allium-family plants (i.e., related to garlic) have an abundance of polyphenols, especially kaempferol.
Of course, enjoy whatever goes best with your meal, but if you’re looking for nutritional density, then leek is where it’s at.
Want to learn more?
You might like to read:
The Many Health Benefits Of Garlic
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: