Non-Sleep Deep Rest: A Neurobiologist’s Take
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How to get many benefits of sleep, while awake!
Today we’re talking about Dr. Andrew Huberman, a neuroscientist and professor in the department of neurobiology at Stanford School of Medicine.
He’s also a popular podcaster, and as his Wikipedia page notes:
❝In episodes lasting several hours, Huberman talks about the state of research in a specific topic, both within and outside his specialty❞
Today, we won’t be taking hours, and we will be taking notes from within his field of specialty (neurobiology). Specifically, in this case:
Non-Sleep Deep Rest (NSDR)
What is it? To quote from his own dedicated site on the topic:
❝What is NSDR (Yoga Nidra)? Non-Sleep Deep Rest, also known as NSDR, is a method of deep relaxation developed by Dr. Andrew Huberman, a neuroscientist at Stanford University School of Medicine.
It’s a process that combines controlled breathing and detailed body scanning to bring you into a state of heightened awareness and profound relaxation. The main purpose of NSDR is to reduce stress, enhance focus, and improve overall well-being.❞
While it seems a bit bold of Dr. Huberman to claim that he developed yoga nidra, it is nevertheless reassuring to get a neurobiologist’s view on this:
How it works, by science
Dr. Huberman says that by monitoring EEG readings during NSDR, we can see how the brain slows down. Measurably!
- It goes from an active beta range of 13–30 Hz (normal waking) to a conscious meditation state of an alpha range of 8–13 Hz.
- However, with practice, it can drop further, into a theta range of 4–8 Hz.
- Ultimately, sustained SSDR practice can get us to 0.5–3 Hz.
This means that the brain is functioning in the delta range, something that typically only occurs during our deepest sleep.
You may be wondering: why is delta lower than theta? That’s not how I remember the Greek alphabet being ordered!
Indeed, while the Greek alphabet goes alpha beta gamma delta epsilon zeta eta theta (and so on), the brainwave frequency bands are:
- Gamma = concentrated focus, >30 Hz
- Beta = normal waking, 13–30 Hz
- Alpha = relaxed state, 8–13 Hz
- Theta = light sleep, 4–8 Hz
- Delta = deep sleep, 1–4 Hz
Source: Sleep Foundation ← with a nice infographic there too
NSDR uses somatic cues to engage our parasympathetic nervous system, which in turn enables us to reach those states. The steps are simple:
- Pick a time and place when you won’t be disturbed
- Lie on your back and make yourself comfortable
- Close your eyes as soon as you wish, and now that you’ve closed them, imagine closing them again. And again.
- Slowly bring your attention to each part of your body in turn, from head to toe. As your attention goes to each part, allow it to relax more.
- If you wish, you can repeat this process for another wave, or even a third.
- Find yourself well-rested!
Note: this engagement of the parasympathetic nervous system and slowing down of brain activity accesses restorative states not normally available while waking, but 10 minutes of NSDR will not replace 7–9 hours of sleep; nor will it give you the vital benefits of REM sleep specifically.
So: it’s an adjunct, not a replacement
Want to try it, but not sure where/how to start?
When you’re ready, let Dr. Huberman himself guide you through it in this shortish (10:49) soundtrack:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to try it, but not right now? Bookmark it for later
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

When supplies resume, should governments subsidise drugs like Ozempic for weight loss? We asked 5 experts

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hundreds of thousands of people worldwide are taking drugs like Ozempic to lose weight. But what do we actually know about them? This month, The Conversation’s experts explore their rise, impact and potential consequences.
You’ve no doubt heard of Ozempic but have you heard of Wegovy? They’re both brand names of the drug semaglutide, which is currently in short supply worldwide.
Ozempic is a lower dose of semaglutide, and is approved and used to treat diabetes in Australia. Wegovovy is approved to treat obesity but is not yet available in Australia. Shortages of both drugs are expected to last throughout 2024.
Both drugs are expensive. But Ozempic is listed on Australia’s Pharmaceutical Benefits Schedule (PBS), so people with diabetes can get a three-week supply for A$31.60 ($7.70 for concession card holders) rather than the full price ($133.80).
Wegovy isn’t listed on the PBS to treat obesity, meaning when it becomes available, users will need to pay the full price. But should the government subsidise it?
Wegovy’s manufacturer will need to make the case for it to be added to the PBS to an independent advisory committee. The company will need to show Wegovy is a safe, clinically effective and cost-effective treatment for obesity compared to existing alternatives.
In the meantime, we asked five experts: when supplies resume, should governments subsidise drugs like Ozempic for weight loss?
Four out of five said yes
This is the last article in The Conversation’s Ozempic series. Read the other articles here.
Disclosure statements: Clare Collins is a National Health and Medical Research Council (NHMRC) Leadership Fellow and has received research grants from the National Health and Medical Research Council (NHMRC), the Australian Research Council (ARC), the Medical Research Future Fund (MRFF), the Hunter Medical Research Institute, Diabetes Australia, Heart Foundation, Bill and Melinda Gates Foundation, nib foundation, Rijk Zwaan Australia, the Western Australian Department of Health, Meat and Livestock Australia, and Greater Charitable Foundation. She has consulted to SHINE Australia, Novo Nordisk (for weight management resources and an obesity advisory group), Quality Bakers, the Sax Institute, Dietitians Australia and the ABC. She was a team member conducting systematic reviews to inform the 2013 Australian Dietary Guidelines update, the Heart Foundation evidence reviews on meat and dietary patterns and current co-chair of the Guidelines Development Advisory Committee for Clinical Practice Guidelines for Treatment of Obesity; Emma Beckett has received funding for research or consulting from Mars Foods, Nutrition Research Australia, NHMRC, ARC, AMP Foundation, Kellogg and the University of Newcastle. She works for FOODiQ Global and is a fat woman. She is/has been a member of committees/working groups related to nutrition or food, including for the Australian Academy of Science, the NHMRC and the Nutrition Society of Australia; Jonathan Karnon does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment; Nial Wheate in the past has received funding from the ACT Cancer Council, Tenovus Scotland, Medical Research Scotland, Scottish Crucible, and the Scottish Universities Life Sciences Alliance. He is a fellow of the Royal Australian Chemical Institute, a member of the Australasian Pharmaceutical Science Association and a member of the Australian Institute of Company Directors. Nial is the chief scientific officer of Vaihea Skincare LLC, a director of SetDose Pty Ltd (a medical device company) and a Standards Australia panel member for sunscreen agents. Nial regularly consults to industry on issues to do with medicine risk assessments, manufacturing, design and testing; Priya Sumithran has received grant funding from external organisations, including the NHMRC and MRFF. She is in the leadership group of the Obesity Collective and co-authored manuscripts with a medical writer provided by Novo Nordisk and Eli Lilly.
Fron Jackson-Webb, Deputy Editor and Senior Health Editor, The Conversation
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Should You Go Light Or Heavy On Carbs?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carb-Strong or Carb-Wrong?

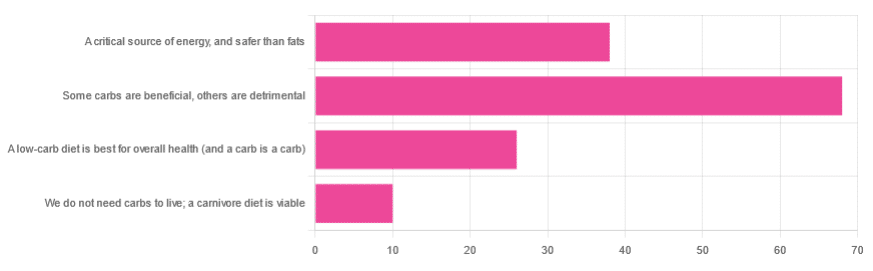
We asked you for your health-related view of carbs, and got the above-depicted, below-described, set of responses
- About 48% said “Some carbs are beneficial; others are detrimental”
- About 27% said “Carbs are a critical source of energy, and safer than fats”
- About 18% said “A low-carb diet is best for overall health (and a carb is a carb)”
- About 7% said “We do not need carbs to live; a carnivore diet is viable”
But what does the science say?
Carbs are a critical source of energy, and safer than fats: True or False?
True and False, respectively! That is: they are a critical source of energy, and carbs and fats both have an important place in our diet.
❝Diets that focus too heavily on a single macronutrient, whether extreme protein, carbohydrate, or fat intake, may adversely impact health.❞
Source: Low carb or high carb? Everything in moderation … until further notice
(the aforementioned lead author Dr. de Souza, by the way, served as an external advisor to the World Health Organization’s Nutrition Guidelines Advisory Committee)
Some carbs are beneficial; others are detrimental: True or False?
True! Glycemic index is important here. There’s a big difference between eating a raw carrot and drinking high-fructose corn syrup:
Which Sugars Are Healthier, And Which Are Just The Same?
While some say grains and/or starchy vegetables are bad, best current science recommends:
- Eat some whole grains regularly, but they should not be the main bulk of your meal (non-wheat grains are generally better)
- Starchy vegetables are not a critical food group, but in moderation they are fine.
To this end, the Mediterranean Diet is the current gold standard of healthful eating, per general scientific consensus:
A low-carb diet is best for overall health (and a carb is a carb): True or False?
True-ish and False, respectively. We covered the “a carb is a carb” falsehood earlier, so we’ll look at “a low-carb diet is best”.
Simply put: it can be. One of the biggest problems facing the low-carb diet though is that adherence tends to be poor—that is to say, people crave their carby comfort foods and eat more carbs again. As for the efficacy of a low-carb diet in the context of goals such as weight loss and glycemic control, the evidence is mixed:
❝There is probably little to no difference in weight reduction and changes in cardiovascular risk factors up to two years’ follow-up, when overweight and obese participants without and with T2DM are randomised to either low-carbohydrate or balanced-carbohydrate weight-reducing diets❞
Source: Low-carbohydrate versus balanced-carbohydrate diets for reducing weight and cardiovascular risk
❝On the basis of moderate to low certainty evidence, patients adhering to an LCD for six months may experience remission of diabetes without adverse consequences.
Limitations include continued debate around what constitutes remission of diabetes, as well as the efficacy, safety, and dietary satisfaction of longer term LCDs❞
~ Dr. Joshua Goldenberg et al.
Source: Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission
❝There should be no “one-size-fits-all” eating pattern for different patient´s profiles with diabetes.
It is clinically complex to suggest an ideal percentage of calories from carbohydrates, protein and lipids recommended for all patients with diabetes.❞
Source: Current Evidence Regarding Low-carb Diets for The Metabolic Control of Type-2 Diabetes
We do not need carbs to live; a carnivore diet is viable: True or False?
False. For a simple explanation:
The Carnivore Diet: Can You Have Too Much Meat?
There isn’t a lot of science studying the effects of consuming no plant products, largely because such a study, if anything other than observational population studies, would be unethical. Observational population studies, meanwhile, are not practical because there are so few people who try this, and those who do, do not persist after their first few hospitalizations.
Putting aside the “Carnivore Diet” as a dangerous unscientific fad, if you are inclined to meat-eating, there is some merit to the Paleo Diet, at least for short-term weight loss even if not necessarily long-term health:
What’s The Real Deal With The Paleo Diet?
For longer-term health, we refer you back up to the aforementioned Mediterranean Diet.
Enjoy!
Share This Post
-

I’ve been given opioids after surgery to take at home. What do I need to know?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Opioids are commonly prescribed when you’re discharged from hospital after surgery to help manage pain at home.
These strong painkillers may have unwanted side effects or harms, such as constipation, drowsiness or the risk of dependence.
However, there are steps you can take to minimise those harms and use opioids more safely as you recover from surgery.

Flystock/Shutterstock Which types of opioids are most common?
The most commonly prescribed opioids after surgery in Australia are oxycodone (brand names include Endone, OxyNorm) and tapentadol (Palexia).
In fact, about half of new oxycodone prescriptions in Australia occur after a recent hospital visit.
Most commonly, people will be given immediate-release opioids for their pain. These are quick-acting and are used to manage short-term pain.
Because they work quickly, their dose can be easily adjusted to manage current pain levels. Your doctor will provide instructions on how to adjust the dosage based on your pain levels.
Then there are slow-release opioids, which are specially formulated to slowly release the dose over about half to a full day. These may have “sustained-release”, “controlled-release” or “extended-release” on the box.
Slow-release formulations are primarily used for chronic or long-term pain. The slow-release form means the medicine does not have to be taken as often. However, it takes longer to have an effect compared with immediate-release, so it is not commonly used after surgery.
Controlling your pain after surgery is important. This allows you get up and start moving sooner, and recover faster. Moving around sooner after surgery prevents muscle wasting and harms associated with immobility, such as bed sores and blood clots.
Everyone’s pain levels and needs for pain medicines are different. Pain levels also decrease as your surgical wound heals, so you may need to take less of your medicine as you recover.
But there are also risks
As mentioned above, side effects of opioids include constipation and feeling drowsy or nauseous. The drowsiness can also make you more likely to fall over.
Opioids prescribed to manage pain at home after surgery are usually prescribed for short-term use.
But up to one in ten Australians still take them up to four months after surgery. One study found people didn’t know how to safely stop taking opioids.
Such long-term opioid use may lead to dependence and overdose. It can also reduce the medicine’s effectiveness. That’s because your body becomes used to the opioid and needs more of it to have the same effect.
Dependency and side effects are also more common with slow-release opioids than immediate-release opioids. This is because people are usually on slow-release opioids for longer.
Then there are concerns about “leftover” opioids. One study found 40% of participants were prescribed more than twice the amount they needed.
This results in unused opioids at home, which can be dangerous to the person and their family. Storing leftover opioids at home increases the risk of taking too much, sharing with others inappropriately, and using without doctor supervision.
Don’t stockpile your leftover opioids in your medicine cupboard. Take them to your pharmacy for safe disposal. Archer Photo/Shutterstock How to mimimise the risks
Before using opioids, speak to your doctor or pharmacist about using over-the-counter pain medicines such as paracetamol or anti-inflammatories such as ibuprofen (for example, Nurofen, Brufen) or diclofenac (for example, Voltaren, Fenac).
These can be quite effective at controlling pain and will lessen your need for opioids. They can often be used instead of opioids, but in some cases a combination of both is needed.
Other techniques to manage pain include physiotherapy, exercise, heat packs or ice packs. Speak to your doctor or pharmacist to discuss which techniques would benefit you the most.
However, if you do need opioids, there are some ways to make sure you use them safely and effectively:
- ask for immediate-release rather than slow-release opioids to lower your risk of side effects
- do not drink alcohol or take sleeping tablets while on opioids. This can increase any drowsiness, and lead to reduced alertness and slower breathing
- as you may be at higher risk of falls, remove trip hazards from your home and make sure you can safely get up off the sofa or bed and to the bathroom or kitchen
- before starting opioids, have a plan in place with your doctor or pharmacist about how and when to stop taking them. Opioids after surgery are ideally taken at the lowest possible dose for the shortest length of time.
A heat pack may help with pain relief, so you end up using fewer painkillers. New Africa/Shutterstock If you’re concerned about side effects
If you are concerned about side effects while taking opioids, speak to your pharmacist or doctor. Side effects include:
- constipation – your pharmacist will be able to give you lifestyle advice and recommend laxatives
- drowsiness – do not drive or operate heavy machinery. If you’re trying to stay awake during the day, but keep falling asleep, your dose may be too high and you should contact your doctor
- weakness and slowed breathing – this may be a sign of a more serious side effect such as respiratory depression which requires medical attention. Contact your doctor immediately.
If you’re having trouble stopping opioids
Talk to your doctor or pharmacist if you’re having trouble stopping opioids. They can give you alternatives to manage the pain and provide advice on gradually lowering your dose.
You may experience withdrawal effects, such as agitation, anxiety and insomnia, but your doctor and pharmacist can help you manage these.
How about leftover opioids?
After you have finished using opioids, take any leftovers to your local pharmacy to dispose of them safely, free of charge.
Do not share opioids with others and keep them away from others in the house who do not need them, as opioids can cause unintended harms if not used under the supervision of a medical professional. This could include accidental ingestion by children.
For more information, speak to your pharmacist or doctor. Choosing Wisely Australia also has free online information about managing pain and opioid medicines.
Katelyn Jauregui, PhD Candidate and Clinical Pharmacist, School of Pharmacy, Faculty of Medicine and Health, University of Sydney; Asad Patanwala, Professor, Sydney School of Pharmacy, University of Sydney; Jonathan Penm, Senior lecturer, School of Pharmacy, University of Sydney, and Shania Liu, Postdoctoral Research Fellow, Faculty of Medicine and Dentistry, University of Alberta
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post



Related Posts
-

Oven-Roasted Ratatouille
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a supremely low-effort, high-yield dish. It’s a nutritional tour-de-force, and very pleasing to the tastebuds too. We use flageolet beans in this recipe; they are small immature kidney beans. If they’re not available, using kidney beans or really any other legume is fine.
You will need
- 2 large zucchini, sliced
- 2 red peppers, sliced
- 1 large eggplant, sliced and cut into semicircles
- 1 red onion, thinly sliced
- 2 cans chopped tomatoes
- 2 cans flageolet beans, drained and rinsed (or 2 cups same, cooked, drained, and rinsed)
- ½ bulb garlic, crushed
- 2 tbsp extra virgin olive oil
- 1 tbsp balsamic vinegar
- 1 tbsp black pepper, coarse ground
- 1 tbsp nutritional yeast
- 1 tbsp red chili pepper flakes (omit or adjust per your heat preferences)
- ½ tsp MSG or 1 tsp low-sodium salt
- Mixed herbs, per your preference. It’s hard to go wrong with this one, but we suggest leaning towards either basil and oregano or rosemary and thyme. We also suggest having some finely chopped to go into the dish, and some held back to go on the dish as a garnish.
Method
(we suggest you read everything at least once before doing anything)
1) Preheat the oven to 350℉ / 180℃.
2) Mix all the ingredients (except the tomatoes and herbs) in a big mixing bowl, ensuring even distribution.
2) Add the tomatoes. The reason we didn’t add these before is because it would interfere with the oil being distributed evenly across the vegetables.
3) Transfer to a deep-walled oven tray or an ovenproof dish, and roast for 30 minutes.
4) Stir, add the chopped herbs, stir again, and return to the oven for another 30 minutes.
5) Serve (hot or cold), adding any herb garnish you wish to use.

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Level-Up Your Fiber Intake! (Without Difficulty Or Discomfort)
- Capsaicin For Weight Loss And Against Inflammation
- The Many Health Benefits Of Garlic
- Black Pepper’s Impressive Anti-Cancer Arsenal (And More)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
7 things you can do if you think you sweat too much
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Sweating is our body’s way of cooling down, a bit like an internal air conditioner.
When our core temperature rises (because it’s hot outside, or you’re exercising), sweat glands all over our skin release a watery fluid. As that fluid evaporates, it takes heat with it, keeping us from overheating.
But sweating can vary from person to person. Some people might just get a little dewy under the arms, others feel like they could fill a swimming pool (maybe not that dramatic, but you get the idea).
So what’s a normal amount of sweat? And what’s too much?
ERIK Miheyeu/Shutterstock Why do some people sweat more than others?
How much you sweat depends on a number of factors including:
- your age (young kids generally sweat less than adults)
- your sex (men tend to sweat more than women)
- how active you are.
The average person sweats at the rate of 300 millilitres per hour (at 30°C and about 40% humidity). But as you can’t go around measuring the volume of your own sweat (or weighing it), doctors use another measure to gauge the impact of sweating.
They ask whether sweating interferes with your daily life. Maybe you stop wearing certain clothes because of the sweat stains, or feel embarrassed so don’t go to social events or work.
If so, this is a medical condition called hyperhidrosis, which affects millions of people worldwide.
People with this condition most commonly report problematic armpit sweating, as you’d expect. But sweaty hands, feet, scalp and groin can also be an issue.
Hyperhidrosis can be a symptom of another medical condition, such as an overactive thyroid, fever or menopause.
But hyperhidrosis can have no obvious cause, and the reasons behind this so-called primary hyperhidrosis are a bit of a mystery. People have normal numbers of sweat glands but researchers think they simply over-produce sweat after triggers such as stress, heat, exercise, tobacco, alcohol and hot spices. There may also be a genetic link.
OK, I sweat a lot. What can I do?
1. Antiperspirants
Antiperspirants, particularly ones with aluminium, are your first line of defence and are formulated to reduce sweating. Deodorants only stop body odour.
Aluminum chloride hexahydrate, aluminium chloride or the weaker aluminum zirconium tetrachlorohydrex glycinate react with proteins in the sweat glands, forming a plug. This plug temporarily blocks the sweat ducts, reducing the amount of sweat reaching the skin’s surface.
These products can contain up to 25% aluminium. The higher the percentage the better these products work, but the more they irritate the skin.
Make sure you’re buying antiperspirant and not deodorant. Okrasiuk/Shutterstock 2. Beat the heat
This might seem obvious, but staying cool can make a big difference. That’s because you have less heat to lose, so the body makes less sweat.
Avoid super-hot, long showers (you will have more heat to loose), wear loose-fitting clothes made from breathable fabrics such as cotton (this allows any sweat you do produce to evaporate more readily), and carry a little hand fan to help your sweat evaporate.
When exercising try ice bandanas (ice wrapped in a scarf or cloth, then applied to the body) or wet towels. You can wear these around the neck, head, or wrists to reduce your body temperature.
Try also to modify the time or place you exercise; try to find cool shade or air-conditioned areas when possible.
If you have tried these first two steps and your sweating is still affecting your life, talk to your doctor. They can help you figure out the best way to manage it.
3. Medication
Some medications can help regulate your sweating. Unfortunately some can also give you side effects such as a dry mouth, blurred vision, stomach pain or constipation. So talk to your doctor about what’s best for you.
Your GP may also refer you to a dermatologist – a doctor like myself who specialises in skin conditions – who might recommend different treatments, including some of the following.
4. Botulinum toxin injections
Botulinum toxin injections are not just used for cosmetic reasons. They have many applications in medicine, including blocking the nerves that control the sweat glands. They do this for many months.
A dermatologist usually gives the injections. But they’re only subsidised by Medicare in Australia for the armpits and if you have primary hyperhidrosis that hasn’t been controlled by the strongest antiperspirants. These injections are given up to three times a year. It is not subsidised for other conditions, such as an overactive thyroid or for other areas such as the face or hands.
If you don’t qualify, you can have these injections privately, but it will cost you hundreds of dollars per treatment, which can last up to six months.
Injections are available on Medicare in some cases. Satyrenko/Shutterstock 5. Iontophoresis
This involves using a device that passes a weak electrical current through water to the skin to reducing sweating in the hands, feet or armpits. Scientists aren’t sure exactly how it works.
But this is the only way to control sweating of the hands and feet that does not require drugs, surgery or botulinum toxin injections.
This treatment is not subsidised by Medicare and not all dermatologists provide it. However, you can buy and use your own device, which tends to be cheaper than accessing it privately. You can ask your dermatologist if this is the right option for you.
6. Surgery
There is a procedure to cut certain nerves to the hands that stop them sweating. This is highly effective but can cause sweating to occur elsewhere.
There are also other surgical options, which you can discuss with your doctor.
7. Microwave therapy
This is a newer treatment that zaps your sweat glands to destroy them so they can’t work any more. It’s not super common yet, and it is quite painful. It’s available privately in a few centres.
Michael Freeman, Associate Professor of Dermatology, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Which Comes First, Cardio or Weights? – by Alex Hutchinson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book of questions and answers, myths and busts, and in short, all things exercise.
It’s laid out as many micro-chapters with questions as headers. The explanations are clear and easy to understand, with several citations (of studies and other academic papers) per question.
While it’s quite comprehensive (weighing in at a hefty 300+ pages), it’s not the kind of book where one could just look up any given piece of information that one wants.
Its strength, rather, lies in pre-emptively arming the reader with knowledge, and correcting many commonly-believed myths. It can be read cover-to-cover, or just dipped into per what interests you (the table of contents lists all questions, so it’s easy to flip through).
Bottom line: if you’ve found the world of exercise a little confusing and would like it demystifying, this book will result in a lot of “Oooooh” moments.
Click here to check out Which Comes First, Cardio or Weights?, and know your stuff!
PS: the short answer to the titular question is “mix it up and keep it varied”
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: