Magic mushrooms may one day treat anorexia, but not just yet
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anorexia nervosa is a severe mental health disorder where people fear weight gain. Those with the disorder have distorted body image and hold rigid beliefs their body is too big. They typically manage this through restricted eating, leading to the serious medical consequences of malnutrition.
Anorexia has one of the highest death rates of any mental illness. Yet there are currently no effective drug treatments and the outcomes of psychotherapy (talk therapy) are poor. So we’re desperately in need of new and improved treatments.
Psilocybin, commonly known as magic mushrooms, is one such novel treatment. But while it shows early promise, you won’t see it used in clinical practice just yet – more research is needed to test if it’s safe and effective.

What does treatment involve?
The treatment involves the patient taking a dose of psilocybin in a safe environment, which is usually a specifically set up clinic. The patient undergoes preparation therapy before the dosing session and integration therapy after.
Psilocybin, extracted from mushrooms, is a psychedelic, which means it can produce altered thinking, sense of time and emotions, and can often result in hallucinations. It also has the potential to shift patients out of their rigid thinking patterns.
Psilocybin is not administered alone but instead with combined structured psychotherapy sessions to help the patient make sense of their experiences and the changes to their thinking. This is an important part of the treatment.
What does the research show?
Research has shown improved effects of psilocybin-assisted psychotherapy after one or two dosing sessions, a couple of weeks apart. Most research to date has targeted depression.
Psilocybin has been found to increase cognitive flexibility – our ability to adjust our thinking patterns according to changing environments or demands. This is one of the ways researchers believe psilocybin might improve symptoms for conditions such as depression and alcohol use disorder, which are marked by rigid thinking styles.
People with anorexia similarly struggle with rigid thinking patterns. So researchers and clinicians have recently turned their attention to anorexia.
In 2023, a small pilot study of ten women with anorexia was published in the journal Nature Medicine. It showed psilocybin-assisted psychotherapy (with 25mg of psilocybin) was safe and acceptable. There were no significant side effects and participants reported having valuable experiences.
Although the trial was not a formal efficacy trial, 40% of the patients did have significant drops in their eating disorder behaviour.
However, the trial only had one dosing session and no long-term follow up, so further research is needed.

A recent animal study using rats examined whether rigid thinking could be improved in rats when given psilocybin. After the psilocybin, rats gained weight and had more flexible thinking (using a reversal learning task).
These positive changes were related to the serotonin neurotransmitter system, which regulates mood, behaviour and satiety (feeling full).
Brain imaging studies in humans show serotonin disturbances in people with anorexia. Psilocybin-assisted psychotherapy is showing promise at modifying the serotonin disturbances and cognitive inflexibility that have been shown to be problematic in anorexia.
Research with animals can provide unique insights into the brain which can sometimes not be investigated in living humans. But animal models can never truly mimic human behaviour and the complex nature of chronic mental health conditions.
What’s next for research?
Further clinical trials in humans are very much needed – and are underway from a research team at the University of Sydney and ours at Swinburne.
Our trial will involve an initial 5mg dose followed by two subsequent doses of 25mg, several weeks apart. An initial low dose aims to help participants prepare for what is likely to be a new and somewhat unpredictable experience.
Our trial will examine the usefulness of providing psychotherapy that directly addresses body image disturbance. We are also investigating if including a family member or close friend in the treatment increases support for their loved one.

Data from other mental health conditions has suggested that not everyone sees benefits, with some people having bad trips and a deterioration in their mental health. So this treatment won’t be for everyone. It’s important to work out who is most likely to respond and under what conditions.
New trials and those underway will be critical in understanding whether psilocybin-assisted psychotherapy is a safe and effective treatment for anorexia, and the optimal conditions to improve the patient’s response. But we are some way off from seeing this treatment in the clinic. One of the big issues being the cost of this intervention and how this will be funded.
Susan Rossell, Director Clinical Trials and Professor Cognitive Neuropsychiatry Centre for Mental Health and Brain Sciences, Swinburne University of Technology and Claire Finkelstein, Clinical Psychologist and PhD candidate, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Eggs: Nutritional Powerhouse or Heart-Health Timebomb?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Eggs: All Things In Moderation?

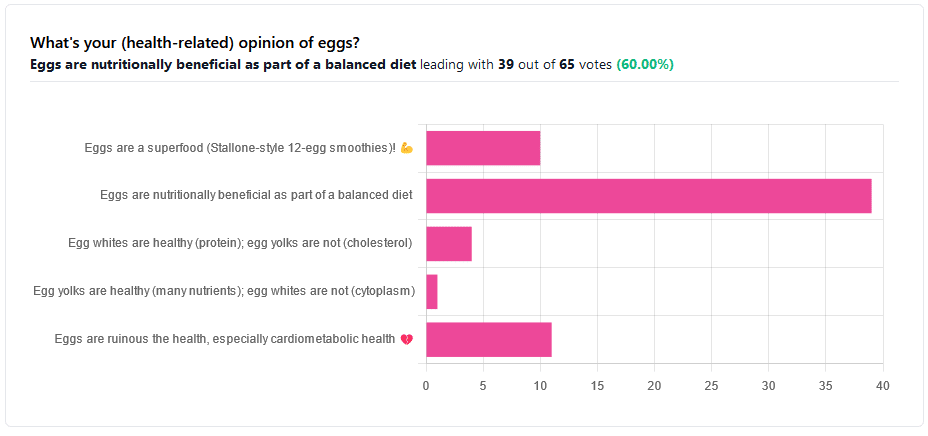
We asked you for your (health-related) opinion on eggs. We specified that, for the sake of simplicity, let’s say that they are from happy healthy backyard hens who enjoy a good diet.
Apparently this one wasn’t as controversial as it might have been! We (for myth-busting purposes) try to pick something polarizing and sometimes even contentious for our Friday editions, and pick apart what science lies underneath public perceptions.
However, more than half (in fact, 60%) of the subscribers who voted in the poll voted for “Eggs are nutritionally beneficial as part of a balanced diet”, which very moderate statement is indeed pretty much the global scientific consensus.
Still, we’ve a main feature to write, so let’s look at the science, and what the other 40% had in mind:
Eggs are ruinous to health, especially cardiometabolic health: True or False?
False, per best current science, anyway!
Scientific consensus has changed over the years. We learned about cholesterol, then we learned about different types of cholesterol, and now we’ve even learned about in some instances even elevated levels of “bad” cholesterol aren’t necessarily a cause of cardiometabolic disorders so much as a symptom—especially in women.
Not to derail this main feature about eggs (rather than just cholesterol), but for those who missed it, this is actually really interesting: basically, research (pertaining to the use of statins) has found that in women, higher LDL levels aren’t anywhere near the same kind of risk factor as they are for men, and thus may mean that statins (whose main job is reducing LDL) may be much less helpful for women than for men, and more likely to cause unwanted serious side effects in women.
Check out our previous main feature about this: Statins: His & Hers?
But, for back on topic, several large studies (totalling 177,000 people in long-term studies in 50 countries) found:
❝Results from the three cohorts and from the updated meta-analysis show that moderate egg consumption (up to one egg per day) is not associated with cardiovascular disease risk overall, and is associated with potentially lower cardiovascular disease risk in Asian populations.❞
Egg whites are healthy (protein); egg yolks are not (cholesterol): True or False?
True and False, respectively. That is to say, egg whites are healthy (protein), and egg yolks are also healthy (many nutrients).
We talked a bit already about cholesterol, so we’ll not rehash that here. As to the rest:
Eggs are one of the most nutritionally dense foods around. After all, they have everything required to allow a cluster of cells to become a whole baby chick. That’s a lot of body-building!
They’re even more nutritionally heavy-hitters if you get omega-3 enriched eggs, which means the hens were fed extra omega-3, usually in the form of flax seeds.
Also, free-range is better healthwise than others. Do bear in mind that unless they really are from your backyard, or a neighbor’s, chances are that the reality is not what the advertising depicts, though. There are industry minimum standards to be able to advertise as “free-range”, and those standards are a) quite low b) often ignored, because an occasional fine is cheaper than maintaining good conditions.
So if you can look after your own hens, or get them from somewhere that you can see for yourself how they are looked after, so much the better!
Check out the differences side-by-side, though:
Pastured vs Omega-3 vs “Conventional” Eggs: What’s the Difference?
Stallone-style 12-egg smoothies are healthy: True or False?
False, at least if taken with any regularity. One can indeed have too much of a good thing.
So, what’s the “right amount” to eat?
It may vary depending on individual factors (including age and ethnicity), but a good average, according to science, is to keep it to 3 eggs or fewer per day. There are a lot of studies, but we only have so much room here, so we’ll pick one. Its findings are representative of (and in keeping with) the many other studies we looked at, so this seems uncontroversial scientifically:
❝Intake of 1 egg/d was sufficient to increase HDL function and large-LDL particle concentration; however, intake of 2-3 eggs/d supported greater improvements in HDL function as well as increased plasma carotenoids. Overall, intake of ≤3 eggs/d favored a less atherogenic LDL particle profile, improved HDL function, and increased plasma antioxidants in young, healthy adults.❞
Enjoy!
Share This Post
-

The Snooze-Button Controversy
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
To Snooze Or Not To Snooze? (Science Has Answers)

This is Dr. Jennifer Kanaan. She’s a medical doctor with a focus on pulmonary critical care, sleep disorders, and sleep medicine.
What does she want to tell us?
She wants us to be wary of the many news articles that have jumped on a certain recent sleep study, such as:
- Is hitting the snooze button really a bad idea? Study sheds light on the impact of morning alarms on sleep and cognition
- Hitting Snooze May Help You Feel Less Sleepy and More Alert, Research Says
- Is it okay to press the snooze button?
- Hitting Snooze May Help You Feel Less Sleepy and More Alert, Research Says
- Hitting the snooze button on your alarm doesn’t make you more tired
For the curious, here is the paper itself, by Dr. Tina Sundelin et al. It’s actually two studies, by the way, but one paper:
The authors of this study concluded:
❝There were no clear effects of snoozing on the cortisol awakening response, morning sleepiness, mood, or overnight sleep architecture.
A brief snooze period may thus help alleviate sleep inertia, without substantially disturbing sleep, for late chronotypes and those with morning drowsiness.❞
Notably, people tend to snooze because an alarm clock will, if not “smart” about it, wake us up mid sleep-cycle more often than not, and that will produce a short “sleep hangover”. By snoozing, we are basically re-rolling the dice on being woken up between sleep cycles, and thus feeling more refreshed.
What’s Dr. Kanaan’s counterpoint?
Dr. Kanaan says:
❝If you’re coming in and out of sleep for 30 minutes, after the alarm goes off the first time, you’re costing yourself 30 minutes of uninterrupted, quality, restorative sleep. This study doesn’t change that fact.❞
She advises that rather than snoozing, we should prioritize getting good sleep in the first place, and once we do wake up, mid sleep-cycle or not, get sunlight. That way, our brain will start promptly scrubbing melatonin and producing the appropriate wakefulness hormones instead. That means serotonin, and also a spike of cortisol.
Remember: cortisol is only bad when it’s chronically elevated. It’s fine, and even beneficial, to have a short spike of cortisol. We make it for a reason!
If you’d like to hear more from Dr. Kanaan, you might like this interview with her at the University of Connecticut:
Want the best of both worlds?
A great option to avoid getting woken in the middle of a sleep cycle, and also not needing to hit snooze, is a sunrise alarm clock. Specifics of these devices vary, but for example, the kind this writer has starts gently glowing an hour before the set alarm time,and gradually gets brighter and lighter over the course of the hour.
We don’t sell them, but here’s an example sunrise alarm clock on Amazon, for your convenience
Share This Post
-

Cleaning Up Your Mental Mess – by Dr. Caroline Leaf
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
First of all, what mental mess is this? Well, that depends on you, but common items include:
- Anxiety
- Depression
- Stress
- Trauma
Dr. Caroline Leaf also includes the more nebulous item “toxic thoughts”, but this is mostly a catch-all term.
Given that it says “5 simple scientifically proven steps”, it would be fair if you are wondering:
“Is this going to be just basic CBT stuff?”
And… First, let’s not knock basic CBT stuff. It’s not a panacea, but it’s a great tool for a lot of things. However… Also, no, this book is not about just basic CBT stuff.
In fact, this book’s methods are presented in such a novel way that this reviewer was taken aback by how unlike it was to anything she’d read before.
And, it’s not that the components themselves are new—it’s just that they’re put together differently, in a much more organized comprehensive and systematic way, so that a lot less stuff falls through the cracks (a common problem with standalone psychological tools and techniques).
Bottom line: if you buy one mental health self-help book this year, we recommend that it be this one
Click here to check out Cleaning Up Your Mental Mess, and take a load off your mind!
Share This Post
-

Should We Skip Shampoo?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝What’s the science on “no poo”? Is it really better for hair? There are so many mixed reports out there.❞
First, for any unfamiliar: this is not about constipation; rather, it is about skipping shampoo, and either:
- Using an alternative cleaning agent, such as vinegar and/or sodium bicarbonate
- Using nothing at all, just conditioner when wet and brushing when dry
Let’s examine why the trend became a thing: the thinking went “shampoo does not exist in nature, and most of our body is more or less self-cleaning; shampoos remove oils from hair, and the body has to produce more sebum to compensate, resulting in a rapid cycle of dry and greasy hair”.
Now let’s fact-check each of those:
- shampoo does not exist in nature: true (except in the sense that everything that exists can be argued to exist in nature, since nature encompasses everything—but the point is that shampoo is a purely artificial human invention)
- most of our body is more or less self-cleaning: true, but our hair is not, for the same reason our nails are not: they’re not really a living part of the overall organism that is our body, so much as a keratinous protrusion of neatly stacked and hardened dead cells from our body. Dead things are not self-cleaning.
- shampoos remove oils from hair: true; that is what they were invented for and they do it well
- the body has to produce more sebum to compensate, resulting in a rapid cycle of dry and greasy hair: false; or at least, there is no evidence for this.
Our hair’s natural oils are great at protecting it, and also great at getting dirt stuck in it. For the former reason we want the oil there; for the latter reason, we don’t.
So the trick becomes: how to remove the oil (and thus the dirt stuck in it) and then put clean oil back (but not too much, because we don’t want it greasy, just, shiny and not dry)?
The popular answer is: shampoo to clean the hair, conditioner to put an appropriate amount of oil* back.
*these days, mostly not actually oil, but rather silicon-based substitutes, that do the same job of protecting hair and keeping it shiny and not brittle, without attracting so much dirt. Remember also that silicon is inert and very body safe; its molecules are simply too large to be absorbed, which is why it gets used in hair products, some skin products, and lube.
See also: Water-based Lubricant vs Silicon-based Lubricant – Which is Healthier?
If you go “no poo”, then what will happen is either you dry your hair out much worse by using vinegar or (even worse) bicarbonate of soda, or you just have oil (and any dirt stuck in it) in your hair for the life of the hair. As in, each individual strand of hair has a lifespan, and when it falls out, the dirt will go with it. But until that day, it’s staying with you, oil and dirt and all.
If you use a conditioner after using those “more natural” harsh cleaners* that aren’t shampoo, then you’ll undo a lot of the damage done, and you’ll probably be fine.
*in fact, if you’re going to skip shampoo, then instead of vinegar or bicarbonate of soda, dish soap from your kitchen may actually do less damage, because at least it’s pH-balanced. However, please don’t use that either.
If you’re going to err one way or the other with regard to pH though, erring on the side of slightly acidic is much better than slightly alkaline.
More on pH: Journal of Trichology | The Shampoo pH can Affect the Hair: Myth or Reality?
If you use nothing, then brushing a lot will mitigate some of the accumulation of dirt, but honestly, it’s never going to be clean until you clean it.
Our recommendation
When your hair seems dirty, and not before, wash it with a simple shampoo (most have far too many unnecessary ingredients; it just needs a simple detergent, and the rest is basically for marketing; to make it foam completely unnecessarily but people like foam, to make it thicker so it feels more substantial, to make it smell nice, to make it a color that gives us confidence it has ingredients in it, etc).
Then, after rinsing, enjoy a nice conditioner. Again there are usually a lot of unnecessary ingredients, but an argument can be made this time for some being more relevant as unlike with the shampoo, many ingredients are going to remain on your hair after rinsing.
Between washes, if you have long hair, consider putting some hair-friendly oil (such as argan oil or coconut oil) on the tips daily, to avoid split ends.
And if you have tight curly hair, then this advice goes double for you, because it takes a lot longer for natural oils to get from your scalp to the ends of your hair. For those of us with straight hair, it pretty much zips straight on down there within a day or two; not so if you have beautiful 4C curls to take care of!
For more on taking care of hair gently, check out:
Gentler Hair Care Options, According To Science
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Tomato vs Cucumber – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing tomato to cucumber, we picked the tomato.
Why?
Both are certainly great, but there are some nutritional factors between them:
In terms of macros, everything is approximately equal except that tomato has more than 2x the fiber, so that’s a win for tomato.
When it comes to vitamins, tomatoes have more of vitamins A, B1, B3, B6, B9, C, E, and choline, while cucumber has more of vitamins B2, B5, and K. In short, an 8:3 victory for tomatoes.
In the category of minerals, tomatoes have more copper, potassium, and manganese, while cucumber has more calcium, iron, magnesium, selenium, and zinc. So, a win for cucumber this time.
Both have useful phytochemical properties, too; tomatoes are rich in lycopene which has many benefits, and cucumbers have powerful anti-inflammatory powers whose mechanism of action is not yet fully understood—see the links below for more details!
All in all, enjoy either or both (they make a great salad chopped roughly together with some olives, a little garlic, and a drizzle of olive oil and balsamic vinegar with a twist or three of black pepper), but if you have to pick just one (what a cruel world), we say the tomato has the most benefits, on balance.
Want to learn more?
You might like to read:
- Lycopene’s Benefits For The Gut, Heart, Brain, & More
- Cucumber Extract Beats Glucosamine & Chondroitin… At 1/135th Of The Dose?!
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hormone Replacement
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝I cant believe 10 Almonds addresses questions. Thanks. I see the word symptoms for menopause. I don’t know what word should replace it but maybe one should be used or is symptom accurate? And I recently read that there was a great disservice for women in my era as they were denied/scared of hormones replacement. Unnecessarily❞
You’d better believe it! In fact we love questions; they give us things to research and write about.
“Symptom” is indeed an entirely justified word to use, being:
- General: any phenomenon or circumstance accompanying something and serving as evidence of it.
- Medical: any phenomenon that arises from and accompanies a particular disease or disorder and serves as an indication of it.
If the question is more whether the menopause can be considered a disease/disorder, well, it’s a naturally occurring and ultimately inevitable change, yes, but then, so is cancer (it’s in the simple mathematics of DNA replication and mutation that, unless a cure for cancer is found, we will always eventually get cancer, if nothing else kills us first).
So, something being natural/inevitable isn’t a reason to not consider it a disease/disorder, nor a reason to not treat it as appropriate if it is causing us harm/discomfort that can be safely alleviated.
Moreover, and semantics aside, it is medical convention to consider menopause to be a medical condition, that has symptoms. Indeed, for example, the US’s NIH (and its constituent NIA, the National Institute of Aging) and the UK’s NHS, both list the menopause’s symptoms, using that word:
- NIA (NIH): What are the signs and symptoms of menopause?
- NHS: Common symptoms of menopause and perimenopause
With regard to fearmongering around HRT, certainly that has been rife, and there were some very flawed (and later soundly refuted) studies a while back that prompted this—and even those flawed studies were not about the same (bioidentical) hormones available today, in any case. So even if they had been correct (they weren’t), it still wouldn’t be a reason to not get treatment nowadays, if appropriate!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: