How Likely Are You To Live To 100?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How much hope can we reasonably have of reaching 100?
Yesterday, we asked you: assuming a good Health-Related Quality of Life (HRQoL), how much longer do you hope to live?
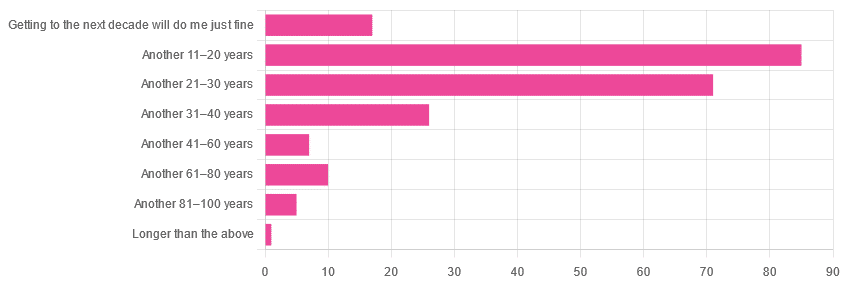
We got the above-depicted, below-described, set of responses:
- A little over 38% of respondents hope to live another 11–20 years
- A little over 31% hope to live another 31–40 years
- A little over 7% will be content to make it to the next decade
- One (1) respondent hopes to live longer than an additional 100 years
This is interesting when we put it against our graph of how old our subscribers are:
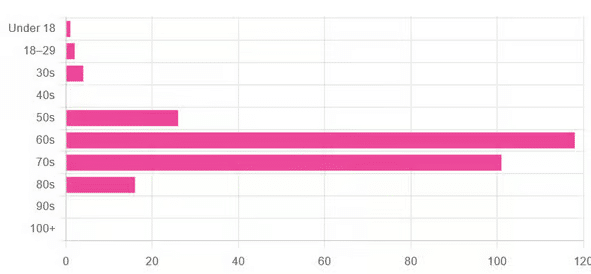
…because it corresponds inversely, right down to the gap/dent in the 40s. And—we may hypothesize—that one person under 18 who hopes to live to 120, perhaps.
This suggests that optimism remains more or less constant, with just a few wobbles that would probably be un-wobbled with a larger sample size.
In other words: most of our education-minded, health-conscious subscriber-base hope to make it to the age of 90-something, while for the most part feeling that 100+ is overly optimistic.
Writer’s anecdote: once upon a time, I was at a longevity conference in Brussels, and a speaker did a similar survey, but by show of hands. He started low by asking “put your hands up if you want to live at least a few more minutes”. I did so, with an urgency that made him laugh, and say “Don’t worry; I don’t have a gun hidden up here!”
Conjecture aside… What does the science say about our optimism?
First of all, a quick recap…
To not give you the same information twice, let’s note we did an “aging mythbusting” piece already covering:
- Aging is inevitable: True or False?
- Aging is, and always will be, unstoppable: True or False?
- We can slow aging: True or False?
- It’s too early to worry about… / It’s too late to do anything about… True or False?
- We can halt aging: True or False?
- We can reverse aging: True or False?
- But those aren’t really being younger, we’ll still die when our time is up: True or False?
You can read the answers to all of those here:
Age & Aging: What Can (And Can’t) We Do About It?
Now, onwards…
It is unreasonable to expect to live past 100: True or False?
True or False, depending on your own circumstances.
First, external circumstances: the modal average person in Hong Kong is currently in their 50s and can expect to live into their late 80s, while the modal average person in Gaza is 14 and may not expect to make it to 15 right now.
To avoid extremes, let’s look at the US, where the modal average person is currently in their 30s and can expect to live into their 70s:
United States Mortality Database
Now, before that unduly worries our many readers already in their 70s…
Next, personal circumstances: not just your health, but your socioeconomic standing. And in the US, one of the biggest factors is the kind of health insurance one has:
SOA Research Institute | Life Expectancy Calculator 2021
You may note that the above source puts all groups into a life expectancy in the 80s—whereas the previous source gave 70s.
Why is this? It’s because the SOA, whose primary job is calculating life insurance risks, is working from a sample of people who have, or are applying for, life insurance. So it misses out many people who die younger without such.
New advances in medical technology are helping people to live longer: True or False?
True, assuming access to those. Our subscribers are mostly in North America, and have an economic position that affords good access to healthcare. But beware…
On the one hand:
The number of people who live past the age of 100 has been on the rise for decades
On the other hand:
The average life expectancy in the U.S. has been on the decline for three consecutive years
COVID is, of course, largely to blame for that, though:
❝The decline of 1.8 years in life expectancy was primarily due to increases in mortality from COVID-19 (61.2% of the negative contribution).
The decline in life expectancy would have been even greater if not for the offsetting effects of decreases in mortality due to cancer (43.1%)❞
Source: National Vital Statistics Reports
The US stats are applicable to Canada, the UK, and Australia: True or False?
False: it’s not quite so universal. Differences in healthcare systems will account for a lot, but there are other factors too:
- Life expectancy in Canada fell for the 3rd year in a row. What’s happening?
- UK life expectancy lagging behind rest of G7 except the US
- Australians are living longer but what does it take to reach 100 years old?
Here’s an interesting (UK-based) tool that calculates not just your life expectancy, but also gives the odds of living to various ages (e.g. this writer was given odds of living to 87, 96, 100).
Check yours here:
Office of National Statistics | Life Expectancy Calculator
To finish on a cheery note…
Data from Italian centenarians suggests a “mortality plateau”:
❝The risk of dying leveled off in people 105 and older, the team reports online today in Science.
That means a 106-year-old has the same probability of living to 107 as a 111-year-old does of living to 112.
Furthermore, when the researchers broke down the data by the subjects’ year of birth, they noticed that over time, more people appear to be reaching age 105.❞
Pop-sci source: Once you hit this age, aging appears to stop
Actual paper: The plateau of human mortality: demography of longevity pioneers
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Drug & Supplement Combo That Reverses Aging

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
So far, its effects have been dramatic (in a good way) in mice; human trials are now underway.
How does it work?
It builds from previous work, in which a Japanese research team created an “anti-aging vaccine”, that responded to a problem more specific than aging as a whole, namely atherosclerosis.
They found that a certain* protein was upregulated (i.e., it was made at a greater rate resulting in greater quantities) in patients (mouse and human alike) with atherosclerosis. So, they immunized the mice against that protein, and long story short, everything improved for them, from their atherosclerosis to general markers of aging—including growing back fur that had been lost due to age-related balding (just like in humans). They also lived longer, as is to be expected of a mouse who is now biologically younger.
*To avoid being mysterious: it was glycoprotein nonmetastatic melanoma protein B, known to its friends as GPNMB.
You may be wondering: how can one be immunized against a protein? If so, do bear in mind, a virus is also a protein. In this case, they developed an RNA vaccine, that works in a similar way to the COVID vaccines we all know and love (albeit with a different target).
You can read about this in abundant detail here: Senolytic vaccination improves normal and pathological age-related phenotypes and increases lifespan in progeroid mice
Hot on the heels of that, new approaches were found, including…
The combination
We’ll not keep you waiting; the combination is dasatinib plus quercetin, or else fisetin alone.
It’s about killing senescent (aging) “zombie cells” while sparing healthy cells, which that drug (dasatinib) and those supplements (quercetin and fisetin) do.
The researchers noted:
❝Senescent cells are resistant to apoptosis, which is governed through the upregulation of senescent cell anti-apoptotic pathways (SCAPs). Compounds were subsequently identified that disrupted the SCAPs, inducing death of senescent cells while leaving healthy cells unaffected. Forty-six potential senolytic agents were discovered through this process. To advance translational efforts, the majority of research has focused on agents with known safety profiles and limited off-target effects (Kirkland and Tchkonia, 2020).
The best characterized senolytic agents are dasatinib, a tyrosine kinase inhibitor approved for use in humans for cancer treatment, and quercetin, a naturally occurring plant flavonoid. The agents have a synergistic effect, making their combination more potent for senescent cell clearance (Zhu et al., 2015). As senescent cells do not divide and accumulate over a period of weeks, they can be administered using an intermittent approach, which further serves to reduce the risk of side effects (Kirkland and Tchkonia, 2020).
In preclinical trials, the combination of dasatinib and quercetin (D + Q) have been found to alleviate numerous chronic medical conditions including vascular stiffness, osteoporosis, frailty, and hepatic stenosis❞
Source: A geroscience motivated approach to treat Alzheimer’s disease: Senolytics move to clinical trials
As to how they expanded on this research:
❝In our study, oral D + Q were intermittently administered to tau transgenic mice with late-stage pathology (approximated to a 70-year-old human with advanced AD) (Musi et al., 2018). The treatment effectively reduced cellular senescence and associated senescence-associated secretory phenotype incidence. The 35 % reduction in neurofibrillary tangles was accompanied by enhanced neuron density, decreased ventricular enlargement, diminished tau accumulation, and restoration of aberrant cerebral blood flow. A subsequent preclinical study validated the findings, reporting that intermittently administered D + Q cleared senescent cells in the central nervous system, reduced amyloid-β plaques, attenuated neuroinflammation, and enhanced cognition❞
Source: Ibid.
And now taking it to humans:
❝The first clinical trial of D + Q for early-stage Alzheimer’s Disease (AD) has completed enrollment (Gonzales et al., 2021). The primary aim of the open-label pilot study was to examine the central nervous system penetrance of D and Q in a small sample of older adults with early-stage AD (NCT04063124). In addition, two placebo-controlled trials of D + Q for neurodegenerative disease are underway (NCT04685590 and NCT04785300).
One of the trials in development is a multi-site, double-blind, randomized, placebo-controlled study of senolytic therapy in older adults with amnestic mild cognitive impairment (MCI) or early-stage dementia (Clinical Dementia Rating Scale (CDR) Global 0.5–1) due to AD (elevated CSF total tau/Aβ42 ratio).
The treatment regimen will consist of 12-weeks of intermittently administered oral D + Q.❞
Source: Ibid.
The study is actually completed now, but its results are not yet published (again, at time of writing). Which means: they have the data, and now they’re writing the paper.
We look forward to providing an update about that, when the paper is published!
In the meantime…
Dasatinib is a drug usually prescribed to people with certain kinds of leukemia, and suffice it to say, it’s prescription-only. And unlike drugs that are often prescribed off-label (such as metformin for weight loss), getting your doctor to prescribe you an anticancer drug is unlikely unless you have the cancer in question.
You may be wondering: how is an anticancer drug helpful against aging? And the answer is that cancer and aging are very interrelated, and both have to do with “these old cells just won’t die, and are using the resources needed for young healthy cells”. So in both cases, killing those “zombie cells” while sparing healthy ones, is what’s needed. However, your doctor will probably not buy that as a reason to prescribe you a drug that is technically chemotherapy.
Quercetin, on the other hand, is a readily-available supplement, as is fisetin, and both have glowing (in a good way) safety profiles.
Want to know more?
You can read more about each of quercetin and fisetin (including how to get them), here:
Enjoy!
Share This Post
-

How To Plan For The Unplannable
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Always Follow Through
❝Two roads diverged in a wood, and I—
I took the one less traveled by,
And that has made all the difference:
Now my socks are wet.❞~ with apologies to Robert Frost
The thing is, much like a different Robert wrote, “The best-laid schemes o’ mice an’ men gang aft agley”, and when we have a plan and the unexpected occurs, we often find ourselves in a position of “well then, now what?”
This goes for New Year’s Resolutions that lasted until around January the 4th, and it goes for “xyz in a month” plans of diet, exercise, or so forth.
We’ve written before on bolstering flagging motivation when all is as expected but we just need an extra boost:
How To Keep On Keeping On… Long Term!
…but what about when the unexpected happens?
First rule: wear a belt and suspenders
Not literally, unless that’s your thing. But you might have heard this phrase from the business world, and it applies to healthful practices too:
If your primary plan fails, you need a second one already in place.
In business, we see this as “business continuity management”. For example, your writer here, I have backups for every important piece of tech I own, Internet connections from two different companies in case one goes down, and if there’s a power cut, I have everything accessible and sync’d on a fully-charged tablet so I can complete my work there if necessary. And yes, I have low-tech coffee-brewing equipment too.
In health, we should be as serious. We all learned back in 2020 that grocery stores and supply chains can fail; how do we eat healthily when all that is on sale is an assortment of random odds and ends? The answer, as we now know because hindsight really is 2020 in this case, is to keep a well-stocked pantry of healthy things with a long shelf life. Also a good stock of whatever supplements we take, and medicines, and water. And maintain them and rotate the stock!
And what of exercise? We must not rely on gyms, we can use and enjoy them sure, but we should have at least one good go-to routine for which we need nothing more than a bit of floorspace at home.
If you’re unsure where to start with that one, we strongly recommend this book that we reviewed recently:
Science of Pilates: Understand the Anatomy and Physiology to Perfect Your Practice – by Tracy Ward
Second rule: troubleshoot up front
With any given intended diet or exercise regime or other endeavor, we must ask ourselves: what could prevent me from doing this? Set a timer for at least 10 minutes, and write down as many things as possible. Then plan for those.
You can read a bit more about some of this here, the below article was written about facing depression and anxiety, but if you can enact your plans when unmotivated and fearful, then you will surely be able to enact them when not, so this information is good anyway:
When You Know What You “Should” Do (But Knowing Isn’t The Problem)
Third rule: don’t err the same way twice
We all screw up sometimes. To err is, indeed, human. So to errantly eat the wrong food, or do so at the wrong time, or miss a day’s exercise session etc, these things happen.
Just, don’t let it happen twice.
Once is an outlier; twice is starting to look like a pattern.
How To Break Out Of Cycles Of Self-Sabotage, And Stop Making The Same Mistakes
Enjoy!
Share This Post
-
5 Ways To Make Your Smoothie Blood Sugar Friendly (Avoid the Spike!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At 10almonds, we are often saying “eat whole fruit; don’t drink your calories”. Whole fruit is great for blood sugars; fruit juices and many smoothies on the other hand, not so much. Especially juices, being near-completely or perhaps even completely stripped of fiber, but even smoothies have had a lot of the fiber broken down and are still a liquid, meaning they are very quickly and easily digestible, and thus their sugars (whatever carbs are in there) can just zip straight into your veins.
However, there are ways to mitigate this…
Slow it down
The theme here is “give the digestive process something else to do”; some things are more quickly and easily digestible than others, and if it’s working on breaking down some of the slower things, it’s not waving sugars straight on through; they have to wait their turn.
To that end, recommendations include:
- Full-fat Greek yogurt which provides both protein and fat, helping to slow down the absorption of sugar. Always choose unsweetened versions to avoid added sugars, though!
- Coconut milk (canned) which is low in sugar and carbs, high in fat. This helps reduce blood sugar spikes, as she found through personal experimentation too.
- Avocado which is rich in healthy fats that help stabilize blood sugar. As a bonus, it blends well into smoothies without affecting the taste much.
- Coconut oil which contains medium-chain triglycerides (MCTs) that are quickly absorbed for energy without involving glucose, promoting fat-burning and reducing blood sugar spikes.
- Collagen powder which is a protein that helps lower blood sugar spikes while also supporting muscle growth, skin, and joints.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Share This Post


Related Posts
-
How To Actually Get Abs (10 Annoying Tips That Work!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Cori Lefkowitz, of “Strong At Any Age”, advises…
The method
It may not be fun, but here’s what she finds works:
- Be boring: stick to a simple, repetitive diet to track progress easily, and make hitting macros simpler.
- Cut back on protein bars: processed protein bars are calorie-dense but not filling (due to their small volume), so limit them, especially when trying to get lean.
- Stop daily fluctuations: she advises to be precise with macros and calories daily, not just weekly, to see consistent results.
- Focus on fiber: aim for 25–30g of fiber daily to improve gut health, reduce cravings, and maintain health while cutting fat.
- Get 30–40g of protein per meal: ensure each meal has enough protein to fuel muscle growth and support overall body function.
- Prioritize carbs around workouts: eat carbs before and after training to fuel performance, aid muscle repair, and maintain lean mass.
- Take diet breaks: incorporate 1–2 week maintenance phases to prevent metabolic adaptation, maintain muscle, and thus stay consistent in the long-term.
- Be careful with fat burners & preworkout: these can harm sleep, recovery, and long-term fat loss; opt for natural dietary energy sources instead.
- Don’t set-and-forget: regularly assess and adjust your diet and macros as your body and lifestyle change.
- “Suck it up, buttercup”: fat loss requires persistence, discipline, and pushing through tough moments when you feel like quitting.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Is A Visible Six-Pack Obtainable Regardless Of Genetic Predisposition?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

‘Tis To Season To Be SAD-Savvy
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Seasonal Affective Disorder & SAD Lamps
For those of us in the Northern Hemisphere, it’s that time of the year; especially after the clocks recently went back and the nights themselves are getting longer. So, what to do in the season of 3pm darkness?
First: the problem
The problem is twofold:
- Our circadian rhythm gets confused
- We don’t make enough serotonin
The latter is because serotonin production is largely regulated by sunlight.
People tend to focus on item 2, but item 1 is important too—both as problem, and as means of remedy.
Circadian rhythm is about more than just light
We did a main feature on this a little while back, talking about:
- What light/dark does for us, and how it’s important, but not completely necessary
- How our body knows what time it is even in perpetual darkness
- The many peaks and troughs of many physiological functions over the course of a day/night
- What that means for us in terms of such things as diet and exercise
- Practical take-aways from the above
Read: The Circadian Rhythm: Far More Than Most People Know
With that in mind, the same methodology can be applied as part of treating Seasonal Affective Disorder.
Serotonin is also about more than just light
Our brain is a) an unbelievably powerful organ, and the greatest of any animal on the planet b) a wobbly wet mass that gets easily confused.
In the case of serotonin, we can have problems:
- knowing when to synthesize it or not
- synthesizing it
- using it
- knowing when to scrub it or not
- scrubbing it
- etc
Selective Serotonin Re-uptake Inhibitors (SSRIs) are a class of antidepressants that, as the name suggests, inhibit the re-uptake (scrubbing) of serotonin. So, they won’t add more serotonin to your brain, but they’ll cause your brain to get more mileage out of the serotonin that’s there, using it for longer.
So, whether or not they help will depend on you and your brain:
Read: Antidepressants: Personalization Is Key!
How useful are artificial sunlight lamps?
Artificial sunlight lamps (also called SAD lamps), or blue light lamps, are used in an effort to “replace” daylight.
Does it work? According to the science, generally yes, though everyone would like more and better studies:
- The Efficacy of Light Therapy in the Treatment of Seasonal Affective Disorder: A Meta-Analysis of Randomized Controlled Trials
- Blue-Light Therapy for Seasonal and Non-Seasonal Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Interestingly, it does still work in cases of visual impairment and blindness:
How much artificial sunlight is needed?
According to Wirz-Justice and Terman (2022), the best parameters are:
- 10,000 lux
- full spectrum (white light)
- 30–60 minutes exposure
- in the morning
Source: Light Therapy: Why, What, for Whom, How, and When (And a Postscript about Darkness)
That one’s a fascinating read, by the way, if you have time.
Can you recommend one?
For your convenience, here’s an example product on Amazon that meets the above specifications, and is also very similar to the one this writer has
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Gut Renovation – by Dr. Roshini Raj, with Sheila Buff
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Unless we actually feel something going on down there, gut health is an oft-neglected part of overall health—which is unfortunate, because invisible as it may often be, it affects so much.
Gastroenterologist Dr. Roshini Raj gives us all the need-to-know information, explanations of why things happen the way they do with regard to the gut, and tips, tricks, and hacks to improve matters.
She also does some mythbusting along the way, and advises about what things don’t make a huge difference, including what medications don’t have a lot of evidence for their usefulness.
The style is easy-reading pop-science, with plenty of high-quality medical content.
Reading between the lines, a lot of the book as it stands was probably written by the co-author, Sheila Buff, who is a professional ghostwriter and specializes in working closely with doctors to produce works that are readable and informative to the layperson while still being full of the doctor’s knowledge and expertise. So a reasonable scenario is that Dr. Raj gave her extensive notes, she took it from there, passed it back to her for medical corrections, and they had a little back and forth until it was done. Whatever their setup, the end result was definitely good!
Bottom line: if you’d like a guide to gut health that’s practical and easy to read, while being quite comprehensive and certainly a lot more than “eat probiotics and fiber”, then this book is a fine choice.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: