Mosquitoes can spread the flesh-eating Buruli ulcer. Here’s how you can protect yourself
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Each year, more and more Victorians become sick with a flesh-eating bacteria known as Buruli ulcer. Last year, 363 people presented with the infection, the highest number since 2004.
But it has been unclear exactly how it spreads, until now. New research shows mosquitoes are infected from biting possums that carry the bacteria. Mozzies spread it to humans through their bite.
What is Buruli ulcer?
Buruli ulcer, also known as Bairnsdale ulcer, is a skin infection caused by the bacterium Mycobacterium ulcerans.
It starts off like a small mosquito bite and over many months, slowly develops into an ulcer, with extensive destruction of the underlying tissue.
While often painless initially, the infection can become very serious. If left untreated, the ulcer can continue to enlarge. This is where it gets its “flesh-eating” name.
Thankfully, it’s treatable. A six to eight week course of specific antibiotics is an effective treatment, sometimes supported with surgery to remove the infected tissue.
Where can you catch it?
The World Health Organization considers Buruli ulcer a neglected tropical skin disease. Cases have been reported across 33 countries, primarily in west and central Africa.
However, since the early 2000s, Buruli ulcer has also been increasingly recorded in coastal Victoria, including suburbs around Melbourne and Geelong.
Scientists have long known Australian native possums were partly responsible for its spread, and suspected mosquitoes also played a role in the increase in cases. New research confirms this.
Our efforts to ‘beat Buruli’
Confirming the role of insects in outbreaks of an infectious disease is achieved by building up corroborating, independent evidence.
In this new research, published in Nature Microbiology, the team (including co-authors Tim Stinear, Stacey Lynch and Peter Mee) conducted extensive surveys across a 350 km² area of Victoria.
We collected mosquitoes and analysed the specimens to determine whether they were carrying the pathogen, and links to infected possums and people. It was like contact tracing for mosquitoes.

Cameron Webb (NSW Health Pathology)
Molecular testing of the mosquito specimens showed that of the two most abundant mosquito species, only Aedes notoscriptus (a widespread species commonly known as the Australian backyard mosquito) was positive for Mycobacterium ulcerans.
We then used genomic tests to show the bacteria found on these mosquitoes matched the bacteria in possum poo and humans with Buruli ulcer.
We further analysed mosquito specimens that contained blood to show Aedes notoscriptus was feeding on both possums and humans.
To then link everything together, geospatial analysis revealed the areas where human Buruli ulcer cases occur overlap with areas where both mosquitoes and possums that harbour Mycobacterium ulcerans are active.
Stop its spread by stopping mozzies breeding
The mosquito in this study primarily responsible for the bacteria’s spread is Aedes notoscriptus, a mosquito that lays its eggs around water in containers in backyard habitats.
Controlling “backyard” mosquitoes is a critical part of reducing the risk of many global mosquito-borne disease, especially dengue and now Buruli ulcer.
You can reduce places where water collects after rainfall, such as potted plant saucers, blocked gutters and drains, unscreened rainwater tanks, and a wide range of plastic buckets and other containers. These should all be either emptied at least weekly or, better yet, thrown away or placed under cover.

Cameron Webb (NSW Health Pathology)
There is a role for insecticides too. While residual insecticides applied to surfaces around the house and garden will reduce mosquito populations, they can also impact other, beneficial, insects. Judicious use of such sprays is recommended. But there are ecological safe insecticides that can be applied to water-filled containers (such as ornamental ponds, fountains, stormwater pits and so on).
Recent research also indicates new mosquito-control approaches that use mosquitoes themselves to spread insecticides may soon be available.
How to protect yourself from bites
The first line of defence will remain personal protection measures against mosquito bites.
Covering up with loose fitted long sleeved shirts, long pants, and covered shoes will provide physical protection from mosquitoes.
Applying topical insect repellent to all exposed areas of skin has been proven to provide safe and effective protection from mosquito bites. Repellents should include diethytolumide (DEET), picaridin or oil of lemon eucalyptus.
While the rise in Buruli ulcer is a significant health concern, so too are many other mosquito-borne diseases. The steps to avoid mosquito bites and exposure to Mycobacteriam ulcerans will also protect against viruses such as Ross River, Barmah Forest, Japanese encephalitis, and Murray Valley encephalitis.![]()
Cameron Webb, Clinical Associate Professor and Principal Hospital Scientist, University of Sydney; Peter Mee, Adjunct Associate Lecturer, School of Applied Systems Biology, La Trobe University; Stacey Lynch, Team Leader- Mammalian infection disease research, CSIRO, and Tim Stinear, Professor of Microbiology, The University of Melbourne
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Not To Be A Night Owl After 40

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s often assumed that being an “early bird” or a “night owl” is purely a matter of genetic predisposition, and… There is indeed a genetic influence, but as it is said, “genes predispose; they don’t predetermine“.
We discussed this in detail, here: Early Bird Or Night Owl? Genes vs Environment
With that in mind, being a night owl is, for most of us, largely a modifiable thing. Some people, of course, will have things going on in their life that preclude getting an early night’s sleep, but if that’s not the case for you, then we do recommend considering shifting your chronotype to being an “early bird”, if it’s not already there.
For more about chronotypes in general, see: 5 Sleep Phenotypes, By Actual Science (Sleep Tracking, For Five Million Nights)
Why does it matter?
A team of researchers (Dr. Ana Wenzler et al.) did a large (n=23,798) study and found that night owls face a higher risk of cognitive decline compared to morning people.
As to why “after 40”, there are two reasons:
- Biological clocks shift throughout life: people tend to be morning types in childhood, shift to evening types in adolescence, and most, but far from all, return to morning preference by around age 40.
- Cognitive decline naturally begins most commonly after age 40, and lifestyle factors influence this process.
For this reason, the study used data from people over the age of 40, to analyze people’s chronotypes (natural sleep patterns) and their behavior over a 10-year period.
As to how much being a night owl affects the risk of cognitive decline; it was broken down by demographics, but for example in the group with the highest education level:
❝each one-hour increase in chronotype corresponded to a 0.80-point decline in cognition per decade (95 % CI: -1.34, -0.26)❞
The “night owl” chronotype was also associated with greater decline in non-verbal fluency and executive functioning among higher educated participants, highlighting the importance of targeted prevention strategies.
In terms of potentially confounding (although also relevant) factors, night owls tend to engage more in unhealthy behaviors such as smoking, drinking, poor diet, and lack of exercise—especially in the evening.
You may be thinking: “I don’t do those things”, in which case, great! But the researchers also calculated that those behaviors explain only about 25% of the cognitive decline risk among night owls.
You can read the paper in full, here: Chronotype as a potential risk factor for cognitive decline: The mediating role of sleep quality and health behaviours in a 10-year follow-up study
How should we fix it?
If you’re currently a night owl, chances are you physically cannot currently sleep earlier than you do—your brain just isn’t ready to sleep yet at the earlier hour.
What you can control, however, is your getting-up time. So, shift that earlier—gently! 15 minutes earlier per day is great—and your “getting sleepy time” in the evening will naturally shift commensurately earlier.
For reference, see also: Calculate (And Enjoy) The Perfect Night’s Sleep
Take care!
Share This Post
-

Avocado Oil vs Olive Oil – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing avocado oil to olive oil, we picked the olive oil.
Why?
Avocados and olives are both very healthy foods. However, when they are made into oils, there’s an important distinguishing factor:
Olive oil usually retains a lot of the micronutrients from the olives (including vitamins E and K), whereas no measurable micronutrients usually remain in avocado oil.
So while both olive oil and avocado oil have a similar (excellent; very heart-healthy!) lipids profile, the olive oil has some bonuses that the avocado oil doesn’t.
We haven’t written about the nutritional profiles of either avocados or olives yet, but here’s what we had to say on the different kinds of olive oil available:
And here’s an example of a good one on Amazon, for your convenience 😎
Share This Post
-
Parsnips vs Potatoes – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing parsnips to potatoes, we picked the parsnips.
Why?
To be more specific, we’re looking at russet potatoes, and in both cases we’re looking at cooked without fat or salt, and with the skin on. In other words, the basic nutritional values of these plants in their edible form, without adding anything. With this in mind, once we get to the root of things (so to speak), there’s a clear winner:
Looking at the macros first, parsnips have more fiber, while potatoes have more carbs. Potatoes do have more protein too, but given the small numbers involved when it comes to protein we don’t think this is enough of a plus to outweigh the extra fiber in the parsnips. So, that’s a win for parsnips in this category.
In the category of vitamins, again a champion emerges: parsnips have more of vitamins B1, B2, B5, B9, C, E, and K, while potatoes have more of vitamins B3 and B6. So, a 7:2 win for parsnips here!
When it comes to minerals, parsnips have more calcium copper, manganese, selenium, and zinc, while potatoes have more iron and potassium. Potatoes do also have more sodium, but for most people most of the time, this is not a plus, healthwise. Disregarding the sodium, this category sees a 5:2 win for parsnips.
Adding up the sections makes a clear overall win for parsnips, but by all means enjoy either or both (in moderation, as with all starchy vegetables), as diversity is good!
Want to learn more?
You might like to read:
Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
Take care!
Share This Post



Related Posts
-

Ear Candling: Is It Safe & Does It Work?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Does This Practice Really Hold A Candle To Evidence-Based Medicine?

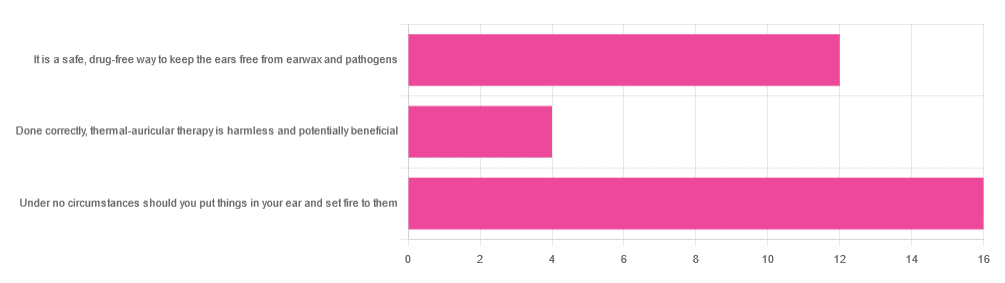
In Tuesday’s newsletter, we asked you your opinion of ear candling, and got the above-depicted, below-described set of responses:
- Exactly 50% said “Under no circumstances should you put things in your ear and set fire to them”
- About 38% said “It is a safe, drug-free way to keep the ears free from earwax and pathogens”
- About 13% said “Done correctly, thermal-auricular therapy is harmless and potentially beneficial”
This means that if we add the two positive-to-candling answers together, it’s a perfect 50:50 split between “do it” and “don’t do it”.
(Yes, 38%+13%=51%, but that’s because we round to the nearest integer in these reports, and more precisely it was 37.5% and 12.5%)
So, with the vote split, what does the science say?
First, a quick bit of background: nobody seems keen to admit to having invented this. One of the major manufacturers of ear candles refers to them as “Hopi” candles, which the actual Hopi tribe has spent a long time asking them not to do, as it is not and never has been used by the Hopi people. Other proposed origins offered by advocates of ear candling include Traditional Chinese Medicine (not used), Ancient Egypt (no evidence of such whatsoever), and Atlantis:
Quackwatch | Why Ear Candling Is Not A Good Idea
It is a safe, drug-free way to keep the ears free from earwax and pathogens: True or False?
False! In a lot of cases of alternative therapy claims, there’s an absence of evidence that doesn’t necessarily disprove the treatment. In this case, however, it’s not even an open matter; its claims have been actively disproven by experimentation:
- It doesn’t remove earwax; on the contrary, experimentation “showed no removal of cerumen from the external auditory canal. Candle wax was actually deposited in some“
- It doesn’t remove pathogens, and the proposed mechanism of action for removing pathogens, that of the “chimney effect”: the idea that the burning candle creates a vacuum that draws wax out of the ear along with debris and bacteria, simply does not work; on the contrary, “Tympanometric measurements in an ear canal model demonstrated that ear candles do not produce negative pressure”.
- It isn’t safe; on the contrary, “Ear candles have no benefit in the management of cerumen and may result in serious injury”
In a medium-sized survey (n=122), the following injuries were reported:
- 13 x burns
- 7 x occlusion of the ear canal
- 6 x temporary hearing loss
- 3 x otitis externa (this also called “swimmer’s ear”, and is an inflammation of the ear, accompanied by pain and swelling)
- 1 x tympanic membrane perforation
Indeed, authors of one paper concluded:
❝Ear candling appears to be popular and is heavily advertised with claims that could seem scientific to lay people. However, its claimed mechanism of action has not been verified, no positive clinical effect has been reliably recorded, and it is associated with considerable risk.
No evidence suggests that ear candling is an effective treatment for any condition. On this basis, we believe it can do more harm than good and we recommend that GPs discourage its use❞
Source: Canadian Family Physician | Ear Candling
Under no circumstances should you put things in your ear and set fire to them: True or False?
True! It’s generally considered good advice to not put objects in general in your ears.
Inserting flaming objects is a definite no-no. Please leave that for the Cirque du Soleil.
You may be thinking, “but I have done this and suffered no ill effects”, which seems reasonable, but is an example of survivorship bias in action—it doesn’t make the thing in question any safer, it just means you were one of the one of the ones who got away unscathed.
If you’re wondering what to do instead… Ear oils can help with the removal of earwax (if you don’t want to go get it sucked out at a clinic—the industry standard is to use a suction device, which actually does what ear candles claim to do). For information on safely getting rid of earwax, see our previous article:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Good Energy – by Dr. Casey Means
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For a book with a title like “Good Energy” and chapters such as “Bad Energy Is the Root of Disease”, this is actually a very science-based book (and there are a flock of well-known doctors saying so in the “praise for” section, too).
The premise is simple: most of our health is a matter of what our metabolism is (or isn’t) doing, and it’s not just a case of “doing more” or “doing less”. Indeed, a lot of “our” energy is expended doing bad things (such as chronic inflammation, to give an obvious example).
Dr. Means outlines about a dozen things many people do wrong, and about a dozen things we can do right, to get our body’s energy system working for us, rather than against us.
The style here is pop-science throughout, and in the category of criticism, the bibliography is offloaded to her website (we prefer to have things in our hands). However, the information here is good, clearly-presented, and usefully actionable.
Bottom line: if you ever find yourself feeling run-down and like your body is using your resources against you rather than for you, this is the book to get you out of that slump!
Click here to check out Good Energy, and get your metabolism working for you!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Seeing the same midwife or doctor in pregnancy and labour reduces the risk of birth trauma
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Every pregnant woman wants to deliver a healthy baby. During labour and birth, women also want to feel listened to and respected, and to come out of the experience physically and emotionally well.
But around 28% of Australian women describe their most recent birth as traumatic.
Birth trauma can include fear for their life or their baby’s life, a loss of control, damage to the perineum or pelvic floor, disrespectful care, or mistreatment from health care providers.
Our new research paper examined birth outcomes and both physical and psychological experiences of women and babies who experienced five different types (or models) of care in Australia during the COVID pandemic.
We found that seeing the same midwife or team of midwives was associated with lower rates of intervention and birth trauma, compared with standard care.
And for some women, private obstetric care also led to lower rates of birth trauma than standard care in the public system. Let’s take a look.

Fly View Productions/Getty Images Five main models of care
Most Australian women receive standard public care or GP shared care.
In standard public care, women see rotating hospital staff (midwives, obstetricians and at times, trainees) throughout pregnancy and often give birth with a midwife or doctor they’ve never met.
GP shared care is when there is an arrangement between a GP and hospital. Women see their GP most during pregnancy and hospital staff for some antenatal appointments. The GP doesn’t usually attend the birth, except in some rural, remote regions.
In continuity of care models, one or a small number of midwives and obstetricians deliver the majority of the care before, during and after birth. This includes continuity of:
- midwifery care in the public system
- private obstetric care
- private midwifery care.
When given a choice, women favour continuity of care models.
What our study found
Our study looked at the experiences of 3,682 Australian women who gave birth in 2020 and 2021.
Compared to women who had standard care, we found that those who had continuity of midwifery care (through the public system or a private midwife) were:
- less likely to be induced or have an oxytocin drip to speed up labour
- much more likely to have a vaginal birth
- more likely to have the midwife visit them at home after the birth
- less likely to have a caesarean section
- less likely to have their baby admitted to special or neonatal intensive care or receive formula in hospital when they had chosen to breastfeed
- half as likely to describe their birth as traumatic.
These differences were seen even after adjusting for differences in the groups that could affect outcomes, such as women’s age, medical risk, education, employment status, country of birth, income and mental health.
These findings line up with decades of evidence. A 2024 Cochrane review of 17 randomised controlled trials found midwifery continuity of care models reduce some birth interventions, including caesarean section, forceps and vacuum birth, and episiotomy (surgical cut to the perineum).
Our study also found that while women who had private obstetric care had higher rates of birth intervention, they had lower rates of birth trauma when compared to standard care. There was no difference in outcomes for the baby, such as admission to special care or neonatal intensive care.
This suggests when women’s choices align with their care provider’s philosophy, outcomes are better – even if intervention levels are higher. Some women seek, or are not concerned about, increased obstetric intervention. Continuity itself, regardless of who the lead health care professional is, reduces birth trauma.
What are the study’s limitations?
As with any study there are limitations. This study relied on women reporting their labour and birth outcomes, so there could be difficulties with recall that affected reporting of some health risks and other important information.
A high proportion of women responding (86%) were born in Australia and spoke English at home (92%) and only 2% were Aboriginal or Torres Strait Islander, meaning the diversity of the Australian population is not represented.
We did not examine stillbirth or neonatal deaths as all the women responding to the survey had a live baby. So people still could have had those experiences but they weren’t captured in our data.
Why does continuity of care make a difference?
Continuity gives women a stable, familiar guide who knows their story, understands their concerns and advocates for them when the system is under strain.
It also allows for the kind of personalised care women consistently say they want and which midwives wish they could deliver more often.
Nearly half of all models of care (49%) have a midwife as the designated carer, with 16% having midwifery continuity of care throughout the maternity period.
However, midwifery continuity of care models are more common in urban centres and can be harder to access in rural and remote areas. Even in urban centres, not everyone who wants to access them can. The popularity of these programs means they fill up fast and many women miss out if they don’t book in when they are first pregnant.
Private obstetric and private midwifery models of care come with out of pocket costs and are not available everywhere. There are few private midwives and many struggle to get admitting rights into hospitals like doctors have.
The recent New South Wales Birth Trauma Inquiry recommended expanding continuity of care models to help reduce the high rates of birth trauma in Australia. Our study shows that this could make a significant difference.
Hannah Dahlen, Professor of Midwifery, Associate Dean Research and HDR, Midwifery Discipline Leader, Western Sydney University; Hazel Keedle, Associate Professor of Midwifery, Western Sydney University, and Kingsley Emwinyore Agho, Professor of Biostatistics and Global Health, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: