Severe irritability in teens can be reduced by daily doses of vitamins and minerals, new research
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Irritability is one of the most common and distressing problems teenagers and their families face.
Its main symptom is an excessive reaction to negative emotional stimuli, resulting in temper outbursts and severe irritable mood.
While current treatment options such as psychotherapy and medications are helpful for some, they can be inaccessible or poorly tolerated.
Our new research, based on a double-blinded, placebo-controlled clinical trial, shows broad-spectrum micronutrients (vitamins and minerals) can significantly reduce severe irritability in teenagers. Teens with severely disruptive behaviour experienced especially large improvements.
This offers a safe, scalable and biologically grounded alternative to conventional psychiatric treatments.

Urgent need for more effective treatments
Irritability cuts across many psychiatric presentations, including anxiety, depression, attention deficit/hyperactivity disorder (ADHD) and other disruptive behaviour disorders.
The need for interventions that directly target irritability, have fewer side effects and are available to all communities is urgent.
Statistics on mental health in young people are especially concerning. Youth mental health has been declining globally over the past two decades and has now reached a “dangerous phase”, according to a Lancet commission.
Despite this, research consistently highlights a lack of effective and accessible treatments for severely irritable youth. This suggests a significant unmet public health need.
Our research findings are based on the Balancing Emotions of Adolescents with Micronutrients (BEAM) trial, in which 132 unmedicated teenagers (aged 12 to 17) with moderate to severe irritability were randomly assigned to micronutrients (taken as four pills three times a day) or an active placebo for eight weeks. They were monitored monthly online by a clinical psychologist.
The placebo response was high, suggesting that simply participating in the study helped many teens feel able to improve their behaviour. But micronutrients still outperformed the placebo across key clinical measures such as irritability, emotional reactivity and overall improvement.
We saw the strongest effects in teenagers with disruptive mood dysregulation disorder (DMDD), with 64% responding to micronutrients compared to 12.5% on placebo. This demonstrates an unusually large effect for a psychiatric intervention.
Parents of participants receiving micronutrients rated the teens’ conduct and prosocial behaviour much higher compared with those of teens on placebo.
Micronutrient treatment was also associated with more rapid improvements in clinician‑rated irritability, parent‑reported dysphoria and teen‑reported quality of life, stress and prosocial behaviours.
One of the most notable and reassuring findings was that suicidal ideation, which about a quarter of study participants reported at the start of the trial, improved over time for both groups, but with a greater change for teens on micronutrients. Self-harm behaviour also decreased for both groups.
Only one side effect differed significantly between groups: diarrhoea was more common on micronutrients (20.9%) than placebo (6.2%). But this side effect was typically temporary and resolved by taking the nutrients with food and water.
A minority (fewer than 10%) found swallowing pills a challenge. Other side effects reported equally in both groups included occasional headaches, stomach aches or a dry mouth. These tended to dissipate within the first few weeks.
Socioeconomic background matters
The response to treatment was moderated by the teens’ socioeconomic status.
Participants from lower socioeconomic backgrounds were more likely to benefit from micronutrients. This is particularly meaningful for both clinical practice and public health.
Lower socioeconomic status is typically associated with greater exposure to nutritional insufficiencies, chronic stress, reduced access to health services and higher rates of mental health difficulties.
Our findings suggest micronutrients may help address underlying nutritional vulnerabilities that may be more prevalent or more severe in disadvantaged groups.
This pattern also indicates that micronutrient supplementation, if publicly funded, could function as a low‑cost, scalable intervention, with the potential to reduce health inequities.
Many evidence‑based psychosocial or pharmacological treatments require resources – time, transportation, specialist access – that disproportionately disadvantage lower‑income families.
In our trial, all meetings between the psychologist and the teen with their family were conducted online and the micronutrients were couriered across the country, making this intervention accessible, particularly to rural communities.
Micronutrients may represent an intervention that is both accessible and responsive to the specific needs of youth who are most at risk yet often least well served by traditional care pathways.
This study was developed alongside Māori health providers and fits within a tikanga (traditional) Māori framework. It had a high percentage of Māori participants (27%) and worked closely with them, their families and health providers to assist in improving mental health outcomes.
The BEAM trial provides robust evidence that a simple nutritional approach can meaningfully improve symptoms, including emotional reactivity, conduct difficulties and even suicidal ideation.
These results are relevant for parents, clinicians, teachers and policymakers seeking safe and practical interventions, especially for young people who cannot access or do not respond well to existing treatments. The results also highlight important equity implications, as teens from lower income families showed stronger responses.
Our results cast a new lens on the cause of some psychiatric problems, often conceptualised as chemical imbalances or family dysfunction. They reframe some cases of irritability as a possible nutritional and metabolic vulnerability, one that might be addressed with greater attention to the quality of our food alongside some supplementation with broad-spectrum micronutrients.
Julia J Rucklidge, Professor of Psychology, University of Canterbury; Angela Sherwin, PhD Candidate in Psychology, University of Canterbury; Joseph Boden, Professor of Psychology, Director of the Christchurch Health and Development Study, University of Otago, and Roger Mulder, Professor of Psychiatry, University of Otago
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Are Brain Chips Safe?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Ready For Cyborgization?

In yesterday’s newsletter, we asked you for your views on Brain-Computer Interfaces (BCIs), such as the Utah Array and Neuralink’s chips on/in brains that allow direct communication between brains and computers, so that (for example) a paralysed person can use a device to communicate, or manipulate a prosthetic limb or two.
We didn’t get as many votes as usual; it’s possible that yesterday’s newsletter ended up in a lot of spam filters due to repeated use of a word in “extra ______ olive oil” in its main feature!
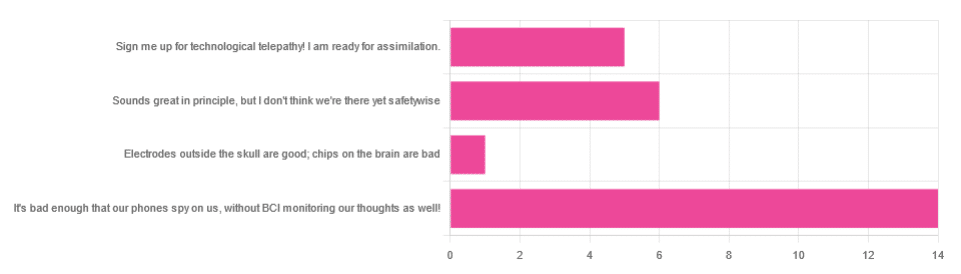
However, of the answers we did get…
- About 54% said “It’s bad enough that our phones spy on us, without BCI monitoring our thoughts as well!”
- About 23% said “Sounds great in principle, but I don’t think we’re there yet safetywise”
- About 19% said “Sign me up for technological telepathy! I am ready for assimilation”
- One (1) person said “Electrode outside the skull are good; chips on the brain are bad”
But what does the science say?
We’re not there yet safetywise: True or False?
True, in our opinion, when it comes to the latest implants, anyway. While it’s very difficult to prove a negative (it could be that everything goes perfectly in human trials), “extraordinary claims require extraordinary evidence”, and so far this seems to be lacking.
The stage before human trials is usually animal trials, starting with small creatures and working up to non-human primates if appropriate, before finally humans.
- Good news: the latest hot-topic BCI device (Neuralink) was tested on animals!
- Bad news: to say it did not go well would be an understatement
The Gruesome Story of How Neuralink’s Monkeys Actually Died
The above is a Wired article, and we tend to go for more objective sources, however we chose this one because it links to very many objective sources, including an open letter from the Physicians’ Committee for Responsible Medicine, which basically confirms everything in the Wired article. There are lots of links to primary (medical and legal) sources, too.
Electrodes outside the skull are good; chips on/in the brain are bad: True or False?
True or False depending on how they’re done. The Utah Array (an older BCI implant, now 20 years old, though it’s been updated many times since) has had a good safety record, after being used by a few dozen people with paralysis to control devices:
How the Utah Array is advancing BCI science
The Utah Array works on the same general principle as Neuralink, but the mechanics of its implementation are very different:
- The Utah Array involves a tiny bundle of microelectrodes (held together by a rigid structure that looks a bit like a nanoscale hairbrush) put in place by a brain surgeon, and that’s that.
- The Neuralink has a dynamic web of electrodes, implanted by a little robot that acts like a tiny sewing machine to implant many polymer threads, each containing its own a bunch of electrodes.
In theory, the latter is much more advanced. In practice, so far, the former has a much better safety record.
I am right to be a little worried about giving companies access to my brain: True or False?
True or False, depending on the nature of your concern.
For privacy: current BCI devices have quite simple switches operated consciously by the user. So while technically any such device that then runs its data through Bluetooth or WiFi could be hacked, this risk is no greater than using a wireless mouse and/or keyboard, because it has access to about the same amount of information.
For safety: yes, probably there is cause to be worried. Likely the first waves of commercial users of any given BCI device will be severely disabled people who are more likely to waive their rights in the hope of a life-changing assistance device, and likely some of those will suffer if things go wrong.
Which on the one hand, is their gamble to make. And on the other hand, makes rushing to human trials, for companies that do that, a little more predatory.
Take care!
Share This Post
-

Dreams: Relevance, Meanings, Interpretations
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I have a question or a suggestion for coverage in your “Psychology Sunday”. Dreams: their relevance, meanings ( if any) interpretations? I just wondered what the modern psychological opinions are about dreams in general.❞
We’ll indeed do that one of these Psychology Sundays! Thanks for suggesting it.
What we can say in advance is that there’s certainly not a single unified scientific consensus yet, but there are two or three prevailing views definitely worth covering, e.g. randomly generated, a by-product of reorganizing information in the brain, or expressions of subconscious thoughts/feelings.
There are also differences between a top-down/bottom-up approach to understanding dreaming, and efforts to tie those two together.
Watch this space!
Share This Post
-

What is ‘cognitive shuffling’ and does it really help you get to sleep? Two sleep scientists explain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’ve been on social media lately – perhaps scrolling in the middle of the night, when you know you shouldn’t but you just can’t sleep – you might have seen those videos promoting a get-to-sleep technique called “cognitive shuffling”.
The idea, proponents say, is to engage your mind with random ideas and images via a special formula:
- pick a random word (such as “cake”)
- focus on the first letter of the word (in this case, C) and list a bunch of words starting with that letter: cat, carrot, calendar and so on
- visualise each word as you go along
- when you feel ready, move onto the next letter (A) and repeat the process
- continue with each letter of the original word (so, in this case, K and then E) until you feel ready to switch to a new word or until you drift off to sleep.
It’s popular on Instagram and TikTok, but does “cognitive shuffling” have any basis in science?

Ursula Ferrara/Shutterstock Where did this idea come from?
The cognitive shuffling technique was made famous by Canada-based researcher Luc P. Beaudoin more than a decade ago, when he published a paper about how what he called “serial diverse imagining” could help with sleep.
One of Beaudoin’s hypothetical examples involved a woman thinking of the word “blanket”, then thinking bicycle (and imagining a bicycle), buying (imagining buying shoes), banana (visualising a banana tree) and so on.
Soon, Beaudoin writes, she moves onto the letter L, thinking about her friend Larry, the word “like” (imagining her son hugging his dog). She soon transitions to the letter A, thinking of the word “Amsterdam”:
and she might very vaguely imagine the large hand of a sailor gesturing for another order of fries in an Amsterdam pub while a rancid accordion plays in the background.
Sleep soon ensues. The goal, according to Beaudoin, is to think briefly about:
a neutral or pleasant target and frequently [switch] to unrelated targets (normally every 5-15 seconds).
Don’t try to relate one word with another or find a link between the words; resist the mind’s natural tendency toward sense-making.
While the research into this technique is still in its infancy, the idea is grounded in science. That’s because we know from other research good sleepers tend to have different kinds of thoughts in bed to bad sleepers.
People with insomnia are more focused on worries, problems, or noises in the environment, and are often preoccupied with not sleeping.
Good sleepers, on the other hand, typically have dream-like, hallucinatory, less ordered thoughts before nodding off.
Good sleepers typically have dream-like, hallucinatory, less ordered thoughts before nodding off. fran_kie/Shutterstock Sorting the pro-somnolent wheat from the insomnolent chaff
Cognitive shuffling attempts to mimic the thinking patterns of good sleepers by simulating the dream-like and random thought patterns they generally have before drifting off to sleep.
In particular, Beaudoin’s research describes two types of sleep-related thoughts: insomnolent (or anti-sleep) and pro-somnolent (sleep-promoting) thoughts.
Insomnolent thoughts include things such as worrying, planning, rehearsing, and ruminating on perceived problems or failings.
Pro-somnolent thoughts on the other hand involve thoughts that can help you fall asleep, such as dream-like imagery or having a calm, relaxed state of mind.
Cognitive shuffling aims to distract from or interfere with insomnolent thought. It offers a calm, neutral path for your racing mind, and can reduce the stress associated with not sleeping.
Cognitive shuffling also helps tell your brain you are ready for sleep.
In fact, the process of “shuffling” between different thoughts is similar to the way your brain naturally drifts off to sleep. During the transition to sleep, brain activity slows. Your brain starts to generate disconnected images and fleeting scenes, known as hypnagogic hallucinations, without a conscious effort to make sense of them.
By mimicking these scattered, disconnected, and random thought patterns, cognitive shuffling may help you transition from wakefulness to sleep.
And the preliminary research into this is promising. Beaudoin and his team have found serial diverse imagining helps to lower arousal before sleep, improve sleep quality and reduce the effort involved in falling asleep.
However, with only a small number of research studies, more work is needed here.
It didn’t work. Now what?
As with every new strategy, however, practise makes perfect. Don’t be disheartened if you don’t see an improvement straight away; these things take time.
Stay consistent and be kind to yourself.
And what works for some won’t work for others. Different people benefit from different types of strategies depending on how they relate to and experience stress or stressful thoughts.
Other strategies to help create the right conditions for sleep include:
- keeping a consistent pre-bedtime routine, so your brain can wind down
- watching your thoughts, without judgement, as you lie in bed
- writing down worries or to-do lists earlier in the day so you don’t think about them at bedtime.
If, despite all your best efforts, night time thoughts continue to impact your sleep or overall wellbeing, consider seeking professional help from your doctor or a trained sleep specialist.
Melinda Jackson, Associate Professor at Turner Institute for Brain and Mental Health, School of Psychological Sciences, Monash University and Eleni Kavaliotis, Research Fellow in the Sleep, Cognition, and Mood Laboratory at Monash University, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



-
5 ways vaccines changed the world
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The first modern vaccine was developed in 1796, when English physician Edward Jenner created a vaccine for smallpox. Since then, vaccines have saved millions of lives worldwide.
They’re one of the most important medical advances in history. Before vaccines, parents had no way to protect their children against deadly diseases like polio, measles, and smallpox. Vaccines changed that, empowering humans to fight and even wipe out diseases that once spread unchecked.
Here are five ways vaccines changed the world for the better.
The end of smallpox
Few diseases caused more fear than smallpox. The extremely contagious virus killed roughly a third of those it infected and left many survivors with lifelong scars. In the 20th century alone, smallpox is believed to have killed more than 300 million people.
Jenner’s groundbreaking smallpox vaccine was highly effective, allowing some parts of Europe to eliminate the disease within a century. The last known case of smallpox was recorded in 1977. Today, smallpox is the only human disease that’s ever been completely wiped out.
Vaccines have reduced the spread of more than a dozen diseases
Thanks to widespread vaccination, diseases like mumps, tetanus, chickenpox, hepatitis, and even cancer-causing HPV are now far less common. In some places, they’ve been nearly eliminated.
Polio is on track to become the second human disease ever eradicated, thanks to an aggressive global vaccination campaign. The Global Polio Eradication Initiative, launched in 1988, led to a 99 percent drop in polio cases worldwide.
Today, wild polio is found in only two countries: Pakistan and Afghanistan.
Vaccination is also responsible for a 99 percent reduction in mumps worldwide and a 90 percent reduction in chickenpox in the U.S. Measles vaccines have reduced global deaths by 87 percent between 2000 and 2022.
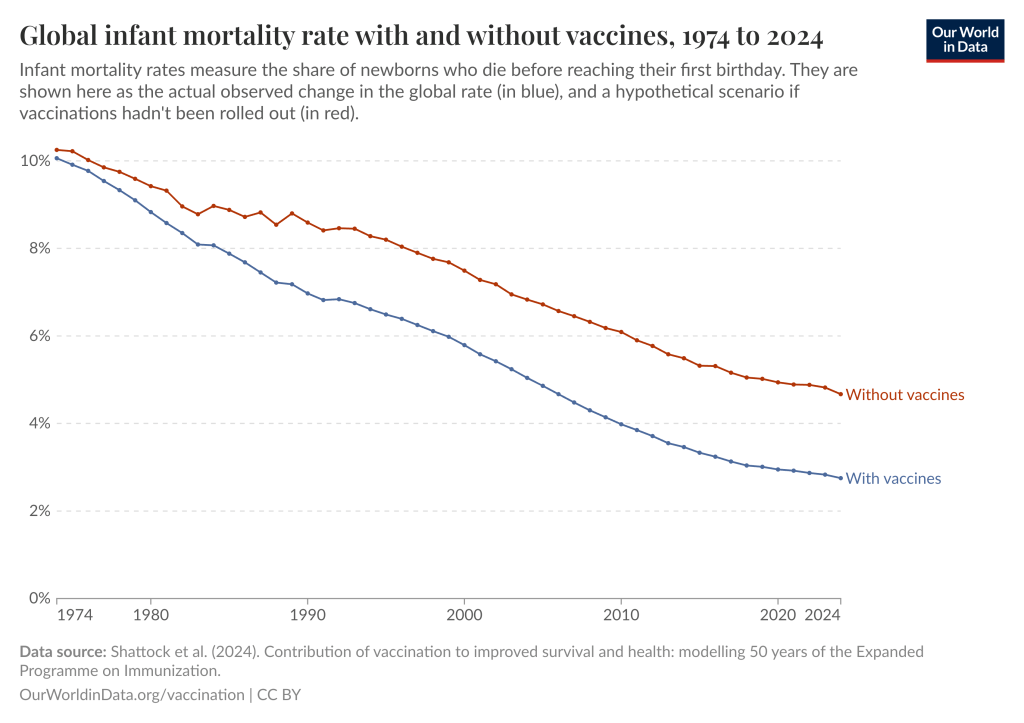
Vaccines have helped cut infant deaths in Africa by half
In 1974, about one in 10 babies died before their first birthday. Now, that number is less than one in 30. Vaccines have played a crucial role in this progress.
One analysis found that vaccines are responsible for 40 percent of the global drop in infant deaths since 1974, preventing around 100 million deaths worldwide. In Africa, the decline is even more dramatic; vaccines have helped cut infant deaths by half over the past 50 years.
Vaccines have saved over 150 million lives in the past 50 years
Since 1974, vaccines have prevented an estimated 154 million deaths globally, mostly in children under 5.
Measles vaccination alone accounts for over 90 million lives saved. Looking ahead, vaccines are expected to save over 51 million lives between 2021 and 2030.
Vaccines have helped to save trillions of dollars
Vaccines don’t just save lives: They save money too. Vaccination is one of the most cost-effective investments in public health.
Every dollar spent on vaccines saves $54 in health care costs. That adds up to over $780 billion saved this decade alone. Childhood vaccinations in the U.S. have saved nearly $3 trillion since 1994.
This article first appeared on Public Good News and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Plant-Based Healthy Cream Cheese
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cream cheese is a delicious food, and having a plant-based diet isn’t a reason to miss out. Here we have a protein-forward nuts-based cream cheese that we’re sure you’ll love (unless you’re allergic to nuts, in which case, maybe skip this one).
You will need
- 1½ cups raw cashews, soaked in warm water and then drained
- ½ cup water
- ½ cup coconut cream
- Juice of ½ lemon
- 3 tbsp nutritional yeast
- ½ tsp onion powder
- ½ tsp garlic powder
- ½ tsp black pepper
- ½ tsp cayenne pepper
- ¼ tsp MSG, or ½ tsp low-sodium salt
- Optional: ⅓ cup fresh basil
Method
(we suggest you read everything at least once before doing anything)
1) Blend all of the ingredients until creamy.
2) Optional: leave on the countertop, covered, for 1–2 hours, if you want a more fermented (effectively: cheesy) taste.
3) Refrigerate, ideally overnight, before serving. Serving on bagels is a classic, but you can also enjoy with the Healthy Homemade Flatbreads we made yesterday
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Pistachios vs Cashews – Which is Healthier? ← Pistachios actually won here, but cashews are also great and are better (from a culinary perspective) for making cream cheese
- Why You Should Diversify Your Nuts!
- Our Top 5 Spices: How Much Is Enough For Benefits?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Don’t let embarrassment stop you – talking about these anal cancer symptoms could save your life
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anal cancer doesn’t get a lot of attention. This may be because it’s relatively rare – anal cancer affects an estimated one to two Australians in every 100,000. As a comparison, melanomas affect around 70 in every 100,000 people.
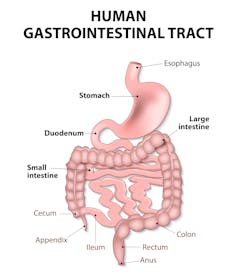
But it’s also likely due to embarrassment. Anal cancer is an abnormal growth in the cells lining the anus, the last few centimetres of the bowel. Many people feel awkward talking about this part of their body.
So, when symptoms appear – such as bleeding or itchiness – they may delay speaking to a doctor. But it’s crucial to know what to look for, because if anal cancer is caught early the chances of treating it are much higher.
The anus is the last few centimetres of the bowel. Designua/Shutterstock Do we know what causes it?
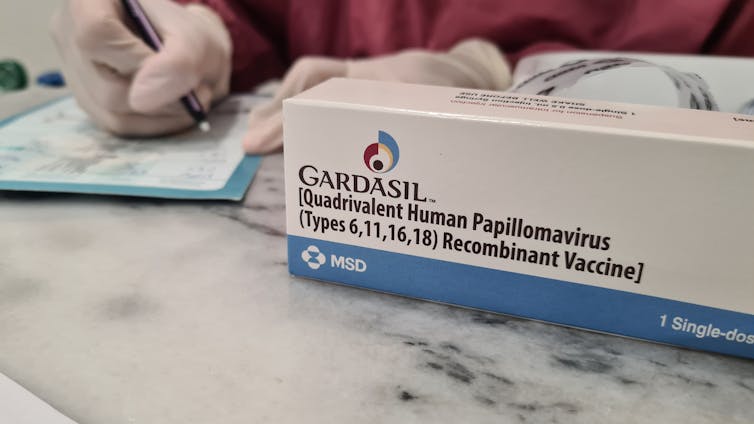
Up to nine in ten anal cancers are caused by human papillomavirus (HPV), a sexually transmitted infection.
HPV is common – more than 80% of people who have ever been sexually active will be infected at some point with a strain (there are more than 150).
Most HPV strains won’t cause any problems. But some, particularly HPV16, are higher risk. Persistent infection can cause changes in the anal lining and this can progress to anal cancer. This can happen even if you don’t have anal sex.
Vaccination against HPV is a highly effective method to reduce the risk of cancers related to HPV infection such as anal and cervical cancer.
Since the national HPV vaccination program began in Australia in 2007, there has been a substantial drop in diseases linked to HPV (such as genital warts). While it’s too early to say, it is hoped that over time cancer rates will also fall due to vaccination.
Other factors that increase your risk for anal cancer include:
- being older
- a history of smoking
- a weakened immune system (for example from medication or HIV)
- sexual activity (having anal sex or multiple sexual partners)
- a history of cervical, vulval or vaginal cancer.
Only some HPV strains are linked to cancer. wisely/Shutterstock What are the symptoms?
Sometimes anal cancer doesn’t cause any symptoms. A doctor may instead detect the cancer visually during a colonoscopy or another examination.
Other times, symptoms may include bleeding from the bottom (you might see blood on the toilet paper), a new anal lump, or feeling non-specific discomfort or itchiness in your anus.
You may also have an unusual sensation that you can’t pass a stool as “fully” or easily as before.
If you have any of these symptoms – particularly if they are new or getting worse – it is important to speak with your doctor.
The symptoms of anal cancer can be very similar to common conditions such as haemorrhoids, so it’s best to get them checked by a doctor to get the diagnosis right.
It’s understandable you might be embarrassed. But for doctors, this is all part of routine practice.
sarkao/Shutterstock Catching it early improves your chances
Survival rates are much better for anal cancer caught in the early stages.
Around 90% of people diagnosed with stage one anal cancer will live five years or more. That drops to 60% if the diagnosis is made when the cancer has developed to stage three.
The test may be as simple as a quick anal examination. Or it may require other investigations such as anoscopy (looking inside the bottom with a slim tube) or specialised ultrasounds or scans.
Most tests involve only a small amount of discomfort or none at all. They can rule out anything serious, giving you peace of mind.
If a cancer is detected, treatment usually involves radiotherapy, chemotherapy or surgery, or a combination.
The bottom line
If you need another reason to get symptoms checked out, here’s one: they could also indicate bowel cancer.
Bowel cancer (also known as colon or colorectal cancer) is the fourth most common cancer diagnosed in Australia, and the second most common cause of cancer death, with similar symptoms such as bleeding from the bottom.
So, it’s crucial to not to let awkwardness get in the way. Speak to your doctor if any symptoms concern you. Starting the conversation early could save your life.
Suzanne Mahady, Gastroenterologist & Clinical Epidemiologist, Senior Lecturer, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: