Immunity – by Dr. William Paul
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This book gives a very person-centric (i.e., focuses on the contributions of named individuals) overview of advances in the field of immunology—up to its publication date in 2015. So, it’s not cutting edge, but it is very good at laying the groundwork for understanding more recent advances that occur as time goes by. After all, immunology is a field that never stands still.
We get a good grounding in how our immune system works (and how it doesn’t), the constant arms race between pathogens and immune responses, and the complexities of autoimmune disorders and—which is functionally in an overlapping category of disease—cancer. And, what advances we can expect soon to address those things.
Given the book was published 8 years ago, how did it measure up? Did we get those advances? Well, for the mostpart yes, we have! Some are still works in progress. But, we’ve also had obvious extra immunological threats in years since, which have also resulted in other advances along the way!
If the book has a downside, it’s that sometimes the author can be a little too person-centric. It’s engaging to focus on human characters, and helps us bring information to life; name-dropping to excess, along with awards won, can sometimes feel a little like the book was co-authored by Tahani Al-Jamil.
Nevertheless, it certainly does keep the book from getting too dry!
Bottom line: this book is a great overview of immunology and immunological research, for anyone who wants to understand these things better.
Click here to check out Immunity, and boost your knowledge of yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

5 Follow-Along Exercises To Rapidly Improve Your Eyesight

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Try it for yourself:
The Eyes Still Have It
It’s best if you follow along in the video, but in case you prefer to know what to expect, the 5 exercises are:
- Blink for a minute: blinking relaxes your eyes by lubricating, cleaning, and shielding them from light. Lack of frequent blinking can cause dryness, inflammation, and blurred vision. Open and close your eyelids quickly but gently for 30–60 seconds—ideal for anyone focusing on screens or detailed work.
- Close your eyes: darkness helps rest and strengthen the photoreceptor cells in your eyes. Sit back, close your eyes fully, and relax your eyelids for about 30 seconds. Think about something pleasant to help your eye muscles unwind. It’s as easy as that!
- Move your gaze in different directions: improves overall visual perception and benefits both nearsighted and farsighted vision. Look right to left for 5 seconds, then up and down for 5 seconds. Next, move your eyes in slow circular motions for 10–15 seconds, and finish by tracing a figure eight with your gaze.
- Draw geometric figures with your gaze: with your eyes open, trace simple shapes—e.g. triangles, rectangles, squares, and circles—then progress to more complex figures. This improves eye coordination and range of movement.
- Move your eyeballs up and down: close your eyes and slowly move your eyeballs up and down about 5–10 times. Keep the movement gentle and deliberate to relax your eye muscles.
If you’d like to be talked through it, then enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Vision for Life, Revised Edition – by Dr. Meir Schneider
Take care!
Share This Post
-

The Cold Truth About Respiratory Infections
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Pathogens That Came In From The Cold

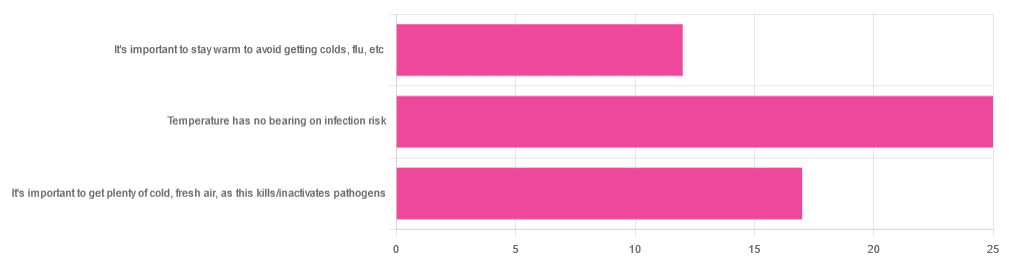
Yesterday, we asked you about your climate-themed policy for avoiding respiratory infections, and got the above-depicted, below-described, set of answers:
- About 46% of respondents said “Temperature has no bearing on infection risk”
- About 31% of respondents said “It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens”
- About 22% of respondents said “It’s important to stay warm to avoid getting colds, flu, etc”
Some gave rationales, including…
For “stay warm”:
❝Childhood lessons❞
For “get cold, fresh air”:
❝I just feel that it’s healthy to get fresh air daily. Whether it kills germs, I don’t know❞
For “temperature has no bearing”:
❝If climate issue affected respiratory infections, would people in the tropics suffer more than those in colder climates? Pollutants may affect respiratory infections, but I doubt just temperature would do so.❞
So, what does the science say?
It’s important to stay warm to avoid getting colds, flu, etc: True or False?
False, simply. Cold weather does increase the infection risk, but for reasons that a hat and scarf won’t protect you from. More on this later, but for now, let’s lay to rest the idea that bodily chilling will promote infection by cold, flu, etc.
In a small-ish but statistically significant study (n=180), it was found that…
❝There was no evidence that chilling caused any acute change in symptom scores❞
Read more: Acute cooling of the feet and the onset of common cold symptoms
Note: they do mention in their conclusion that chilling the feet “causes the onset of cold symptoms in about 10% of subjects who are chilled”, but the data does not support that conclusion, and the only clear indicator is that people who are more prone to colds generally, were more prone to getting a cold after a cold water footbath.
In other words, people who were more prone to colds remained more prone to colds, just the same.
It’s important to get plenty of cold, fresh air, as this kills/inactivates pathogens: True or False?
Broadly False, though most pathogens do have an optimal operating temperature that (for obvious reasons) is around normal human body temperature.
However, given that they don’t generally have to survive outside of a host body for long to get passed on, the fact that the pathogens may be a little sluggish in the great outdoors will not change the fact that they will be delighted by the climate in your respiratory tract as soon as you get back into the warm.
With regard to the cold air not being a reliable killer/inactivator of pathogens, we call to the witness stand…
Polar Bear Dies From Bird Flu As H5N1 Spreads Across Globe
(it was found near Utqiagvik, one of the northernmost communities in Alaska)
Because pathogens like human body temperature, raising the body temperature is a way to kill/inactivate them: True or False?
True! Unfortunately, it’s also a way to kill us. Because we, too, cannot survive for long above our normal body temperature.
So, for example, bundling up warmly and cranking up the heating won’t necessarily help, because:
- if the temperature is comfortable for you, it’s comfortable for the pathogen
- if the temperature is dangerous to the pathogen, it’s dangerous to you too
This is why the fever response evolved, and/but why many people with fevers die anyway. It’s the body’s way of playing chicken with the pathogen, challenging “guess which of us can survive this for longer!”
Temperature has no bearing on infection risk: True or False?
True and/or False, circumstantially. This one’s a little complex, but let’s break it down to the essentials.
- Temperature has no direct effect, for the reasons we outlined above
- Temperature is often related to humidity, which does have an effect
- Temperature does tend to influence human behavior (more time spent in open spaces with good ventilation vs more time spent in closed quarters with poor ventilation and/or recycled air), which has an obvious effect on transmission rates
The first one we covered, and the third one is self-evident, so let’s look at the second one:
Temperature is often related to humidity, which does have an effect
When the environmental temperature is warmer, water droplets in the air will tend to be bigger, and thus drop to the ground much more quickly.
When the environmental temperature is colder, water droplets in the air will tend to be smaller, and thus stay in the air for longer (along with any pathogens those water droplets may be carrying).
Some papers on the impact of this:
- Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections
- A Decrease in Temperature and Humidity Precedes Human Rhinovirus Infections in a Cold Climate
So whatever temperature you like to keep your environment, humidity is a protective factor against respiratory infections, and dry air is a risk factor.
So, for example:
- If the weather doesn’t suit having good ventilation, a humidifier is a good option
- Being in an airplane is one of the worst places to be for this, outside of a hospital
Don’t have a humidifier? Here’s an example product on Amazon, but by all means shop around.
A crock pot with hot water in and the lid off is also a very workable workaround too
Take care!
Share This Post
-

Move – by Caroline Williams
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
- Get 150 minutes of moderate exercise per week, says the American Heart Association
- There are over 10,000 minutes per week, says the pocket calculator
Is 150/10,000 really the goal here? Really?
For Caroline Williams, the answer is no.
In this book that’s practically a manifesto, she outlines the case that:
- Humans evolved to move
- Industrialization and capitalism scuppered that
- We now spend far too long each day without movement
Furthermore, for Williams this isn’t just an anthropological observation, it’s a problem to be solved, because:
- Our lack of movement is crippling us—literally
- Our stagnation affects not just our bodies, but also our minds
- (again literally—there’s a direct correlation with mental health)
- We urgently need to fix this
So, what now, do we need to move in to the gym and become full-time athletes to clock up enough hours of movement? No.
Williams convincingly argues the case (using data from supercentenarian “blue zones” around the world) that even non-exertive movement is sufficient. In other words, you don’t have to be running; walking is great. You don’t have to be lifting weights; doing the housework or gardening will suffice.
From that foundational axiom, she calls on us to find ways to build our life around movement… rather than production-efficiency and/or convenience. She gives plenty of tips for such too!
Bottom line: some books are “I couldn’t put it down!” books. This one’s more of a “I got the urge to get up and get moving!” book.
Get your get-up-and-go up and going with “Move”—order yours from Amazon today!
Share This Post

Related Posts
-

Living a Healthy Life with Chronic Conditions – by Dr. Kate Lorig et al.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The “et al.” here is a collection of other medical professionals, and indeed the first edition of this book was based on a 5-year study they did. Since then, it’s grown as a collaborative endeavour between the listed authors and colleagues in their field who didn’t make the author list on the front cover, but did contribute research, feedback, additions, etc. This has been so comprehensive that one could argue that in essence, this whole book itself has been as-though peer-reviewed by the extent of the professional collaboration.
The authors make the case that while a lot of people are in the happy position of considering “chronic conditions” to be something suffered by other people, most of us—even most of the healthiest of us—will acquire at least one in our lifetime.
You may be wondering how the book addresses the incredible heterogeneity of chronic conditions; surely there is no one-size-fits-all advice for sufferers of things as diverse as diabetes and lupus and long COVID and osteoporosis and depression.
And the answer is that while there are sections for condition-specific advice, a lot of the book takes a “different conditions, similar symptoms” approach that notes that, in fact, self-managing these symptoms typically is an endeavor in which we find more commonalities than differences.
Nor is it your average industry professional book of “get some exercise, eat more plants, do some meditation”. Because yes, those things are good (and the book does cover them too), but that’s a little basic and is more a fair topic for a leaflet than a 418*-page tome. Instead, this book goes far beyond that, covering everything from self-advocacy in healthcare settings, to sex positions (in fact there is a whole chapter about sex and intimacy, including dealing with symptoms that occur during sex, and other ways that chronic conditions can change sex, and what can be done about that in practical terms).
*The Amazon listing currently says 344 pages, but this reviewer is distinctly looking at page 418 here, so perhaps the 344-page count got copied and pasted from a listing of an older edition.
There are also whole chapters about managing medications actively (i.e. not just doing whatever you are told without question, but actually being able to understand and make more decisions for yourself), pain management of course, the broad topic of safety and freedom (reducing the limits placed on one’s life and what one can do, where one can go, etc, and doing so safely) and so much more.
The style is highly-polished high-quality science education. It’s neither dumbed-down pop-science nor inaccessible academia. It’s clear and easy to read, and incredibly informative.
Bottom line: if you or a loved one has a chronic health condition, we recommend getting a copy of this.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Foot Drop!
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Interesting about DVT after surgery. A friend recently got diagnosed with foot drop. Could you explain that? Thank you.❞
First, for reference, the article about DVT after surgery was:
DVT Risk Management Beyond The Socks
As for foot drop…
Foot drop is descriptive of the main symptom: the inability to raise the front part of the foot due to localized weakness/paralysis. Hence, if a person with foot drop dangles their feet over the edge of the bed, for example, the affected foot will simply flop down, while the other (if unaffected) can remain in place under its own power. The condition is usually neurological in origin, though there are various more specific causes:
When walking unassisted, this will typically result in a distinctive “steppage gait”, as it’s necessary to lift the foot higher to compensate, or else the toes will scuff along the ground.
There are mobility aids that can return one’s walking to more or less normal, like this example product on Amazon.
Incidentally, the above product will slightly shorten the lifespan of shoes, as it will necessarily pull a little at the front.
There are alternatives that won’t like this example product on Amazon, but this comes with the different problem that it limits the user to stepping flat-footedly, which is not only also not an ideal gait, but also, will serve to allow any muscles down there that were still (partially or fully) functional to atrophy. For this reason, we’d recommend the first product we mentioned over the second one, unless your personal physiotherapist or similar advises otherwise (because they know your situation and we don’t).
Both have their merits, though:
Trends and Technologies in Rehabilitation of Foot Drop: A Systematic Review
Of course, prevention is better than cure, so while some things are unavoidable (especially when it comes to neurological conditions), we can all look after our nerve health as well as possible along the way:
Peripheral Neuropathy: How To Avoid It, Manage It, Treat It
…as well as the very useful:
What Does Lion’s Mane Actually Do, Anyway?
…which this writer personally takes daily and swears by (went from frequent pins-and-needles to no symptoms and have stayed that way, and that’s after many injuries over the years).
If you’d like a more general and less supplements-based approach though, check out:
Steps For Keeping Your Feet A Healthy Foundation
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Top 8 Fruits That Prevent & Kill Cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Amy Dee, pharmacist and cancer survivor herself, lays out the best options for anticancer fruits:
The fruits
Without further ado, they are:
- Kiwi: promotes cancer cell death while sparing healthy cells
- Plums & peaches: an interesting choice to list these similar fruits together as one item, but they both also induce cell death in cancer cells while sparing healthy ones
- Dragon fruit: this does the same, while also inhibiting cancer cell growth
- Figs: these have antitumor effects specifically, while removing carcinogens too, and additionally sensitizing cancer cells to light therapy
- Cranberries: disrupt cancer cell adhesion, breaking down tumors, while protecting non-cancerous cells against DNA damage
- Citrus fruits: inhibit tumor growth and kill cancer cells; regular consumption is also associated with a lower cancer risk (be warned though, grapefruit interacts with some medications)
- Cherries: induce cancer cell death; protect healthy cells against DNA damage
- Tomatoes: don’t often make it into lists of fruits, but lycopene reduces cancer risk, and slows the growth of cancer cells (10almonds note: watermelon has more lycopene than tomatoes, and is more traditionally considered a fruit in all respects, so could have taken the spot here).
We would also argue that apricots could have had a spot on the list, both for their lycopene content (comparable to tomatoes) and their botanical (and thus phytochemical) similarities to peaches and plums.
For more information on each of these (she also talks about the different polyphenols and other nutrients that constitute the active compounds delivering these anticancer effects), enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
- Food Choice & Cancer Risk: Eat To Beat Cancer
- Beat Cancer Kitchen: Deliciously Simple Plant-Based Anticancer Recipes (book)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: