Sun-dried Tomatoes vs Black Olives – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sun-dried tomatoes to black olives, we picked the sun-dried tomatoes.
Why?
These common snack-salad items may seem similar in consistency, but their macros are very different: the tomatoes, being dried, have proportionally a lot more protein, carbs, and fiber. The olives, meanwhile, have more fat (and/but yes, a very healthy blend of fats). Note that these comments are true for the things themselves; be aware that sun-dried tomatoes are often sold in vegetable oil, which would obviously change the macros considerably and be much less healthy. So, for the sake of statistics, we’re assuming you got sun-dried tomatoes that aren’t soaked in oil. All in all, we’re calling this category a win for the tomatoes, but those fats from the olives are very good too.
In terms of vitamins, the sun-dried tomatoes being dried again means that the loss of water weight means the vitamin content is proportionally much higher; the tomatoes are higher in vitamins A, B1, B2, B3, B5, B6, B9, C, and K, while olives are higher only in vitamin E (but in their defence, olives have 165x more vitamin E than sun-dried tomatoes). Still, a win for sun-dried tomatoes here.
When it comes to minerals, it’s a similar story for the same reason; the loss of water weight in the sun-dried tomatoes makes them much more nutritionally dense; they are higher in calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while the olives are higher only in sodium. Note, we’re looking at black olives today; green olives would be even higher in sodium than black ones, as they are “cured” for longer.
Lastly, in terms of polyphenols, they both have a lot of great things to bring, but sun-dried tomatoes are pretty much the richest natural source of lycopene, which itself a very powerful polyphenol even my general polyphenol standards, so we’d call this one a win for the sun-dried tomatoes too.
Want to learn more?
You might like to read:
Lycopene’s Benefits For The Gut, Heart, Brain, & More
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Who Screens The Sunscreens?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We Screen The Sunscreens!

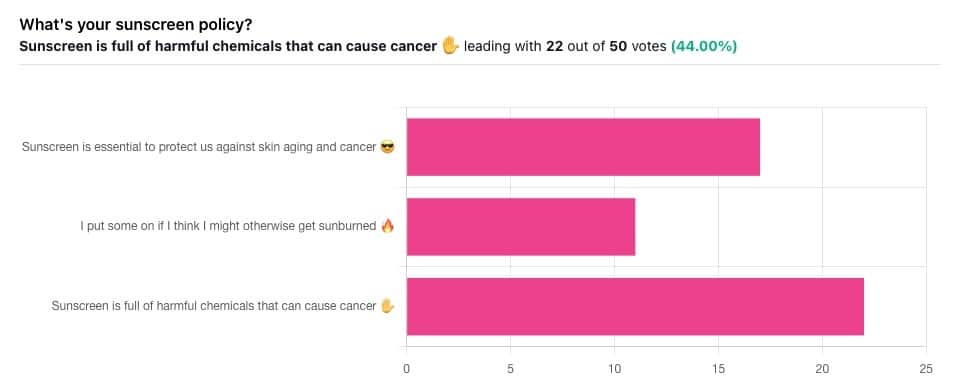
Yesterday, we asked you what your sunscreen policy was, and got a spread of answers. Apparently this one was quite polarizing!
One subscriber who voted for “Sunscreen is essential to protect us against skin aging and cancer” wrote:
❝My mom died of complications from melanoma, so we are vigilant about sun and sunscreen. We are a family of campers and hikers and gardeners—outdoors in all seasons—and we never burn❞
Our condolences with regard to your mom! Life is so precious, and when something like that happens, it tends to stick with us. We’re glad you and your family are taking care of yourselves.
Of the subscribers who voted for “I put some on if I think I might otherwise get sunburned”, about half wrote to express uncertainties:
- uncertainty about how safe it is, and
- uncertainty about how helpful it is
…so we’re going to tackle those questions in a moment. But what of those who voted for “Sunscreen is full of harmful chemicals that can cause cancer”?
Of those, only one wrote a message, which was to say one has to be very careful of what is in the formula.
Let’s take a look, then…
Sunscreen is full of harmful chemicals that can cause cancer: True or False?
False—according to current best science. Research is ongoing!
There are four main chemicals (found in most sunscreens) that people tend to worry about:
- Abobenzone
- Oxybenzone
- Octocrylene
- Ecamsule
Now, these two sound like four brands of rocket fuel, but then, dihydrogen monoxide (DHMO), which is also found in most sunscreens, sounds like a deadly toxin too. That’s water, by the way.
But what of these four chemicals? Well, as we say, research is ongoing, but we found a study that measured all four, to see how much got into the blood, and what adverse effects, if any, this caused.
We’ll skip to their conclusion:
❝In this preliminary study involving healthy volunteers, application of 4 commercially available sunscreens under maximal use conditions resulted in plasma concentrations that exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens. The systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings. These results do not indicate that individuals should refrain from the use of sunscreen.❞
Now, “exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens” sounds alarming, so why did they close with the words “These results do not indicate that individuals should refrain from the use of sunscreen”?
Let’s skip back up to a line from the results:
❝The most common adverse event was rash, which developed in 1 participant with each sunscreen.❞
This was most probably due to the oxybenzone, which can cause allergic skin reactions in some people.
Let us take a moment to remember the most common adverse event that occurs from not wearing sunscreen: sunburn!
You can read the full study here:
None of those ingredients have been found to be carcinogenic, even at the maximal blood plasma concentrations studied, from applications 4x/day to 75% of the body.
UVA rays, on the other hand, are absolutely very much known to cause cancer, and the effect is cumulative.
Sunscreen is essential to protect us against skin aging and cancer: True or False?
True, unequivocally, unless we live indoors and/or otherwise never go about under sunlight.
“But our ancestors—” lived under the same sun we do, and either used sunscreen or got advanced skin aging and cancer.
Sunscreen of times past ranged from mud to mineral lotions, but it’s pretty much always existed. Even non-human animals that have skin and don’t have fur or feathers, tend to take mud-baths in sunny parts of the world.
If you’d like to avoid oxybenzone and other chemicals, though, you might have your reasons. Maybe you’re allergic, or maybe you read that it’s a potential endocrine disruptor with estrogen-like and anti-androgenic properties that you don’t want.
There are other options, to include physical blockers containing zinc and titanium dioxide, which are generally recognized as safe and effective ingredients.
If you’re interested, you can even make your own sunscreen that blocks both UVA and UVB rays (UVA is what causes skin cancer; UVB is “milder” and is what causes sunburn):
Share This Post
-

Applesauce vs Cranberry Sauce – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing applesauce to cranberry sauce, we picked the applesauce.
Why?
It mostly comes down to the fact that apples are sweeter than cranberries:
In terms of macros, they are both equal on fiber (both languishing at a paltry 1.1g/100g), and/but cranberry sauce has 4x the carbs, of which, more than 3x the sugar. Simply, cranberry sauce recipes invariably have a lot of added sugar, while applesauce recipes don’t need that. So this is a huge relative win for applesauce (we say “relative” because it’s still not great, but cranberry sauce is far worse).
In the category of vitamins, applesauce has more of vitamins B1, B2, B5, B6, B9, and C, while cranberry sauce has more of vitamins E, K, and choline. A more moderate win for applesauce this time.
When it comes to minerals, applesauce has more calcium, copper, magnesium, phosphorus, and potassium, while cranberry sauce has more iron, manganese, and selenium. Another moderate win for applesauce.
Since we’ve discussed relative amounts rather than actual quantities, it’s worth noting that neither sauce is a good source of vitamins or minerals, and neither are close to just eating the actual fruits. Just, cranberry sauce is the relatively more barren of the two.
While cranberries famously have some UTI-fighting properties, you cannot usefully gain this benefit from a sauce that (with its very high sugar content and minimal fiber) actively feeds the very C. albicans you are likely trying to kill.
All in all, a pitiful show of nutritional inadequacy from these two products today, but one is relatively less bad than the other, and that’s the applesauce.
Want to learn more?
You might like to read:
From Apples to Bees, and High-Fructose Cs: Which Sugars Are Healthier, And Which Are Just The Same?
Enjoy!
Share This Post
-
Beetroot vs Red Cabbage – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing beetroot to red cabbage, we picked the red cabbage.
Why?
Both are great, and both have their strengths!
In terms of macros, beetroot has very slightly more protein, carbs, and fiber, but the margins of difference are very small in each case. However, in terms of glycemic index, red cabbage has the considerably lower glycemic index, of 32 (low) as opposed to beetroot’s GI of 64 (medium). On the strength of this GI difference, we call this category a win for red cabbage.
In the category of vitamins, beetroot has more of vitamin B9, while red cabbage has a lot more of vitamins A, B1, B2, B3, B6, C, E, K, and choline. By strength of numbers and also by having very large margins of difference on most of those, red cabbage is the clear winner here.
When it comes to minerals, beetroot has more copper, magnesium, manganese, phosphorus, and potassium, while red cabbage has more calcium (and about ⅓ of the sodium). By the numbers, this is a win for beetroot, though it’s worth noting that the margins of difference were small, i.e. red cabbage was right behind beetroot on each of those.
Adding up the sections makes for an overall red cabbage win, but as we say, beetroot is great too, especially when it comes to minerals!
As ever, enjoy either or both; diversity is good.
Want to learn more?
You might like to read:
No, beetroot isn’t vegetable Viagra. But here’s what it can do!
Enjoy!
Share This Post
Related Posts
-

The Whole Heart Solution – by Dr. Joel Kahn
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If there’s a single central focus here is on the evidence for including a lot of plants in our diet, and in particular, certain ones that are particularly impactful (positively) for our health. However, it’s not all about diet; Dr. Kahn also discusses (as the subtitle suggests) making the most of every safe, useful tool available for us for good heart health. Including, where appropriate, drugs and surgery, but definitely with a preference to avoid their necessity with lifestyle adjustments and regular pre-emptive testing of various kinds.
Indeed, the promised “75 low-cost things you can do right away” are mostly lifestyle adjustments, and as well as the dietary tips, they include non-dietary things such as opening your windows and walking barefoot, for example—we’ll learn tips relating to all areas of life, in fact.
An interesting note on diet, though: he also talks about how all requests for reimbursement for Medicare and Medicaid services are evaluated with regard to whether they are appropriate, and of all the programs for intensive cardiac rehabilitation that have been requested, only two have been approved (at time of going to press, at least). Both are plan-based programs, of which, one is the dietary approach described in this book. Bearing in mind that Medicare and Medicate have a mandate to save money, they will only approve a program that results in costing them less in hospital care and prescriptions. Which means that their interests are aligned with yours, in this case!
The style is enthusiastic pop science, that is to say, it is written with extreme conviction—there is plenty of science cited to back it up, of course, but certainly this is not an indifferent book.
Bottom line: if you’d like to improve your heart health, this book is a top-tier one-stop solution (if you implement its contents, anyway!)
Click here to check out the Whole Heart Solution, and live wholeheartedly!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Good (Or Bad) Health Starts With Your Blood
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Blood Should Be Only Slightly Thicker Than Water

This is Dr. Casey Means, a physician, lecturer (mostly at Stanford), and CMO of a metabolic health company, Levels, as well as being Associate Editor of the International Journal of Diabetes Reversal and Prevention, where she serves alongside such names as Dr. Colin Campbell, Dr. Joel Fuhrman, Dr. Michael Greger, Dr. William Li, Dr. Dean Ornish, and you get the idea: it’s a star-studded cast.
What does she want us to know?
The big blood problem:
❝We’re spending 3.8 trillion dollars a year on healthcare costs in the U.S., and the reality is that people are getting sicker, fatter, and more depressed.
Over 50% of Americans have pre-diabetes or type 2 diabetes; it’s insane, that number should be close to zero.❞
~ Dr. Casey Means
Indeed, pre-diabetes and especially type 2 diabetes should be very avoidable in any wealthy nation.
Unfortunately, the kind of diet that avoids it tends to rely on having at least 2/3 of the following:
- Money
- Time
- Knowledge
For example:
- if you have money and time, you can buy lots of fresh ingredients without undue worry, and take the time to carefully prep and cook them
- if you have money and knowledge you can have someone else shop and cook for you, or at least get meal kits delivered
- if you have time and knowledge, you can actually eat very healthily on a shoestring budget
If you have all three, then the world’s your oyster mushroom steak sautéed in extra virgin olive oil with garlic and cracked black pepper served on a bed of Swiss chard and lashed with Balsamic vinegar.
However, many Americans aren’t in the happy position of having at least 2/3, and a not-insignificant portion of the population don’t even have 1/3.
As an aside: there is a food scientist and chef who’s made it her mission to educate people about food that’s cheap, easy, and healthy:
…but today is about Dr. Means, so, what does she suggest?
Know
thyselfthy blood sugarsDr. Means argues (reasonably; this is well-backed up by general scientific consensus) that much of human disease stems from the diabetes and pre-diabetes that she mentioned above, and so we should focus on that most of all.
Our blood sugar levels being unhealthy will swiftly lead to other metabolic disorders:
Heart disease and non-alcoholic fatty liver disease are perhaps first in line, but waiting in the wings are inflammation-mediated autoimmune disorders, and even dementia, because neuroinflammation is at least as bad as inflammation anywhere else, arguably worse, and our brain can only be as healthy as the blood that feeds it and takes things that shouldn’t be there away.
Indeed,
❝Alzheimer’s dementia is now being called type 3 diabetes because it’s so related to blood sugar❞
~ Dr. Casey Means
…which sounds like a bold claim, but it’s true, even if the name is not “official” yet, it’s well-established in professional circulation:
❝We conclude that the term “type 3 diabetes” accurately reflects the fact that AD represents a form of diabetes that selectively involves the brain and has molecular and biochemical features that overlap with both T1DM and T2DM❞
~ Dr. Suzanne M. de la Monte & Dr. Jack Wands
Read in full: Alzheimer’s Disease Is Type 3 Diabetes–Evidence Reviewed ← this is from the very respectable Journal of Diabetes Science and Technology.
What to do about it
Dr. Means suggests we avoid the “glucose roller-coaster” that most Americans are on, meaning dramatic sugar spikes, or to put it in sciencese: high glycemic variability.
This leads to inflammation, oxidative stress, glycation (where sugar sticks to proteins and DNA), and metabolic dysfunction. Then there’s the flipside: reactive hypoglycemia, a result of a rapid drop in blood sugar after a spike, can cause anxiety, fatigue, weakness/trembling, brain fog, and of course cravings. And so the cycle repeats.
But it doesn’t have to!
By taking it upon ourselves to learn about what causes our blood sugars to rise suddenly or gently, we can manage our diet and other lifestyle factors accordingly.
And yes, it’s not just about diet, Dr. Means tells us. While added sugar and refined carbohydrates or indeed the main drivers of glycemic variability, our sleep, movement, stress management, and even toxin exposure play important parts too.
One way to do this, that Dr. Means recommends, is with a continuous glucose monitor:
Track Your Blood Sugars For Better Personalized Health
Another way is to just apply principles that work for almost everyone:
10 Ways To Balance Blood Sugars
Want to know more from Dr. Means?
You might like her book:
Good Energy – by Dr. Casey Means
…which goes into this in far more detail than we have room to today.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Their First Baby Came With Medical Debt. These Illinois Parents Won’t Have Another.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
JACKSONVILLE, Ill. — Heather Crivilare was a month from her due date when she was rushed to an operating room for an emergency cesarean section.
The first-time mother, a high school teacher in rural Illinois, had developed high blood pressure, a sometimes life-threatening condition in pregnancy that prompted doctors to hospitalize her. Then Crivilare’s blood pressure spiked, and the baby’s heart rate dropped. “It was terrifying,” Crivilare said.
She gave birth to a healthy daughter. What followed, though, was another ordeal: thousands of dollars in medical debt that sent Crivilare and her husband scrambling for nearly a year to keep collectors at bay.
The Crivilares would eventually get on nine payment plans as they juggled close to $5,000 in bills.
“It really felt like a full-time job some days,” Crivilare recalled. “Getting the baby down to sleep and then getting on the phone. I’d set up one payment plan, and then a new bill would come that afternoon. And I’d have to set up another one.”
Crivilare’s pregnancy may have been more dramatic than most. But for millions of new parents, medical debt is now as much a hallmark of having children as long nights and dirty diapers.
About 12% of the 100 million U.S. adults with health care debt attribute at least some of it to pregnancy or childbirth, according to a KFF poll.
These people are more likely to report they’ve had to take on extra work, change their living situation, or make other sacrifices.
Overall, women between 18 and 35 who have had a baby in the past year and a half are twice as likely to have medical debt as women of the same age who haven’t given birth recently, other KFF research conducted for this project found.
“You feel bad for the patient because you know that they want the best for their pregnancy,” said Eilean Attwood, a Rhode Island OB-GYN who said she routinely sees pregnant women anxious about going into debt.
“So often, they may be coming to the office or the hospital with preexisting debt from school, from other financial pressures of starting adult life,” Attwood said. “They are having to make real choices, and what those real choices may entail can include the choice to not get certain services or medications or what may be needed for the care of themselves or their fetus.”
Best-Laid Plans
Crivilare and her husband, Andrew, also a teacher, anticipated some of the costs.
The young couple settled in Jacksonville, in part because the farming community less than two hours north of St. Louis was the kind of place two public school teachers could afford a house. They saved aggressively. They bought life insurance.
And before Crivilare got pregnant in 2021, they enrolled in the most robust health insurance plan they could, paying higher premiums to minimize their deductible and out-of-pocket costs.
Then, two months before their baby was due, Crivilare learned she had developed preeclampsia. Her pregnancy would no longer be routine. Crivilare was put on blood pressure medication, and doctors at the local hospital recommended bed rest at a larger medical center in Springfield, about 35 miles away.
“I remember thinking when they insisted that I ride an ambulance from Jacksonville to Springfield … ‘I’m never going to financially recover from this,’” she said. “‘But I want my baby to be OK.’”
For weeks, Crivilare remained in the hospital alone as covid protocols limited visitors. Meanwhile, doctors steadily upped her medications while monitoring the fetus. It was, she said, “the scariest month of my life.”
Fear turned to relief after her daughter, Rita, was born. The baby was small and had to spend nearly two weeks in the neonatal intensive care unit. But there were no complications. “We were incredibly lucky,” Crivilare said.
When she and Rita finally came home, a stack of medical bills awaited. One was already past due.
Crivilare rushed to set up payment plans with the hospitals in Jacksonville and Springfield, as well as the anesthesiologist, the surgeon, and the labs. Some providers demanded hundreds of dollars a month. Some settled for monthly payments of $20 or $25. Some pushed Crivilare to apply for new credit cards to pay the bills.
“It was a blur of just being on the phone constantly with all the different people collecting money,” she recalled. “That was a nightmare.”
Big Bills, Big Consequences
The Crivilares’ bills weren’t unusual. Parents with private health coverage now face on average more than $3,000 in medical bills related to a pregnancy and childbirth that aren’t covered by insurance, researchers at the University of Michigan found.
Out-of-pocket costs are even higher for families with a newborn who needs to stay in a neonatal ICU, averaging $5,000. And for 1 in 11 of these families, medical bills related to pregnancy and childbirth exceed $10,000, the researchers found.
“This forces very difficult trade-offs for families,” said Michelle Moniz, a University of Michigan OB-GYN who worked on the study. “Even though they have insurance, they still have these very high bills.”
Nationwide polls suggest millions of these families end up in debt, with sometimes devastating consequences.
About three-quarters of U.S. adults with debt related to pregnancy or childbirth have cut spending on food, clothing, or other essentials, KFF polling found.
About half have put off buying a home or delayed their own or their children’s education.
These burdens have spurred calls to limit what families must pay out-of-pocket for medical care related to pregnancy and childbirth.
In Massachusetts, state Sen. Cindy Friedman has proposed legislation to exempt all these bills from copays, deductibles, and other cost sharing. This would parallel federal rules that require health plans to cover recommended preventive services like annual physicals without cost sharing for patients. “We want … healthy children, and that starts with healthy mothers,” Friedman said. Massachusetts health insurers have warned the proposal will raise costs, but an independent state analysis estimated the bill would add only $1.24 to monthly insurance premiums.
Tough Lessons
For her part, Crivilare said she wishes new parents could catch their breath before paying down medical debt.
“No one is in the right frame of mind to deal with that when they have a new baby,” she said, noting that college graduates get such a break. “When I graduated with my college degree, it was like: ‘Hey, new adult, it’s going to take you six months to kind of figure out your life, so we’ll give you this six-month grace period before your student loans kick in and you can get a job.’”
Rita is now 2. The family scraped by on their payment plans, retiring the medical debt within a year, with help from Crivilare’s side job selling resources for teachers online.
But they are now back in debt, after Rita’s recurrent ear infections required surgery last year, leaving the family with thousands of dollars in new medical bills.
Crivilare said the stress has made her think twice about seeing a doctor, even for Rita. And, she added, she and her husband have decided their family is complete.
“It’s not for us to have another child,” she said. “I just hope that we can put some of these big bills behind us and give [Rita] the life that we want to give her.”
About This Project
“Diagnosis: Debt” is a reporting partnership between KFF Health News and NPR exploring the scale, impact, and causes of medical debt in America.
The series draws on original polling by KFF, court records, federal data on hospital finances, contracts obtained through public records requests, data on international health systems, and a yearlong investigation into the financial assistance and collection policies of more than 500 hospitals across the country.
Additional research was conducted by the Urban Institute, which analyzed credit bureau and other demographic data on poverty, race, and health status for KFF Health News to explore where medical debt is concentrated in the U.S. and what factors are associated with high debt levels.
The JPMorgan Chase Institute analyzed records from a sampling of Chase credit card holders to look at how customers’ balances may be affected by major medical expenses. And the CED Project, a Denver nonprofit, worked with KFF Health News on a survey of its clients to explore links between medical debt and housing instability.
KFF Health News journalists worked with KFF public opinion researchers to design and analyze the “KFF Health Care Debt Survey.” The survey was conducted Feb. 25 through March 20, 2022, online and via telephone, in English and Spanish, among a nationally representative sample of 2,375 U.S. adults, including 1,292 adults with current health care debt and 382 adults who had health care debt in the past five years. The margin of sampling error is plus or minus 3 percentage points for the full sample and 3 percentage points for those with current debt. For results based on subgroups, the margin of sampling error may be higher.
Reporters from KFF Health News and NPR also conducted hundreds of interviews with patients across the country; spoke with physicians, health industry leaders, consumer advocates, debt lawyers, and researchers; and reviewed scores of studies and surveys about medical debt.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: