

5 Ways To Make Your Smoothie Blood Sugar Friendly (Avoid the Spike!)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At 10almonds, we are often saying “eat whole fruit; don’t drink your calories”. Whole fruit is great for blood sugars; fruit juices and many smoothies on the other hand, not so much. Especially juices, being near-completely or perhaps even completely stripped of fiber, but even smoothies have had a lot of the fiber broken down and are still a liquid, meaning they are very quickly and easily digestible, and thus their sugars (whatever carbs are in there) can just zip straight into your veins.
However, there are ways to mitigate this…
Slow it down
The theme here is “give the digestive process something else to do”; some things are more quickly and easily digestible than others, and if it’s working on breaking down some of the slower things, it’s not waving sugars straight on through; they have to wait their turn.
To that end, recommendations include:
- Full-fat Greek yogurt which provides both protein and fat, helping to slow down the absorption of sugar. Always choose unsweetened versions to avoid added sugars, though!
- Coconut milk (canned) which is low in sugar and carbs, high in fat. This helps reduce blood sugar spikes, as she found through personal experimentation too.
- Avocado which is rich in healthy fats that help stabilize blood sugar. As a bonus, it blends well into smoothies without affecting the taste much.
- Coconut oil which contains medium-chain triglycerides (MCTs) that are quickly absorbed for energy without involving glucose, promoting fat-burning and reducing blood sugar spikes.
- Collagen powder which is a protein that helps lower blood sugar spikes while also supporting muscle growth, skin, and joints.
For more on all of these, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.

Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
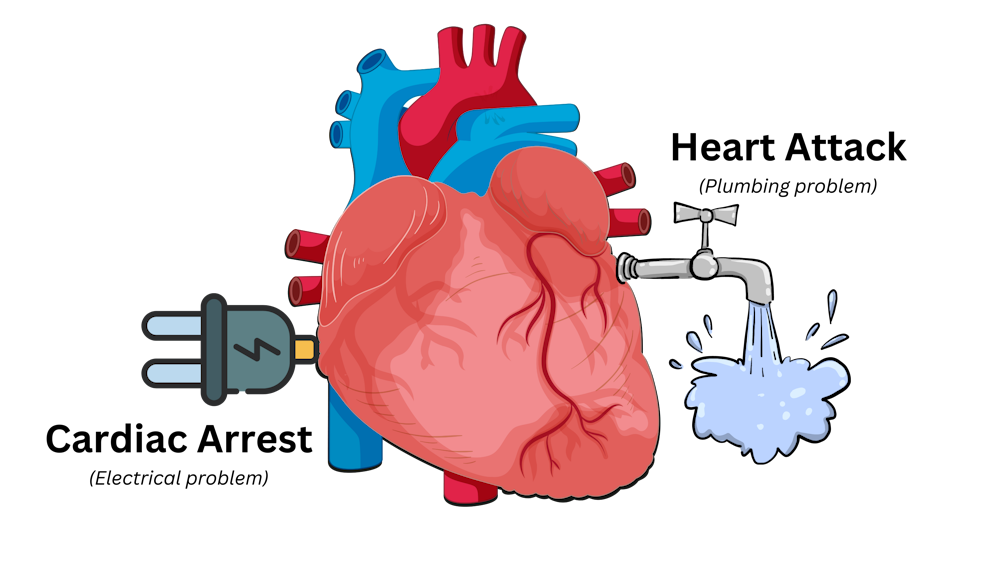
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Going for a bushwalk? 3 handy foods to have in your backpack (including muesli bars)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This time of year, many of us love to get out and spend time in nature. This may include hiking through Australia’s many beautiful national parks.
Walking in nature is a wonderful activity, supporting both physical and mental health. But there can be risks and it’s important to be prepared.
You may have read the news about hiker, Hadi Nazari, who was recently found alive after spending 13 days lost in Kosciuszko National Park.
He reportedly survived for almost two weeks in the Snowy Mountains region of New South Wales by drinking fresh water from creeks, and eating foraged berries and two muesli bars.
So next time you’re heading out for a day of hiking, what foods should you pack?
Here are my three top foods to carry on a bushwalk that are dense in nutrients and energy, lightweight and available from the local grocery store.
Leah-Anne Thompson/Shutterstock 1. Muesli bars
Nazari reportedly ate two muesli bars he found in a mountain hut. Whoever left the muesli bars there made a great choice.
Muesli bars come individually wrapped, which helps them last longer and makes them easy to transport.
They are also a good source of energy. Muesli bars typically contain about 1,500–1,900 kilojoules per 100 grams. The average energy content for a 35g bar is about 614kJ.
This may be a fraction of what you’d usually need in a day. However, the energy from muesli bars is released at a slow to moderate pace, which will help keep you going for longer.
Muesli bars are also packed with nutrients. They contain all three macronutrients (carbohydrate, protein and fat) that our body needs to function. They’re a good source of carbohydrates, in particular, which are a key energy source. An average Australian muesli bar contains 14g of whole grains, which provide carbohydrates and dietary fibre for long-lasting energy.
Muesli bars that contain nuts are typically higher in fat (19.9g per 100g) and protein (9.4g per 100g) than those without.
Fat and protein are helpful for slowing down the release of energy from foods and the protein will help keep you feeling full for longer.
There are many different types of muesli bars to choose from. I recommend looking for those with whole grains, higher dietary fibre and higher protein content.
2. Nuts
Nuts are nature’s savoury snack and are also a great source of energy. Cashews, pistachios and peanuts contain about 2,300-2,400kJ per 100g while Brazil nuts, pecans and macadamias contain about 2,700-3,000kJ per 100g. So a 30g serving of nuts will provide about 700-900kJ depending on the type of nut.
Just like muesli bars, the energy from nuts is released slowly. So even a relatively small quantity will keep you powering on.
Nuts are also full of nutrients, such as protein, fat and fibre, which will help to stave off hunger and keep you moving for longer.
When choosing which nuts to pack, almost any type of nut is going to be great.
Peanuts are often the best value for money, or go for something like walnuts that are high in omega-3 fatty acids, or a nut mix.
Whichever nut you choose, go for the unsalted natural or roasted varieties. Salted nuts will make you thirsty.
Nut bars are also a great option and have the added benefit of coming in pre-packed serves (although nuts can also be easily packed into re-usable containers).
If you’re allergic to nuts, roasted chickpeas are another option. Just try to avoid those with added salt.
Nuts are nature’s savoury snack and are also a great source of energy. Eakrat/Shutterstock 3. Dried fruit
If nuts are nature’s savoury snack, fruit is nature’s candy. Fresh fruits (such as grapes, frozen in advance) are wonderfully refreshing and perfect as an everyday snack, although can add a bit of weight to your hiking pack.
So if you’re looking to reduce the weight you’re carrying, go for dried fruit. It’s lighter and will withstand various conditions better than fresh fruit, so is less likely to spoil or bruise on the journey.
There are lots of varieties of dried fruits, such as sultanas, dried mango, dried apricots and dried apple slices.
These are good sources of sugar for energy, fibre for fullness and healthy digestion, and contain lots of vitamins and minerals. So choose one (or a combination) that works for you.
Don’t forget water
Next time you head out hiking for the day, you’re all set with these easily available, lightweight, energy- and nutrient-dense snacks.
This is not the time to be overly concerned about limiting your sugar or fat intake. Hiking, particularly in rough terrain, places demands on your body and energy needs. For instance, an adult hiking in rough terrain can burn upwards of about 2,000kJ per hour.
And of course, don’t forget to take plenty of water.
Having access to even limited food, and plenty of fresh water, will not only make your hike more pleasurable, it can save your life.
Margaret Murray, Senior Lecturer, Nutrition, Swinburne University of Technology
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Fix Your Squat: 3 Squat Myths That Need To Die
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This also explains why these myths appeared in the first place:
Let’s get down to it
Trying to copy one “perfect” squat form for every body type can cause more harm than good (people have different builds, postures, mobility, and injury histories).
The result is often people giving wrong advice, much like an albatross might say to a penguin “flight is easy, just flap your wings like this”, or a penguin might say to an albatross “it’s perfectly safe to swim under this ice, just your breath for 15 minutes”.
Consequently, good form should focus on engaging the right muscles and moving safely, not just mimicking how a squat looks on someone else.
Furthermore, forcing a “textbook” squat that’s not right for you can make your body seek mobility from the wrong joints or overuse small stabilizing muscles, increasing compensation injury risk.
In particular, three myths are very prevalent:
- “Your knees mustn’t go past your toes”: this cue originated to help people sit back instead of bending only at the knees, but knees can and often should go past toes, for example when doing a deep and/or pistol squat. The real key is to keep your heels down and properly load your glutes while maintaining good hip and ankle mobility.
- “You must stay perfectly upright”: forcing a straight torso if your build or mobility doesn’t allow for it can cause back pain. A forward lean can be perfectly fine—especially for people with long femurs or shorter torsos—as long as your glutes and core are working properly.
- “There’s one correct squat depth”: there’s no universal rule about how low to go—it depends on your structure, injury history, and control. aim to move through the largest range of motion you can safely manage. Both deep and parallel squats have value depending on your goals. Also, even those who can squat deep can still benefit from using partial squats to target weak points, while others may stop at parallel to protect their knees or maintain control.
For more on each of these plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Squat Variations for Painful Knees (No More Pain!)
Take care!
Share This Post






-
Lupus Sex Differences Are Not What You Might Think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

This is Dr. Seyhan Yazar, a medical scientist and Research Fellow, whose lab (the Yazar Lab) “focuses on uncovering the complex interplay between genetic susceptibility and environmental triggers in autoimmune diseases”, of which, lupus is one.
So, what does she want us to know?
Sex? It’s not about the X
First, a recap on how lupus works: lupus is an autoimmune disease where the immune system attacks its own tissues, causing inflammation and organ damage (to oversimplify it in very few words).
Next, how lupus is currently treated: mostly with immunosuppressant drugs, which reduce symptoms but have significant side effects, not least of all the fact that your immune system will be suppressed, leaving you vulnerable to infections, cancer, aging, and the like. So, there’s really a “damned if you do, damned if you don’t” aspect here (because untreated lupus will run your immune system into the ground with its chronic inflammation, which will also leave you vulnerable to the aforementioned things).
See also: How to Prevent (or Reduce) Inflammation
Finally, onto the new science from Dr. Yazar: while it’s well-known that lupus disproportionately affects women (with women’s lupus risk being 9x that of men’s, all other things being equal), it hasn’t been known entirely what’s going on with that and how, but Dr. Yazar’s work shines new light on this!
She and her team analyzed over a million (for the curious: 1,267,758) individual immune cells from 982 healthy people, to identify sex-specific genetic switches that shape male and female immune systems differently.
In the immune cell analysis, women had higher levels of B cells and regulatory T cells, with immune activity more strongly biased towards inflammatory pathways, creating a more vigilant immune system that will often better fight infections, but at a cost: it also raises the risk of “friendly fire” against healthy tissues, and that’s what happens in the case of lupus.
On the flipside, men had more monocytes and immune activity focused more on cellular maintenance rather than inflammation, which will tend to reduce autoimmune risk but at its own cost: it raises the risk (and severity) of infections and some cancers.
Notably, these results showed that the sex-specific immune differences aren’t driven by X or Y chromosomes as often assumed, but instead by autosomes—the non-sex chromosomes shared by all sexes.
This is very consistent with what we know of many sex-related disease risk factors being hormonally mediated, rather than mediated by genes.
You can read Dr. Yazar’s paper on all of this, here: The impact of sex on the immune system explored at the single-cell level
As for what can be done about this, the same principle applies as we talked about in Alzheimer’s Sex Differences May Not Be What They Appear but the opposite way around, meaning the solution may be the same as what we talked about in The Hormone Therapy That Reduces Breast Cancer Risk & More.
But! That last part is not yet proven, and is rather more simply a promising avenue for the next leg of the research, so please don’t take that as medical advice.
Want to learn more?
For a much more in-depth treatment of lupus management, you might like this excellent book we reviewed a while back:
The “et al.” in question? Jemima Albayda, MD; Divya Angra, MD; Alan N. Baer, MD; Sasha Bernatsky, MD, PhD; George Bertsias, MD, PhD; Ashira D. Blazer, MD; Ian Bruce, MD; Jill Buyon, MD; Yashaar Chaichian, MD; Maria Chou, MD; Sharon Christie, Esq; Angelique N. Collamer, MD; Ashté Collins, MD; Caitlin O. Cruz, MD; Mark M. Cruz, MD; Dana DiRenzo, MD; Jess D. Edison, MD; Titilola Falasinnu, PhD; Andrea Fava, MD; Cheri Frey, MD; Neda F. Gould, PhD; Nishant Gupta, MD; Sarthak Gupta, MD; Sarfaraz Hasni, MD; David Hunt, MD; Mariana J. Kaplan, MD; Alfred Kim, MD; Deborah Lyu Kim, DO; Rukmini Konatalapalli, MD; Fotios Koumpouras, MD; Vasileios C. Kyttaris, MD; Jerik Leung, MPH; Hector A. Medina, MD; Timothy Niewold, MD; Julie Nusbaum, MD; Ginette Okoye, MD; Sarah L. Patterson, MD; Ziv Paz, MD; Darryn Potosky, MD; Rachel C. Robbins, MD; Neha S. Shah, MD; Matthew A. Sherman, MD; Yevgeniy Sheyn, MD; Julia F. Simard, ScD; Jonathan Solomon, MD; Rodger Stitt, MD; George Stojan, MD; Sangeeta Sule, MD; Barbara Taylor, CPPM, CRHC; George Tsokos, MD; Ian Ward, MD; Emma Weeding, MD; Arthur Weinstein, MD; Sean A. Whelton, MD
The reason we mention this is to render it clear that this isn’t one man’s opinions (as happens with many books about certain topics), but rather, a panel of that many doctors all agreeing that this is correct and good, evidence-based, up-to-date (as of the publication of this latest revised edition all so recently) information.
Want to learn less?
If the aforementioned 848-page opus seems a little too overwhelming, then you might prefer:
The Lupus Solution – by Dr. Tiffany Caplan & Dr. Brent Caplan ← a much slimmer tome; just 182 pages 🙂
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Sweet Potato vs Turnip – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sweet potato to turnip, we picked the sweet potato.
Why?
It wasn’t close:
In terms of macros, sweet potato has more fiber, carbs, and protein, making it the more nutrient-dense option in this category.
In the category of vitamins, sweet potato has a lot more of vitamins A, B1, B2, B3, B5, B6, C, E, and K, while turnips have a little more vitamin B9, yielding a very convincing 9:1 victory to sweet potato here.
Looking at minerals next, sweet potatoes have more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and zinc, while turnips are not higher in any minerals. Another easy win for sweet potatoes!
Adding up the sections makes for a clear overall win for sweet potato, but by all means do enjoy either or both, as diversity is best, and watch how you cook them!
In this comparison, we used data from them both being steamed skin-on, in the interests of fairness, so there’s a difference between that and if you decided to make sweet potato fries or somesuch 😉
Want to learn more?
You might like:
Carb-Strong or Carb-Wrong? Should You Go Light Or Heavy On Carbs?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Is cancer more common in women after IVF?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Since fertility treatments such as in vitro fertilisation (IVF) began, there has been concern they could cause cancer.
Concerns have included whether aspects of treatment – such as taking hormonal medications, or puncturing the ovaries to retrieve eggs – could stimulate the growth of cancer cells.
Now, our new study, published on Wednesday, has found women who underwent fertility treatments had a comparable overall rate of cancer to similarly aged women.
However, there were some differences: they had more uterine, ovarian, and melanoma cancers, and fewer lung and cervical cancers. Let’s take a look at what this means.
Shaw Photography Co./Getty What we did
Our study wanted to find out whether women who underwent fertility treatments had a different rate of cancer from the general population.
We used individual records from Medicare and the Pharmaceutical Benefits Scheme to find women who had fertility treatments between 1991 and 2018. We linked this data to the Australian Cancer Database to find cancer diagnoses.
We found 417,984 women who received fertility treatments and followed them for about a decade on average:
- 274,676 women had treatments where the egg was removed from the women’s body (IVF and similar treatments)
- 120,739 women had treatments with a specialist where the egg was not removed (mainly intrauterine insemination)
- 175,510 women received a prescription for clomiphene citrate (also known as Clomid), a medication that induces ovulation.
One woman could have had multiple types of treatment.
Their median age (the midpoint of their ages) was 32–34 years. Compared to the general population, fewer lived in disadvantaged areas.
We compared these women’s rates of cancers to women in the general population, by statistically matching them on factors such as age and the state they lived in.
What we found
Women who received fertility treatments, either with or without egg removal, had close to the exact total number of cancers we would expect in the general population of women.
But women who used clomiphene citrate had 1.04 times the rate of cancer, or 8.6 extra cancers for every 100,000 women treated each year.
Rates of uterine cancer, ovarian cancer (except for those who used clomiphene citrate), and melanoma were 1.07–1.83 times higher, depending on treatment type. This means about three to seven more of these cancers for every 100,000 women treated each year.
This difference could be due to risk factors unrelated to the treatment. For example, endometriosis – a risk factor for infertility – is linked to ovarian cancer. Similarly, more Caucasian women receive fertility treatments, and fair skin is an established risk factor for melanoma.
Across all treatments rates of cervical cancer and lung cancer were 1.43–1.92 times lower. This translates to around two to six fewer cancers for every 100,000 treated women each year.
These decreases could be due to women receiving fertility treatment being less likely to smoke. Women who receive fertility treatment may also be more likely to be screened for cervical cancer, as clinicians often encourage them to get screened before treatment. But this is anecdotal – we don’t yet have data on this.
What this means
Overall, these findings are reassuring for women who have received or are planning fertility treatments.
The number of people undergoing fertility treatments is increasing worldwide. These findings deepen our understanding of the types of cancers diagnosed in women who receive fertility treatment.
Our study shows some cancers are more common in women who received fertility treatments than in the general population of women.
However, the absolute numbers of these cancers are small, similar to those observed for women using some other medical interventions (including the contraceptive pill).
It is normal to see differences in cancer risk in specific populations when compared to the general population.
So, does this mean IVF does not cause cancer?
This study design cannot determine if fertility treatments themselves cause or prevent cancer.
Though fertility treatments may contribute to cancer risk, women who receive fertility treatments have a different health and socio-demographic profile to the general population of women. These factors may affect cancer risk.
We did not have any data on why women were using fertility treatments to get pregnant and whether this is connected to their cancer risk. For example, we don’t know if they were receiving treatment for medical infertility, or for another reason (such as same-sex couples trying to conceive).
Our study also only followed women for around ten years, and the cancer risk profile may change as these women age.
The takeaway
As with every medical treatment, it is important for women and their health-care practitioners to make informed decisions before and after fertility treatment, including considering potential changes in cancer risk.
Women considering fertility treatment, and those who’ve used fertility treatment, should continue to participate in the routine cancer screening programs they’re eligible for.
If women are worried about their risk of cancer, they should consult their doctor to understand the steps they can take to reduce their risk.
Adrian Raymond Walker, Research Fellow, Centre for Big Data Research in Health, UNSW Sydney and Claire Vajdic, Professor, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:




