Rehab Science – by Dr. Tom Walters
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Many books of this kind deal with the injury but not the pain; some source talk about pain but not the injury; this one does both, and more.
Dr. Walters discusses in detail the nature of pain, various different kinds of pain, the factors that influence pain, and, of course, how to overcome pain.
He also takes us on a tour of various different categories of injury, because some require very different treatment than others, and while there are some catch-all “this is good/bad for healing” advices, sometimes what will help with one injury with hinder healing another. So, this information alone would make the book a worthwhile read already.
After this two-part theory-heavy introduction, the largest part of the book is given over to rehab itself, in a practical fashion.
We learn about how to make an appropriate rehab plan, get the material things we need for it (if indeed we need material things), and specific protocols to follow for various different body parts and injuries.
The style is very much that of a textbook, well-formatted and with plenty of illustrations throughout (color is sometimes relevant, so we recommend a print edition over Kindle for this one).
Bottom line: if you have an injury to heal, or even just believe in being prepared, this book is an excellent guide.
Click here to check out Rehab Science, to overcome pain and heal from injury!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

6-Minute Core Strength – by Dr. Jonathan Su

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We don’t normally do author biographies here, but in this case it’s worth noting that Dr. Su is a physiotherapist, military rehab expert, and an IAYT yoga therapist. So, these things together certainly do lend weight to his advice.
About the “6-minute” thing: this is in the style of the famous “7-minute workout” and “5 Minutes’ Physical Fitness” etc, and refers to how long each exercise session should take. The baseline is one such session per day, though of course doing more than one set of 6 minutes each time is a bonus if you wish to do so.
The exercises are focused on core strength, but they also include hip and shoulder exercises, since these are after all attached to the core, and hip and shoulder mobility counts for a lot.
A particular strength of the book is in troubleshooting mistakes of the kind that aren’t necessarily visible from photos; in this case, Dr. Su explains what you need to go for in a certain exercise, and how to know if you are doing it correctly. This alone is worth the cost of the book, in this reviewer’s opinion.
Bottom line: if you want core strength and want it simple yet comprehensive, this book can guide you.
Click here to check out 6-Minute Core Strength, and strengthen yours!
Share This Post
-

Hashimoto’s Food Pharmacology – by Dr. Izabella Wentz
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The author is a doctor of pharmacology, and we’ve featured her before as an expert on Hashimoto’s, which she has. She has recommendations about specific blood tests and medications, but in this book she’s mainly focussing on what she calls the “three Rs” of managing hypothyroidism:
- Remove the causes and triggers of your hypothyroidism, so far as possible
- Repair the damage caused to your body, especially your gut
- Replace the thyroid hormones and related things in which your body has become deficient
To this end, she provides recipes that avoid processed meats and unfermented dairy, and include plenty of nutrient-dense whole foods specifically tailored to meet the nutritional needs of someone with hypothyroidism.
A nice bonus of the presentation of recipes (of which there are 125, if we include things like “mint tea” and “tomato sauce” and “hot lemon water” as recipes) is explaining the thyroid-supporting elements of each recipe.
A downside for some will be that if you are vegetarian/vegan, this book is very much not, and since many recipes are paleo-style meat dishes, substitutions will change the nutritional profile completely.
Bottom line: if you have hypothyroidism (especially if: Hashimoto’s) and like meat, this will be a great recipe book for you.
Click here to check out Hashimoto’s Food Pharmacology, and get cooking!
Share This Post
-

The Anti-Stress Herb That Also Fights Cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What does Rhodiola rosea actually do, anyway?
Rhodiola rosea (henceforth, “rhodiola”) is a flowering herb whose roots have adaptogenic properties.
In the cold, mountainous regions of Europe and Asia where it grows, it has been used in herbal medicine for centuries to alleviate anxiety, fatigue, and depression.
What does the science say?
Well, let’s just say the science is more advanced than the traditional use:
❝In addition to its multiplex stress-protective activity, Rhodiola rosea extracts have recently demonstrated its anti-aging, anti-inflammation, immunostimulating, DNA repair and anti-cancer effects in different model systems❞
Nor is how it works a mystery, as the same paper explains:
❝Molecular mechanisms of Rhodiola rosea extracts’s action have been studied mainly along with one of its bioactive compounds, salidroside. Both Rhodiola rosea extracts and salidroside have contrasting molecular mechanisms on cancer and normal physiological functions.
For cancer, Rhodiola rosea extracts and salidroside inhibit the mTOR pathway and reduce angiogenesis through down-regulation of the expression of HIF-1α/HIF-2α.
For normal physiological functions, Rhodiola rosea extracts and salidroside activate the mTOR pathway, stimulate paracrine function and promote neovascularization by inhibiting PHD3 and stabilizing HIF-1α proteins in skeletal muscles❞
~ Ibid.
And, as for the question of “do the supplements work?”,
❝In contrast to many natural compounds, salidroside is water-soluble and highly bioavailable via oral administration❞
~ Ibid.
And as to how good it is:
❝Rhodiola rosea extracts and salidroside can impose cellular and systemic benefits similar to the effect of positive lifestyle interventions to normal physiological functions and for anti-cancer❞
~ Ibid.
Source: Rhodiola rosea: anti-stress, anti-aging, and immunostimulating properties for cancer chemoprevention
But that’s not all…
We can’t claim this as a research review if we only cite one paper (even if that paper has 144 citations of its own), and besides, it didn’t cover all the benefits yet!
Let’s first look at the science for the “traditional use” trio of benefits:
When you read those, what are your first thoughts?
Please don’t just take our word for things! Reading even just the abstracts (summaries) at the top of papers is a very good habit to get into, if you don’t have time (or easy access) to read the full text.
Reading the abstracts is also a very good way to know whether to take the time to read the whole paper, or whether it’s better to skip onto a different one.
- Perhaps you noticed that the paper we cited for anxiety was quite a small study.
- The fact is, while we found mountains of evidence for rhodiola’s anxiolytic (antianxiety) effects, they were all small and/or animal studies. So we picked a human study and went with it as illustrative.
- Perhaps you noticed that the paper we cited for fatigue pertained mostly to stress-related fatigue.
- This, we think, is a feature not a bug. After all, most of us experience fatigue because of the general everything of life, not because we just ran a literal marathon.
- Perhaps you noticed that the paper we cited for depression said it didn’t work as well as sertraline (a very common pharmaceutical SSRI antidepressant).
- But, it worked almost as well and it had far fewer adverse effects reported. Bear in mind, the side effects of antidepressants are the reason many people avoid them, or desist in taking them. So rhodiola working almost as well as sertraline for far fewer adverse effects, is quite a big deal!
Bonus features
Rhodiola also putatively offers protection against Alzheimer’s disease, Parkinson’s disease, and cerebrovascular disease in general:
Rosenroot (Rhodiola): Potential Applications in Aging-related Diseases
It may also be useful in the management of diabetes (types 1 and 2), but studies so far have only been animal studies, and/or in vitro studies. Here are two examples:
- Antihyperglycemic action of rhodiola-aqeous extract in type 1 diabetic rats
- Evaluation of Rhodiola crenulata and Rhodiola rosea for management of type 2 diabetes and hypertension
How much to take?
Dosages have varied a lot in studies. However, 120mg/day seems to cover most bases. It also depends on which of rhodiola’s 140 active compounds a particular benefit depends on, though salidroside and rosavin are the top performers.
Where to get it?
As ever, we don’t sell it (or anything else) but here’s an example product on Amazon.
Enjoy!
Share This Post
- Perhaps you noticed that the paper we cited for anxiety was quite a small study.
Related Posts
-

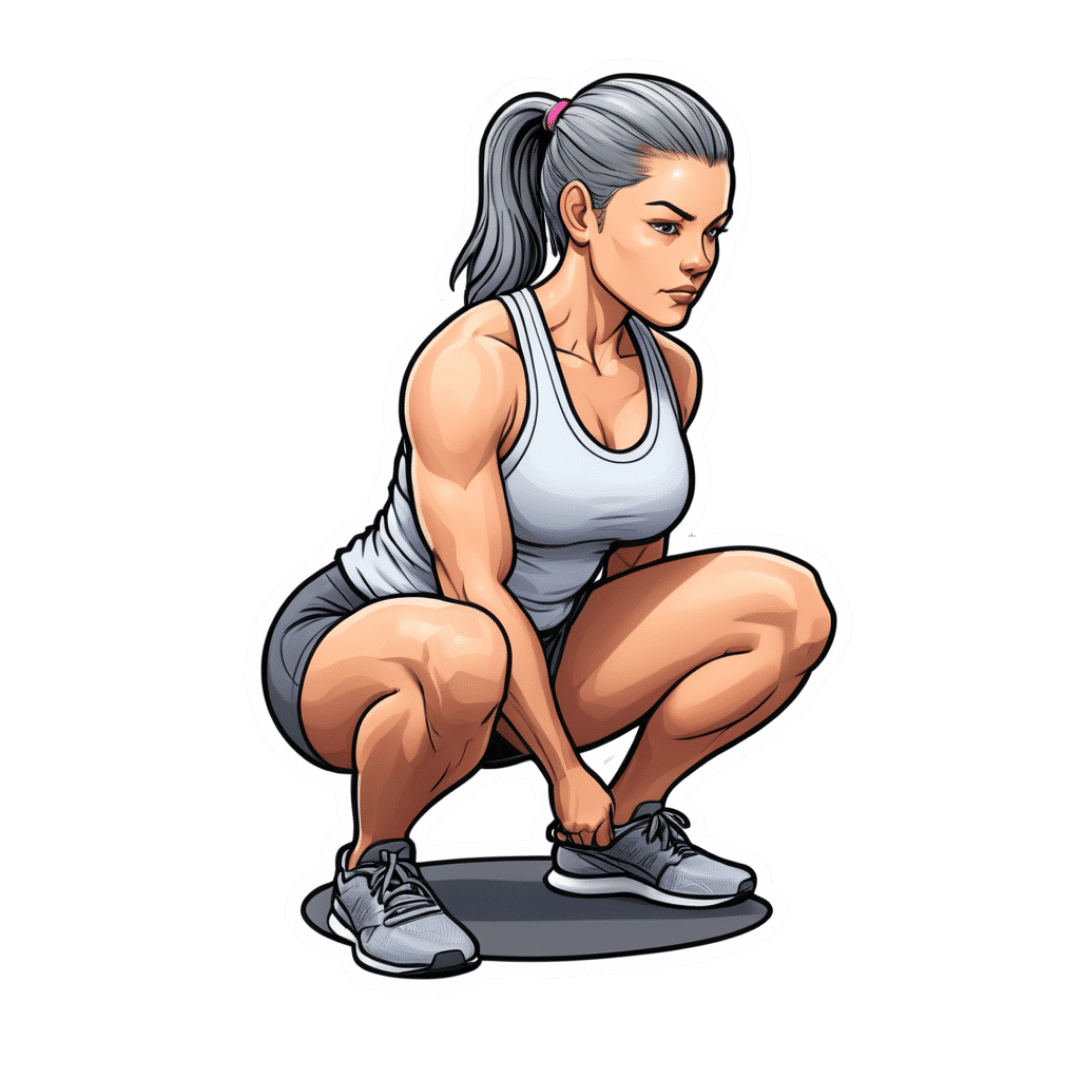
Struggle To Deep Squat? It’s Probably This One Fixable Thing Holding You Back
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Deep squat, Asian squat, Slav squat, resting squat… Whatever we want to call it, many in the West struggle with it.
Nevertheless, this struggle is entirely circumstantial, very fixable, and definitely not some kind of immutable law of the universe:
A strong foundation
A proper deep squat relies on four main factors:
- Ankle dorsiflexion allows the toes to pull toward the shin.
- Hip flexion and external rotation bring the thighs close to the torso while slightly rotating outward.
- Knee flexion ensures the thighs and calves make contact.
- Maintaining the center of mass over the midfoot is essential for balance.
Correspondingly, the reason for struggling can be a case of…
- Limited ankle mobility, which prevents the knees from moving forward, shifting weight backward.
- Tight glutes and weak hip flexors making it hard to bring the torso close to the thighs, often causing people to fall backward.
- Quad tightness can also restrict depth if the thighs cannot meet the calves.
- Proportionally longer femurs than average can cause extra difficulty as the pelvis shifts further back, requiring more knee travel for balance.
However, we said “one thing”, not “four things”, so what’s the deal?
For most people, we are told in this video, ankle mobility is the biggest limiting factor in achieving a deep squat. Thus, she recommends working on that, and (at the end of this video) links to another video with specifically ankle exercises.
For all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
The Secret To Better Squats: Foot, Knee, & Ankle Mobility
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Quinoa vs Couscous – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing quinoa to couscous, we picked the quinoa.
Why?
Firstly, quinoa is the least processed by far. Couscous, even if wholewheat, has by necessity been processed to make what is more or less the same general “stuff” as pasta. Now, the degree to which something has or has not been processed is a common indicator of healthiness, but not necessarily declarative. There are some processed foods that are healthy (e.g. many fermented products) and there are some unprocessed plant or animal products that can kill you (e.g. red meat’s health risks, or the wrong mushrooms). But in this case—quinoa vs couscous—it’s all borne out pretty much as expected.
For the purposes of the following comparisons, we’ll be looking at uncooked/dry weights.
In terms of macros, quinoa has a little more protein, slightly lower carbs, and several times the fiber. The amino acids making up quinoa’s protein are also much more varied.
In the category of vitamins, quinoa has more of vitamins A, B1, B2, B6, and B9, while couscous boasts a little more of vitamins B3 and B5. Given the respective margins of difference, as well as the total vitamins contained, this category is an easy win for quinoa.
When it comes to minerals, this one’s not even more clear. Quinoa has a lot more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Couscous, meanwhile has more of just one mineral: sodium. So, maybe not one you want more of.
All in all, today’s is an easy pick: quinoa!
Want to learn more?
You might like to read:
- Carbohydrate Mythbusting: Should You Go Light Or Heavy On Carbs?
- What’s The Real Deal With The Paleo Diet?
- Gluten Mythbusting: What’s The Truth? ← we didn’t mention it above, but couscous is by default gluten-free, and couscous, being made of wheat, is by default not gluten-free, which may be another reason for some to choose quinoa
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How Metformin Slows Aging
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Metformin And How It Slows Down Aging
That’s a bold claim for a title, but the scientific consensus is clear, and this Research Review Monday we’re going to take a look at exactly that!
Metformin is a common diabetes-management drug, used to lower blood sugar levels in people who either don’t have enough insulin or the insulin isn’t being recognized well enough by the body.
However, it also slows aging, which is a quality it’s also been studied for for more than a decade. We’ll look at some of the more recent research, though. Let’s kick off with an initial broad statement, from the paper “The Use of Metformin to Increase the Human Healthspan”, as part of the “Advances in Experimental Medicine and Biology” series:
In recent years, more attention has been paid to the possibility of using metformin as an anti-aging drug. It was shown to significantly increase the lifespan in some model organisms and delay the onset of age-associated declines. Growing amounts of evidence from clinical trials suggest that metformin can effectively reduce the risk of many age-related diseases and conditions, including cardiometabolic disorders, neurodegeneration, chronic inflammation and frailty.
How does it work?
That’s still being studied, but the scientific consensus is that it works by inducing hormesis—the process by which minor stress signals cells to start repairing themselves. How does it induce that hormesis? Again, still being studied, but it appears to do it by activating a specific enzyme; namely, the AMP-activated protein kinase:
Read: Metformin-enhances resilience via hormesis
It also has been found to slow aging by means of an anti-inflammatory effect, as a bonus!
Any bad news?
Well, firstly, in most places it’s only prescribed for diabetes management, not for healthy life extension. A lot of anti-aging enthusiasts have turned to the grey market online to get it, and we can’t recommend that.
Secondly, it does have some limitations:
- Its bioavailability isn’t great in tablet form (the form in which it is most commonly given)
- It has quite a short elimination half-life (around 6 hours), which makes it great to fix transient hyperglycemia in diabetics—job done and it’s out—but presents a logistical challenge when it comes to something so pernicious as aging.
- Some people are non-responders (a non-responder, in medicine, is someone for whom a drug simply doesn’t work, for no obvious reason)
Want to know more? Check out:
Metformin in aging and aging-related diseases: clinical applications and relevant mechanism
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: