Red Cabbage vs Spinach – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing red cabbage to spinach, we picked the spinach.
Why?
We recently compared [white] cabbage to spinach, and spinach won, so it was interesting to see whether it being red cabbage would tip the scales. It didn’t.
In terms of macros, these are once again very similar: mostly water, small amounts of carbs and protein, and enough fiber to hold them together. Nominally, red cabbage has very slightly more carbs and spinach has very slightly more protein, but the numbers are so low in both cases as to render this category still a tie in our regard, for all practical purposes. A purist argument could be made to call it a win for spinach, though.
In the category of vitamins, it’s only slightly less imbalanced than it was for white cabbage vs spinach; red cabbage has more of vitamins B5, B5, and C, while spinach has more of vitamins A, B1, B2, B3, B7, B9, E, K, and choline; a clear win for spinach.
When it comes to minerals, cabbage is once again not higher in any minerals, and spinach has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, selenium, and zinc. Another easy win for spinach.
With regard to phytochemicals, red cabbage fared better than white cabbage did, but spinach still has a much higher polyphenol content (mostly flavonols), and on the flipside, spinach has a much higher oxalate content (that’s not a problem for most people, but bad if you have certain kidney issues). So this category could be swung any which way depending on the state of your kidneys. For simplicity, we’ll record this round as a tie, but its constituent parts are worth bearing in mind.
Adding up the sections makes for an overall win for spinach, but by all means enjoy either or both; diversity is good, and cabbage of any kind is always a nutritional powerhouse; it just looks bad standing next to spinach!
Want to learn more?
You might like:
21 Most Beneficial Polyphenols & What Foods Have Them
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Even small diet tweaks can lead to sustainable weight loss

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s a well-known fact that to lose weight, you either need to eat less or move more. But how many calories do you really need to cut out of your diet each day to lose weight? It may be less than you think.
To determine how much energy (calories) your body requires, you need to calculate your total daily energy expenditure (TDEE). This is comprised of your basal metabolic rate (BMR) – the energy needed to sustain your body’s metabolic processes at rest – and your physical activity level. Many online calculators can help determine your daily calorie needs.
If you reduce your energy intake (or increase the amount you burn through exercise) by 500-1,000 calories per day, you’ll see a weekly weight loss of around one pound (0.45kg).
But studies show that even small calorie deficits (of 100-200 calories daily) can lead to long-term, sustainable weight-loss success. And although you might not lose as much weight in the short-term by only decreasing calories slightly each day, these gradual reductions are more effective than drastic cuts as they tend to be easier to stick with.

Small diet changes can still lead to weight loss in the long run. Monkey Business Images/ Shutterstock Hormonal changes
When you decrease your calorie intake, the body’s BMR often decreases. This phenomenon is known as adaptive thermogenesis. This adaptation slows down weight loss so the body can conserve energy in response to what it perceives as starvation. This can lead to a weight-loss plateau – even when calorie intake remains reduced.
Caloric restriction can also lead to hormonal changes that influence metabolism and appetite. For instance, thyroid hormones, which regulate metabolism, can decrease – leading to a slower metabolic rate. Additionally, leptin levels drop, reducing satiety, increasing hunger and decreasing metabolic rate.
Ghrelin, known as the “hunger hormone”, also increases when caloric intake is reduced, signalling the brain to stimulate appetite and increase food intake. Higher ghrelin levels make it challenging to maintain a reduced calorie diet, as the body constantly feels hungrier.
Insulin, which helps regulate blood sugar levels and fat storage, can improve in sensitivity when we reduce calorie intake. But sometimes, insulin levels decrease instead, affecting metabolism and leading to a reduction in daily energy expenditure. Cortisol, the stress hormone, can also spike – especially when we’re in a significant caloric deficit. This may break down muscles and lead to fat retention, particularly in the stomach.
Lastly, hormones such as peptide YY and cholecystokinin, which make us feel full when we’ve eaten, can decrease when we lower calorie intake. This may make us feel hungrier.
Fortunately, there are many things we can do to address these metabolic adaptations so we can continue losing weight.
Weight loss strategies
Maintaining muscle mass (either through resistance training or eating plenty of protein) is essential to counteract the physiological adaptations that slow weight loss down. This is because muscle burns more calories at rest compared to fat tissue – which may help mitigate decreased metabolic rate.
Portion control is one way of decreasing your daily calorie intake. Fevziie/ Shutterstock Gradual caloric restriction (reducing daily calories by only around 200-300 a day), focusing on nutrient-dense foods (particularly those high in protein and fibre), and eating regular meals can all also help to mitigate these hormonal challenges.
But if you aren’t someone who wants to track calories each day, here are some easy strategies that can help you decrease daily calorie intake without thinking too much about it:
1. Portion control: reducing portion sizes is a straightforward way of reducing calorie intake. Use smaller plates or measure serving sizes to help reduce daily calorie intake.
2. Healthy swaps: substituting high-calorie foods with lower-calorie alternatives can help reduce overall caloric intake without feeling deprived. For example, replacing sugary snacks with fruits or swapping soda with water can make a substantial difference to your calorie intake. Fibre-rich foods can also reduce the calorie density of your meal.
3. Mindful eating: practising mindful eating involves paying attention to hunger and fullness cues, eating slowly, and avoiding distractions during meals. This approach helps prevent overeating and promotes better control over food intake.
4. Have some water: having a drink with your meal can increase satiety and reduce total food intake at a given meal. In addition, replacing sugary beverages with water has been shown to reduce calorie intake from sugars.
4. Intermittent fasting: restricting eating to specific windows can reduce your caloric intake and have positive effects on your metabolism. There are different types of intermittent fasting you can do, but one of the easiest types is restricting your mealtimes to a specific window of time (such as only eating between 12 noon and 8pm). This reduces night-time snacking, so is particularly helpful if you tend to get the snacks out late in the evening.
Long-term behavioural changes are crucial for maintaining weight loss. Successful strategies include regular physical activity, continued mindful eating, and periodically being diligent about your weight and food intake. Having a support system to help you stay on track can also play a big role in helping you maintain weight loss.
Modest weight loss of 5-10% body weight in people who are overweight or obese offers significant health benefits, including improved metabolic health and reduced risk of chronic diseases. But it can be hard to lose weight – especially given all the adaptations our body has to prevent it from happening.
Thankfully, small, sustainable changes that lead to gradual weight loss appear to be more effective in the long run, compared with more drastic lifestyle changes.
Alexandra Cremona, Lecturer, Human Nutrition and Dietetics, University of Limerick
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

How To Prevent And Reverse Type 2 Diabetes
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Turn back the clock on insulin resistance

This is Dr. Jason Fung. He’s a world-leading expert on intermittent fasting and low carbohydrate approaches to diet. He also co-founded the Intensive Dietary Management Program, later rebranded to the snappier title: The Fasting Method, a program to help people lose weight and reverse type 2 diabetes. Dr. Fung is certified with the Institute for Functional Medicine, for providing functional medicine certification along with educational programs directly accredited by the Accreditation Council for Continuing Medical Education (ACCME).
Why Intermittent Fasting?
Intermittent fasting is a well-established, well-evidenced, healthful practice for most people. In the case of diabetes, it becomes complicated, because if one’s blood sugars are too low during a fasting period, it will need correcting, thus breaking the fast.
Note: this is about preventing and reversing type 2 diabetes. Type 1 is very different, and sadly cannot be prevented or reversed in this fashion.
However, these ideas may still be useful if you have T1D, as you have an even greater need to avoid developing insulin resistance; you obviously don’t want your exogenous insulin to stop working.
Nevertheless, please do confer with your endocrinologist before changing your dietary habits, as they will know your personal physiology and circumstances in ways that we (and Dr. Fung) don’t.
In the case of having type 2 diabetes, again, please still check with your doctor, but the stakes are a lot lower for you, and you will probably be able to fast without incident, depending on your diet itself (more on this later).
Intermittent Fasting can be extra helpful for the body in the case of type 2 diabetes, as it helps give the body a rest from high insulin levels, thus allowing the body to become gradually re-sensitised to insulin.
Why low carbohydrate?
Carbohydrates, especially sugars, especially fructose*, cause excess sugar to be quickly processed by the liver and stored there. When the body’s ability to store glycogen is exceeded, the liver stores energy as fat instead. The resultant fatty liver is a major contributor to insulin resistance, when the liver can’t keep up with the demand; the blood becomes spiked full of unprocessed sugars, and the pancreas must work overtime to produce more and more insulin to deal with that—until the body starts becoming desensitized to insulin. In other words, type 2 diabetes.
There are other factors that affect whether we get type 2 diabetes, for example a genetic predisposition. But, our carb intake is something we can control, so it’s something that Dr. Fung focuses on.
*A word on fructose: actual fruits are usually diabetes-neutral or a net positive due to their fiber and polyphenols.
Fructose as an added ingredient, however, not so much. That stuff zips straight into your veins with nothing to slow it down and nothing to mitigate it.
The advice from Dr. Fung is simple here: cut the carbs. If you are already diabetic and do this with no preparation, you will probably simply suffer hypoglycemia, so instead:
- Enjoy a fibrous starter (a salad, some fruit, or perhaps some nuts)
- Load up with protein first, during your main meal—this will start to trigger your feelings of satedness
- Eat carbs last (preferably whole, unprocessed carbohydrates), and stop eating when 80% full.
Adapting Intermittent Fasting to diabetes
Dr. Fung advocates for starting small, and gradually increasing your fasting period, until, ideally, fasting 16 hours per day. You probably won’t be able to do this immediately, and that’s fine.
You also probably won’t be able to do this, if you don’t also make the dietary adjustments that help to give your liver a break, and thus by knock-on-effect, give your pancreas a break too.
With the dietary adjustments too, however, your insulin production-and-response will start to return to its pre-diabetic state, and finally its healthy state, after which, it’s just a matter of maintenance.
Want to hear more from Dr. Fung?
You may enjoy his blog, and for those who like videos, here is his YouTube channel:
Share This Post
-

Can Saturated Fats Be Healthy?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Saturated Fat: What’s The Truth?

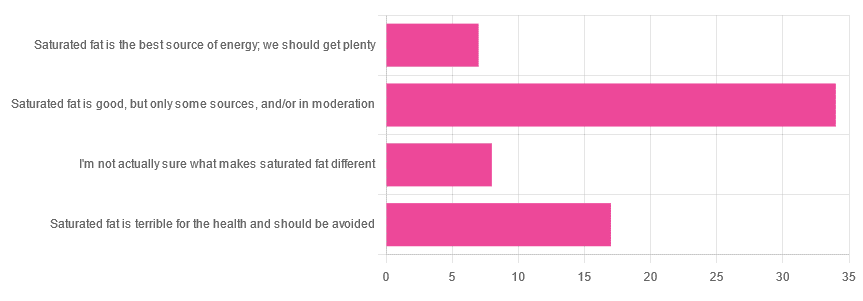
We asked you for your health-related opinion of saturated fat, and got the above-pictured, below-described, set of results.
- Most recorded votes were for “Saturated fat is good, but only some sources, and/or in moderation”
- This is an easy one to vote for, because of the “and/or in moderation” part, which tends to be a “safe bet” for most things.
- Next most popular was “Saturated fat is terrible for the health and should be avoided”
- About half as many recorded votes were for “I’m not actually sure what makes saturated fat different”, which is a very laudable option to click. Admitting when we don’t know things (and none of us know everything) is a very good first step to learning about them!
- Fewest recorded votes were for “Saturated fat is the best source of energy; we should get plenty”.
So, what does the science say?
First, a bit of physics, chemistry, and biology
You may be wondering what, exactly, saturated fats are “saturated” with. That’s a fair question, so…
All fats have a molecular structure made up of carbon, hydrogen, and oxygen atoms. Saturated fats are saturated with hydrogen, and thus have only single bonds between carbon atoms (unsaturated fats have at least one double-bond between carbon atoms).
The observable effect this has on them, is that fats that are saturated with hydrogen are solid at room temperature, whereas unsaturated fats are liquid at room temperature. Their different properties also make for different interactions inside the human body, including how likely or not they are to (for example) clog arteries.
See also: Could fat in your bloodstream cause blood clots?
Saturated fat is the best source of energy; we should get plenty: True or False?
False, in any reasonable interpretation, anyway. That is to say, if your idea of “plenty” is under 13g (e.g: two tablespoons of butter, and no saturated fat from other sources, e.g. meat) per day, then yes, by all means feel free to eat plenty. More than that, though, and you might want to consider trimming it down a bit.
The American Heart Association has this to say:
❝When you hear about the latest “diet of the day” or a new or odd-sounding theory about food, consider the source.
The American Heart Association recommends limiting saturated fats, which are found in butter, cheese, red meat and other animal-based foods, and tropical oils.
Decades of sound science has proven it can raise your “bad” cholesterol and put you at higher risk for heart disease.❞
Source: The American Heart Association Diet and Lifestyle Recommendations on Saturated Fat
The British Heart Foundation has a similar statement:
❝Despite what you read in the media, our advice is clear: replace saturated fats with unsaturated fats and avoid trans fats. Saturated fat is the kind of fat found in butter, lard, ghee, fatty meats and cheese. This is linked to an increased risk of heart and circulatory disease❞
Source: British Heart Foundation: What does fat do and what is saturated fat?
As for the World Health Organization:
❝1. WHO strongly recommends that adults and children reduce saturated fatty acid intake to 10% of total energy intake
2. WHO suggests further reducing saturated fatty acid intake to less than 10% of total energy intake
3. WHO strongly recommends replacing saturated fatty acids in the diet with polyunsaturated fatty acids; monounsaturated fatty acids from plant sources; or carbohydrates from foods containing naturally occurring dietary fibre, such as whole grains, vegetables, fruits and pulses.❞
Source: Saturated fatty acid and trans-fatty acid intake for adults and children: WHO guideline
Please note, organizations such as the AHA, the BHF, and the WHO are not trying to sell us anything, and just would like us to not die of heart disease, the world’s #1 killer.
As for “the best source of energy”…
We evolved to eat (much like our nearest primate cousins) a diet consisting mostly of fruits and other edible plants, with a small supplementary amount of animal-source protein and fats.
That’s not to say that because we evolved that way we have to eat that way—we are versatile omnivores. But for example, we are certainly not complete carnivores, and would quickly sicken and die if we tried to live on only meat and animal fat (we need more fiber, more carbohydrates, and many micronutrients that we usually get from plants)
The closest that humans tend to come to doing such is the ketogenic diet, which focuses on a high fat, low carbohydrate imbalance, to promote ketosis, in which the body burns fat for energy.
The ketogenic diet does work, and/but can cause a lot of health problems if a lot of care is not taken to avoid them.
See for example: 7 Keto Risks To Keep In Mind
Saturated fat is terrible for the health and should be avoided: True or False?
False, if we are talking about “completely”.
Firstly, it’s practically impossible to cut out all saturated fats, given that most dietary sources of fat are a mix of saturated, unsaturated (mono- and poly-), and trans fats (which are by far the worst, but beyond the scope of today’s main feature).
Secondly, a lot of research has been conducted and found insignificant or inconclusive results, in cases where saturated fat intake was already within acceptable levels (per the recommendations we mentioned earlier), and then cut down further.
Rather than fill up the newsletter with individual studies of this kind here’s a high-quality research review, looking at 19 meta-analyses, each of those meta-analyses having looked at many studies:
Dietary saturated fat and heart disease: a narrative review
Saturated fat is good, but only some sources, and/or in moderation: True or False?
True! The moderation part is easy to guess, so let’s take a look at the “but only some sources”.
We were not able to find any convincing science to argue for health-based reasons to favor plant- or animal-sourced saturated fat. However…
Not all saturated fats are created equal (there are many kinds), and also many of the foods containing them have additional nutrients, or harmful compounds, that make a big difference to overall health, when compared gram-for-gram in terms of containing the same amount of saturated fat.
For example:
- Palm oil’s saturated fat contains a disproportionate amount of palmitic acid, which raises LDL (“bad” cholesterol) without affecting HDL (“good” cholesterol), thus having an overall heart-harmful effect.
- Most animal fats contain a disproportionate amount of stearic acid, which has statistically insignificant effects on LDL and HDL levels, and thus is broadly considered “heart neutral” (in moderation!)
- Coconut oil’s saturated fat contains a disproportionate amount of lauric acid, which raises total cholesterol, but mostly HDL without affecting LDL, thus having an overall heart-beneficial effect (in moderation!)
Do you know what’s in the food you eat?
Test your knowledge with the BHF’s saturated fat quiz!
Enjoy!
Share This Post
- Most recorded votes were for “Saturated fat is good, but only some sources, and/or in moderation”



Related Posts
-

Why scrapping the term ‘long COVID’ would be harmful for people with the condition
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The assertion from Queensland’s chief health officer John Gerrard that it’s time to stop using the term “long COVID” has made waves in Australian and international media over recent days.
Gerrard’s comments were related to new research from his team finding long-term symptoms of COVID are similar to the ongoing symptoms following other viral infections.
But there are limitations in this research, and problems with Gerrard’s argument we should drop the term “long COVID”. Here’s why.
A bit about the research
The study involved texting a survey to 5,112 Queensland adults who had experienced respiratory symptoms and had sought a PCR test in 2022. Respondents were contacted 12 months after the PCR test. Some had tested positive to COVID, while others had tested positive to influenza or had not tested positive to either disease.
Survey respondents were asked if they had experienced ongoing symptoms or any functional impairment over the previous year.
The study found people with respiratory symptoms can suffer long-term symptoms and impairment, regardless of whether they had COVID, influenza or another respiratory disease. These symptoms are often referred to as “post-viral”, as they linger after a viral infection.
Gerrard’s research will be presented in April at the European Congress of Clinical Microbiology and Infectious Diseases. It hasn’t been published in a peer-reviewed journal.
After the research was publicised last Friday, some experts highlighted flaws in the study design. For example, Steven Faux, a long COVID clinician interviewed on ABC’s television news, said the study excluded people who were hospitalised with COVID (therefore leaving out people who had the most severe symptoms). He also noted differing levels of vaccination against COVID and influenza may have influenced the findings.
In addition, Faux pointed out the survey would have excluded many older people who may not use smartphones.
The authors of the research have acknowledged some of these and other limitations in their study.
Ditching the term ‘long COVID’
Based on the research findings, Gerrard said in a press release:
We believe it is time to stop using terms like ‘long COVID’. They wrongly imply there is something unique and exceptional about longer term symptoms associated with this virus. This terminology can cause unnecessary fear, and in some cases, hypervigilance to longer symptoms that can impede recovery.
But Gerrard and his team’s findings cannot substantiate these assertions. Their survey only documented symptoms and impairment after respiratory infections. It didn’t ask people how fearful they were, or whether a term such as long COVID made them especially vigilant, for example.
Tens of thousands of Australians, and millions of people worldwide, have long COVID.
New Africa/ShutterstockIn discussing Gerrard’s conclusions about the terminology, Faux noted that even if only 3% of people develop long COVID (the survey found 3% of people had functional limitations after a year), this would equate to some 150,000 Queenslanders with the condition. He said:
To suggest that by not calling it long COVID you would be […] somehow helping those people not to focus on their symptoms is a curious conclusion from that study.
Another clinician and researcher, Philip Britton, criticised Gerrard’s conclusion about the language as “overstated and potentially unhelpful”. He noted the term “long COVID” is recognised by the World Health Organization as a valid description of the condition.
A cruel irony
An ever-growing body of research continues to show how COVID can cause harm to the body across organ systems and cells.
We know from the experiences shared by people with long COVID that the condition can be highly disabling, preventing them from engaging in study or paid work. It can also harm relationships with their friends, family members, and even their partners.
Despite all this, people with long COVID have often felt gaslit and unheard. When seeking treatment from health-care professionals, many people with long COVID report they have been dismissed or turned away.
Last Friday – the day Gerrard’s comments were made public – was actually International Long COVID Awareness Day, organised by activists to draw attention to the condition.
The response from people with long COVID was immediate. They shared their anger on social media about Gerrard’s comments, especially their timing, on a day designed to generate greater recognition for their illness.
Since the start of the COVID pandemic, patient communities have fought for recognition of the long-term symptoms many people faced.
The term “long COVID” was in fact coined by people suffering persistent symptoms after a COVID infection, who were seeking words to describe what they were going through.
The role people with long COVID have played in defining their condition and bringing medical and public attention to it demonstrates the possibilities of patient-led expertise. For decades, people with invisible or “silent” conditions such as ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome) have had to fight ignorance from health-care professionals and stigma from others in their lives. They have often been told their disabling symptoms are psychosomatic.
Gerrard’s comments, and the media’s amplification of them, repudiates the term “long COVID” that community members have chosen to give their condition an identity and support each other. This is likely to cause distress and exacerbate feelings of abandonment.
Terminology matters
The words we use to describe illnesses and conditions are incredibly powerful. Naming a new condition is a step towards better recognition of people’s suffering, and hopefully, better diagnosis, health care, treatment and acceptance by others.
The term “long COVID” provides an easily understandable label to convey patients’ experiences to others. It is well known to the public. It has been routinely used in news media reporting and and in many reputable medical journal articles.
Most importantly, scrapping the label would further marginalise a large group of people with a chronic illness who have often been left to struggle behind closed doors.

Deborah Lupton, SHARP Professor, Vitalities Lab, Centre for Social Research in Health and Social Policy Centre, and the ARC Centre of Excellence for Automated Decision-Making and Society, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Yoga Sucks, According To A Yoga Teacher
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Yoga’s great, except in the ways it isn’t:
These ideas might meet with some resistance
Fun fact: around 75% of yoga practitioners worldwide are female, and 81% of them are over the age of 30.
Fun fact: women over the age of 30 experience sarcopenia, the gradual loss of skeletal muscle mass and strength, and osteoporosis, the thinning and weakening of bones.
…which is a pain in each part, because:
- Muscle is metabolically active tissue, so declining muscle mass slows metabolism and lowers calorie needs, contributing to weight gain if eating habits don’t change.
- Reduced bone density increases the risk of fractures, stress injuries like shin splints, loss of height due to spinal compression, and serious injury from falls.
Happily, these age-related changes can be slowed or even prevented through correct fitness choices.
Good news: resistance training involves working against progressively challenging external loads that create mechanical stress to stimulate muscle and bone growth.
Bad news: yoga is not resistance training and doesn’t meaningfully build muscle mass or increase bone density for most practitioners.
To be clear, yoga can increase strength and benefit beginners initially, but it quickly plateaus and doesn’t provide enough stimulus for bone density improvements.
In summary: yoga is valuable for flexibility, mental health, and enjoyment, but it should be combined with meaningful resistance training for health, longevity, and resilience.
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Which Style Of Yoga Is Best For You?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Everything you need to know about cervical cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Every year, around 11,500 new cases of cervical cancer are diagnosed in the U.S. While cervical cancer used to be one of the most common causes of cancer death for U.S. women, the vaccine against the human papillomavirus (HPV), and increased early screening and detection have resulted in a decrease in rates.
“Cervical cancer is almost always preventable and typically diagnosed in patients who have either never had a screening test or have gone many years without one,” says Fred Wyand, director of communications at the American Sexual Health Association, which includes the National Cervical Cancer Coalition.
January is Cervical Cancer Awareness Month, so we spoke to experts to learn more about what it is, its symptoms, and what you can do to prevent it.
What is cervical cancer?
Cervical cancer is a type of cancer that starts in the cervix—the lower part of the uterus that connects the vagina to the uterus. Cervical cancer can affect anyone with a cervix but is most frequently diagnosed in women ages 35 to 44, according to the American Cancer Society.
There are two types:
- Squamous cell carcinoma: Cervical cancer that starts in the thin squamous cells on the outside of the cervix. This is the most common type of cervical cancer.
- Adenocarcinoma: Cervical cancer that starts in glandular cells that line the inside of the cervix. This type of cervical cancer is less common.
In some cases, cervical cancer has features of both types.
What causes cervical cancer?
Almost all cases of cervical cancer are caused by high-risk cases of HPV, a virus that is spread through sexual activity or other close skin-to-skin contact. But don’t panic: HPV is very common, and getting HPV doesn’t always mean you’ll get cervical cancer. Around 85 percent of people in the U.S. will get an HPV infection in their lifetime, but for most people, the virus clears on its own.
However, there are many strains of HPV, and some are linked to cervical cancer. In those cases, when the virus does not clear on its own and the HPV infection persists, it can cause a range of cancers in both men and women, including cancers of the cervix, anus, penis, throat, and vagina.
That’s why HPV vaccination is so important for all people: It can help prevent many types of cancer, including cervical cancer caused by those high-risk HPV infections.
What are the symptoms of cervical cancer?
Cervical cancer doesn’t usually have symptoms in its early stages, but once cancer begins to spread, the symptoms can include:
- Vaginal bleeding between periods, after sexual intercourse, or after menopause.
- Heavier and longer menstrual periods than usual.
- Vaginal discharge that has a strong odor and is watery.
- Pelvic pain or pain during sexual intercourse.
In more advanced stages, symptoms of cervical cancer can include:
- Leg swelling.
- Difficult or painful bowel movements or bleeding during a bowel movement.
- Blood in urine or difficulty urinating.
- Back pain.
“Most women present with no symptoms,” Dr. Kristina A. Butler, gynecologic oncologist at Mayo Clinic, tells PGN. “Therefore, the checkups with visualization of the cervix, speaking with your provider, and having a Pap smear are so important.”
How can you help prevent or reduce your risk for cervical cancer?
Vaccination: Cervical cancer is highly preventable. The most effective way to help protect yourself from it is by getting the HPV vaccine. The HPV vaccine is most effective before a person is first exposed to HPV, typically before becoming sexually active.
“If we are able to vaccinate children before they become adults [and] are subsequently exposed, those individuals are maximally protected against the [worst effects] of the virus, which could ultimately be cancer,” Butler adds.
You’re eligible to get the vaccine if you’re between 9 and 45 years old, but there are specific guidelines for each age group. The Centers for Disease Control and Prevention recommends HPV vaccination for children ages 11 or 12 (though it can start at 9 years).
The CDC says that you can get catch-up doses until you’re 26 if you didn’t get vaccinated earlier, but if you’re between 26 and 45 years old, you should talk to your health care provider about your individual risk for HPV and to see if you should get the vaccine.
Screenings: This is another effective way to prevent cervical cancer.
Dr. Deanna Gerber, a gynecologic oncologist at NYU Langone’s Laura and Isaac Perlmutter Cancer Center, tells PGN that regular screenings can catch HPV before it has a chance to become cancer.
“Now that we’re encouraging people to see their gynecologist and get screening more regularly, we’re catching cancer at earlier stages,” she says.
Screenings for cervical cancer include:
- Pap smear: During a Pap smear, also known as a Pap test, cells are collected from your cervix to find precancerous or cervical cancer cells. Pap smears should start at 21 years old, regardless of when you start having sex.
If you’re between 21 and 29, you should get a Pap smear every three years. If you’re 30 to 65 years old, it’s recommended you get one every three years, a Pap and HPV test together every five years, or an HPV test alone every five years.
- HPV test: During an HPV test, cells are collected from your cervix to look for infection with high-risk HPV strains that can cause cervical cancer. If you’re between 21 and 30 years old, it’s only recommended that you get an HPV test if you had an abnormal Pap smear result. After 30, an HPV test is recommended with a Pap smear every five years, as long as other results were normal.
(People over 65 years old should talk to their health care provider about whether they need screening.)
Not smoking: Avoiding smoking can reduce your risk of developing cervical cancer because “HPV and smoking tobacco work together to accelerate the negative effects of HPV,” says Gerber.
Wearing condoms: Although condoms don’t completely prevent HPV infection, they provide some protection. And according to the CDC, the use of condoms has been associated with a lower rate of cervical cancer.
There is hope with early detection
There is hope for people diagnosed with cervical cancer. “Compared to the survival [rates] 10 years ago, women survive much longer now with the great treatments we have,” adds Butler.
Some of those treatments and advances include radiation, chemotherapy, and surgical therapy.
And while there may be some stigma surrounding sexual health, it’s important to advocate for yourself, says Gerber.
“Being comfortable and bold talking to your doctor about your health or any concerns that you have, feeling comfortable with your provider by asking all these questions is really the best thing you can do.”
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: