Make Social Media Work For Your Mental Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Social Media, But Healthy
Social media has a bad reputation, and rightly so. It’s calculated to trick you into doomscrolling and rage-posting, and it encourages you to compare your everyday life to other people’s carefully-curated highlight reels.
Rebalancing Dopamine (Without “Dopamine Fasting”)
But it doesn’t have to be so.
Find your community
One of the biggest strengths social media has going for it is that it can, if used well, be a powerful tool for community. As for why that’s important from a health perspective, see:
How To Beat Loneliness & Isolation
Loneliness & isolation do, of course, kill people. By:
- Accidents, e.g. household fall but nobody notices for a week
- Depression and resultant decline (and perhaps even active suicidality)
- Cognitive decline from a lack of social contact
Read more:
- The Mental Health First-Aid That You’ll Hopefully Never Need
- How To Stay Alive (When You Really Don’t Want To)
- The Five Key Traits Of Healthy Aging
So, what’s “community” to you, and to what extent can you find it online? Examples might include:
- A church, or other religious community, if we be religious
- The LGBT+ community, or even just a part of it, if that fits for us
- Any mutual-support oriented, we-have-this-shared-experience community, could be anything from AA to the VA.
Find your people, and surround yourself with them. There are more than 8,000,000,000 people on this planet, you will not find all the most compatible ones with you on your street.
Grow & nurture your community
Chances are, you have a lot to contribute. Your life experiences are valuable.
Being of service to other people is strongly associated “flourishing”, per the science.
Indeed, one of the questions on the subjective wellness scale test is to ask how much one agrees with the statement “I actively contribute to the happiness and wellbeing of others”.
See: Are You Flourishing? (There’s a Scale)
So, help people, share your insights, create whatever is relevant to your community and fits your skills (it could be anything from art to tutorials to call-to-action posts or whatever works for you and your community)
As a bonus: when people notice you are there for them, they’ll probably be there for you, too. Not always, sadly, but there is undeniable strength in numbers.
Remember it’s not the boss of you
Whatever social media platform(s) you use, the companies in question will want you to use it in the way that is most profitable for them.
Usually that means creating a lot of shallow content, clicking on as many things as possible, and never logging off.
Good ways to guard against that include:
- Use the social media from a computer rather than a handheld device
- Disable “infinite scroll” in the settings, if possible
- Set a timer and stick to it
- Try to keep your interactions to only those that are relevant and kind (for the good of your own health, let alone anyone else’s)
On that latter note…
Before posting, ask “what am I trying to achieve here?” and ensure your action is aligned with your actual desires, and not just reactivity. See also:
A Bone To Pick… Up And Then Put Back Where We Found It
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Potatoes & Anxiety

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝My other half considers potatoes a wonder food, except when fried. I don’t. I find, when I am eating potatoes I put on weight; and, when I’m not eating them, I lose it. Also, although I can’t swear to it, potatoes also make me feel a little anxious (someone once told me it could have something to do with where they are on the “glycemic index”). What does the science say?❞
The glycemic index of potatoes depends on the kind of potato (obviously) and also, less obviously, how it’s prepared. For a given white potato, boiling (which removes a lot of starch) might produce a GI of around 60, while instant mash (basically: potato starch) can be more like 80. For reference, pure glucose is 100. And you probably wouldn’t take that in the same quantity you’d take potato, and expect to feel good!
So: as for anxiety, it could be, since spiked blood sugars can cause mood swings, including anxiety.
Outside of the matter of blood sugars, the only reference we could find for potatoes causing anxiety was fried potatoes specifically:
❝frequent fried food consumption, especially fried potato consumption, is strongly associated with 12% and 7% higher risk of anxiety and depression, respectively❞
…which heavily puts the blame not on the potatoes themselves, but on acrylamide (the orange/brown stuff that is made by the Maillard reaction of cooking starches in the absence of water, e.g. by frying, roasting, etc).
Here’s a very good overview of that, by the way:
A Review on Acrylamide in Food: Occurrence, Toxicity, and Mitigation Strategies
Back on the core topic of potatoes and GI and blood sugar spikes and anxiety, you might benefit from a few tweaks that will allow you to enjoy potatoes without spiking blood sugars:
10 Ways To Balance Blood Sugars
Enjoy!
Share This Post
-
How stigma perpetuates substance use
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In 2022, 54.6 million people 12 and older in the United States needed substance use disorder (SUD) treatment. Of those, only 24 percent received treatment, according to the most recent National Survey on Drug Use and Health.
SUD is a treatable, chronic medical condition that causes people to have difficulty controlling their use of legal or illegal substances, such as alcohol, tobacco, prescription opioids, heroin, methamphetamine, or cocaine. Using these substances may impact people’s health and ability to function in their daily life.
While help is available for people with SUD, the stigma they face—negative attitudes, stereotypes, and discrimination—often leads to shame, worsens their condition, and keeps them from seeking help.
Read on to find out more about how stigma perpetuates substance use.
Stigma can keep people from seeking treatment
Suzan M. Walters, assistant professor at New York University’s Grossman School of Medicine, has seen this firsthand in her research on stigma and health disparities.
She explains that people with SUD may be treated differently at a hospital or another health care setting because of their drug use, appearance (including track marks on their arms), or housing situation, which may discourage them from seeking care.
“And this is not just one case; this is a trend that I’m seeing with people who use drugs,” Walters tells PGN. “Someone said, ‘If I overdose, I’m not even going to the [emergency room] to get help because of this, because of the way I’m treated. Because I know I’m going to be treated differently.’”
People experience stigma not only because of their addiction, but also because of other aspects of their identities, Walters says, including “immigration or race and ethnicity. Hispanic folks, brown folks, Black folks [are] being treated differently and experiencing different outcomes.”
And despite the effective harm reduction tools and treatment options available for SUD, research has shown that stigma creates barriers to access.
Syringe services programs, for example, provide infectious disease testing, Narcan, and fentanyl test strips. These programs have been proven to save lives and reduce the spread of HIV and hepatitis C. SSPs don’t increase crime, but they’re often mistakenly “viewed by communities as potential settings of drug-related crime;” this myth persists despite decades of research proving that SSPs make communities safer.
To improve this bias, Walters says it’s helpful for people to take a step back and recognize how we use substances, like alcohol, in our own lives, while also humanizing those with addiction. She says, “There’s a lack of understanding that these are human beings and people … [who] are living lives, and many times very functional lives.”
Misconceptions lead to stigma
SUD results from changes in the brain that make it difficult for a person to stop using a substance. But research has shown that a big misconception that leads to stigma is that addiction is a choice and reflects a person’s willpower.
Michelle Maloney, executive clinical director of mental health and addiction recovery services for Rogers Behavioral Health, tells PGN that statements such as “you should be able to stop” can keep a patient from seeking treatment. This belief goes back to the 1980s and the War on Drugs, she adds.
“We think about public service announcements that occurred during that time: ‘Just say no to drugs,’” Maloney says. “People who have struggled, whether that be with nicotine, alcohol, or opioids, [know] it’s not as easy as just saying no.”
Stigma can worsen addiction
Stigma can also lead people with SUD to feel guilt and shame and blame themselves for their medical condition. These feelings, according to the National Institute on Drug Abuse, may “reinforce drug-seeking behavior.”
In a 2020 article, Dr. Nora D. Volkow, the director of NIDA, said that “when internalized, stigma and the painful isolation it produces encourage further drug taking, directly exacerbating the disease.”
Overall, research agrees that stigma harms people experiencing addiction and can make the condition worse. Experts also agree that debunking myths about the condition and using non-stigmatizing language (like saying someone is a person with a substance use disorder, not an addict) can go a long way toward reducing stigma.
Resources to mitigate stigma:
- CDC: Stigma Reduction
- National Harm Reduction Coalition: Respect To Connect: Undoing Stigma
- NIDA:
- Shatterproof: Addiction language guide (Disclosure: The Public Good Projects, PGN’s parent company, is a Shatterproof partner)
This article first appeared on Public Good News and is republished here under a Creative Commons license.

Share This Post
-

Body by Science – by Dr. Doug McGuff & John Little
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The idea that you’ll get a re-sculpted body at 12 minutes per week is a bold claim, isn’t it? Medical Doctor Doug McGuff and bodybuilder John Little team up to lay out their case. So, how does it stand up to scrutiny?
First, is it “backed by rigorous research” as claimed? Yes… with caveats.
The book uses a large body of scientific literature as its foundation, and that weight of evidence does support this general approach:
- Endurance cardio isn’t very good at burning fat
- Muscle, even just having it without using it much, burns fat to maintain it
- To that end, muscle can be viewed as a fat-burning asset
- Muscle can be grown quickly with short bursts of intense exercise once per week
Why once per week? The most relevant muscle fibers take about that long to recover, so doing it more often will undercut gains.
So, what are the caveats?
The authors argue for slow reps of maximally heavy resistance work sufficient to cause failure in about 90 seconds. However, most of the studies cited for the benefits of “brief intense exercise” are for High Intensity Interval Training (HIIT). HIIT involves “sprints” of exercise. It doesn’t have to be literally running, but for example maxing out on an exercise bike for 30 seconds, slowing for 60, maxing out for 30, etc. Or in the case of resistance work, explosive (fast!) concentric movements and slow eccentric movements, to work fast- and slow-twitch muscle fibers, respectively.
What does this mean for the usefulness of the book?
- Will it sculpt your body as described in the blurb? Yes, this will indeed grow your muscles with a minimal expenditure of time
- Will it improve your body’s fat-burning metabolism? Yes, this will indeed turn your body into a fat-burning machine
- Will it improve your “complete fitness”? No, if you want to be an all-rounder athlete, you will still need HIIT, as otherwise anything taxing your under-worked fast-twitch muscle fibers will exhaust you quickly.
Bottom line: read this book if you want to build muscle efficiently, and make your body more efficient at burning fat. Best supplemented with at least some cardio, though!
Click here to check out Body by Science, and get re-sculpting yours!
Share This Post

Related Posts
-

Can Saturated Fats Be Healthy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Saturated Fat: What’s The Truth?

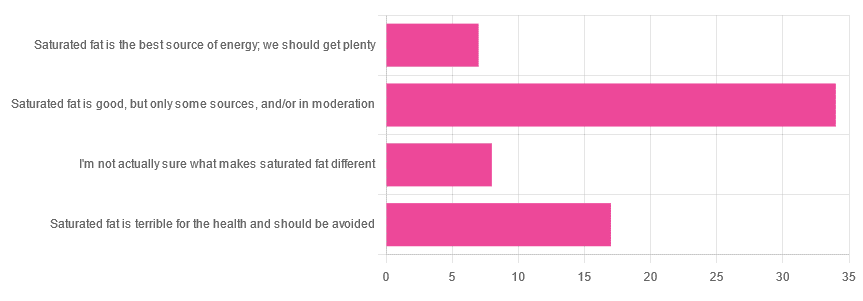
We asked you for your health-related opinion of saturated fat, and got the above-pictured, below-described, set of results.
- Most recorded votes were for “Saturated fat is good, but only some sources, and/or in moderation”
- This is an easy one to vote for, because of the “and/or in moderation” part, which tends to be a “safe bet” for most things.
- Next most popular was “Saturated fat is terrible for the health and should be avoided”
- About half as many recorded votes were for “I’m not actually sure what makes saturated fat different”, which is a very laudable option to click. Admitting when we don’t know things (and none of us know everything) is a very good first step to learning about them!
- Fewest recorded votes were for “Saturated fat is the best source of energy; we should get plenty”.
So, what does the science say?
First, a bit of physics, chemistry, and biology
You may be wondering what, exactly, saturated fats are “saturated” with. That’s a fair question, so…
All fats have a molecular structure made up of carbon, hydrogen, and oxygen atoms. Saturated fats are saturated with hydrogen, and thus have only single bonds between carbon atoms (unsaturated fats have at least one double-bond between carbon atoms).
The observable effect this has on them, is that fats that are saturated with hydrogen are solid at room temperature, whereas unsaturated fats are liquid at room temperature. Their different properties also make for different interactions inside the human body, including how likely or not they are to (for example) clog arteries.
See also: Could fat in your bloodstream cause blood clots?
Saturated fat is the best source of energy; we should get plenty: True or False?
False, in any reasonable interpretation, anyway. That is to say, if your idea of “plenty” is under 13g (e.g: two tablespoons of butter, and no saturated fat from other sources, e.g. meat) per day, then yes, by all means feel free to eat plenty. More than that, though, and you might want to consider trimming it down a bit.
The American Heart Association has this to say:
❝When you hear about the latest “diet of the day” or a new or odd-sounding theory about food, consider the source.
The American Heart Association recommends limiting saturated fats, which are found in butter, cheese, red meat and other animal-based foods, and tropical oils.
Decades of sound science has proven it can raise your “bad” cholesterol and put you at higher risk for heart disease.❞
Source: The American Heart Association Diet and Lifestyle Recommendations on Saturated Fat
The British Heart Foundation has a similar statement:
❝Despite what you read in the media, our advice is clear: replace saturated fats with unsaturated fats and avoid trans fats. Saturated fat is the kind of fat found in butter, lard, ghee, fatty meats and cheese. This is linked to an increased risk of heart and circulatory disease❞
Source: British Heart Foundation: What does fat do and what is saturated fat?
As for the World Health Organization:
❝1. WHO strongly recommends that adults and children reduce saturated fatty acid intake to 10% of total energy intake
2. WHO suggests further reducing saturated fatty acid intake to less than 10% of total energy intake
3. WHO strongly recommends replacing saturated fatty acids in the diet with polyunsaturated fatty acids; monounsaturated fatty acids from plant sources; or carbohydrates from foods containing naturally occurring dietary fibre, such as whole grains, vegetables, fruits and pulses.❞
Source: Saturated fatty acid and trans-fatty acid intake for adults and children: WHO guideline
Please note, organizations such as the AHA, the BHF, and the WHO are not trying to sell us anything, and just would like us to not die of heart disease, the world’s #1 killer.
As for “the best source of energy”…
We evolved to eat (much like our nearest primate cousins) a diet consisting mostly of fruits and other edible plants, with a small supplementary amount of animal-source protein and fats.
That’s not to say that because we evolved that way we have to eat that way—we are versatile omnivores. But for example, we are certainly not complete carnivores, and would quickly sicken and die if we tried to live on only meat and animal fat (we need more fiber, more carbohydrates, and many micronutrients that we usually get from plants)
The closest that humans tend to come to doing such is the ketogenic diet, which focuses on a high fat, low carbohydrate imbalance, to promote ketosis, in which the body burns fat for energy.
The ketogenic diet does work, and/but can cause a lot of health problems if a lot of care is not taken to avoid them.
See for example: 7 Keto Risks To Keep In Mind
Saturated fat is terrible for the health and should be avoided: True or False?
False, if we are talking about “completely”.
Firstly, it’s practically impossible to cut out all saturated fats, given that most dietary sources of fat are a mix of saturated, unsaturated (mono- and poly-), and trans fats (which are by far the worst, but beyond the scope of today’s main feature).
Secondly, a lot of research has been conducted and found insignificant or inconclusive results, in cases where saturated fat intake was already within acceptable levels (per the recommendations we mentioned earlier), and then cut down further.
Rather than fill up the newsletter with individual studies of this kind here’s a high-quality research review, looking at 19 meta-analyses, each of those meta-analyses having looked at many studies:
Dietary saturated fat and heart disease: a narrative review
Saturated fat is good, but only some sources, and/or in moderation: True or False?
True! The moderation part is easy to guess, so let’s take a look at the “but only some sources”.
We were not able to find any convincing science to argue for health-based reasons to favor plant- or animal-sourced saturated fat. However…
Not all saturated fats are created equal (there are many kinds), and also many of the foods containing them have additional nutrients, or harmful compounds, that make a big difference to overall health, when compared gram-for-gram in terms of containing the same amount of saturated fat.
For example:
- Palm oil’s saturated fat contains a disproportionate amount of palmitic acid, which raises LDL (“bad” cholesterol) without affecting HDL (“good” cholesterol), thus having an overall heart-harmful effect.
- Most animal fats contain a disproportionate amount of stearic acid, which has statistically insignificant effects on LDL and HDL levels, and thus is broadly considered “heart neutral” (in moderation!)
- Coconut oil’s saturated fat contains a disproportionate amount of lauric acid, which raises total cholesterol, but mostly HDL without affecting LDL, thus having an overall heart-beneficial effect (in moderation!)
Do you know what’s in the food you eat?
Test your knowledge with the BHF’s saturated fat quiz!
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
- Most recorded votes were for “Saturated fat is good, but only some sources, and/or in moderation”
-

Workout Advice For Busy People
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hampton at Hybrid Calisthenics always has very sound advice in his uplifting videos, and this one’s no exception:
Key tips for optimizing workouts without burning out
“We all have the same 24 hours” is a folly when in fact, some of us have more responsibilities and/or other impediments to getting things done (e.g. disabilities).
A quick word on disabilities first: sometimes people are quick to point out Paralympian athletes, and “if they can do it, so can you!” and forget that these people are in the top percentile of the top percentile of the top percentile of human performance. If you wouldn’t disparagingly say “if Simone Biles/Hussein Bolt/Michael Phelps can do it, so can you”, then don’t for Paralympians either 😉
Now, as for Hampton’s advice, he recommends:
Enjoy short, intense workouts:
- You can get effective results in under 30 minutes (or even just a few minutes per day) with compound exercises (e.g., squats, pull-ups).
- Focus on full-body movements also saves time!
- Push closer to failure when possible to maximize efficiency. It’s the last rep where most of the strength gains are made! Same deal with cardiovascular fitness, too. Nevertheless, do take safety into account in both cases, of course.
Time your rest periods:
- Resting for 2–3 minutes between sets ensures optimal recovery.
- Avoid getting distracted during rest by setting a timer to stay focused.
- 10almonds tip: use this time to practice a mindfulness meditation. That will greatly reduce the chance of you becoming distracted.
Remember holistic fitness:
- Fitness isn’t just about exercise; diet, sleep, and stress management are equally important for your fitness as much as for the rest of your health.
- Better sleep and reduced stress will help you exercise more consistently and avoid junk food.
Address burnout:
- If feeling too exhausted to apply these tips, focus on getting better rest and reducing stress first.
- Taking a short break to reset can help in the long run.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- How To Do High Intensity Interval Training (Without Wrecking Your Body)
- How To Rest More Efficiently (Yes, Really)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Love Sense – by Dr. Sue Johnson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Let’s quickly fact-check the subtitle:
- Is it revolutionary? It has a small element of controversy, but mostly no
- Is it new? No, it is based on science from the 70s that was expanded in the 80s and 90s and has been, at most, tweaked a little since.
- Is it science? Yes! It is so much science. This book comes with about a thousand references to scientific studies.
What’s the controversy, you ask? Dr. Johnson asserts, based on our (as a species) oxytocin responsiveness, that we are biologically hardwired for monogamy. This is in contrast to the prevailing scientific consensus that we are not.
Aside from that, though, the book is everything you could expect from an expert on attachment theory with more than 35 years of peer-reviewed clinical research, often specifically for Emotionally Focused Therapy (EFT), which is her thing.
The writing style is similar to that of her famous “Hold Me Tight: Seven Conversations For A Lifetime Of Love”, a very good book that we reviewed previously. It can be a little repetitive at times in its ideas, but this is largely because she revisits some of the same questions from many angles, with appropriate research to back up her advice.
Bottom line: if you are the sort of person who cares to keep working to improve your romantic relationship (no matter whether it is bad or acceptable or great right now), this book will arm you with a lot of deep science that can be applied reliably with good effect.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: