How much weight do you actually need to lose? It might be a lot less than you think
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’re one of the one in three Australians whose New Year’s resolution involved losing weight, it’s likely you’re now contemplating what weight-loss goal you should actually be working towards.
But type “setting a weight loss goal” into any online search engine and you’ll likely be left with more questions than answers.
Sure, the many weight-loss apps and calculators available will make setting this goal seem easy. They’ll typically use a body mass index (BMI) calculator to confirm a “healthy” weight and provide a goal weight based on this range.
Your screen will fill with trim-looking influencers touting diets that will help you drop ten kilos in a month, or ads for diets, pills and exercise regimens promising to help you effortlessly and rapidly lose weight.
Most sales pitches will suggest you need to lose substantial amounts of weight to be healthy – making weight loss seem an impossible task. But the research shows you don’t need to lose a lot of weight to achieve health benefits.
Using BMI to define our target weight is flawed
We’re a society fixated on numbers. So it’s no surprise we use measurements and equations to score our weight. The most popular is BMI, a measure of our body weight-to-height ratio.
BMI classifies bodies as underweight, normal (healthy) weight, overweight or obese and can be a useful tool for weight and health screening.
But it shouldn’t be used as the single measure of what it means to be a healthy weight when we set our weight-loss goals. This is because it:
- fails to consider two critical factors related to body weight and health – body fat percentage and distribution
- does not account for significant differences in body composition based on gender, ethnicity and age.
How does losing weight benefit our health?
Losing just 5–10% of our body weight – between 6 and 12kg for someone weighing 120kg – can significantly improve our health in four key ways.
1. Reducing cholesterol
Obesity increases the chances of having too much low-density lipoprotein (LDL) cholesterol – also known as bad cholesterol – because carrying excess weight changes how our bodies produce and manage lipoproteins and triglycerides, another fat molecule we use for energy.
Having too much bad cholesterol and high triglyceride levels is not good, narrowing our arteries and limiting blood flow, which increases the risk of heart disease, heart attack and stroke.
But research shows improvements in total cholesterol, LDL cholesterol and triglyceride levels are evident with just 5% weight loss.
2. Lowering blood pressure
Our blood pressure is considered high if it reads more than 140/90 on at least two occasions.
Excess weight is linked to high blood pressure in several ways, including changing how our sympathetic nervous system, blood vessels and hormones regulate our blood pressure.
Essentially, high blood pressure makes our heart and blood vessels work harder and less efficiently, damaging our arteries over time and increasing our risk of heart disease, heart attack and stroke.

Prostock-studio/Shutterstock
Like the improvements in cholesterol, a 5% weight loss improves both systolic blood pressure (the first number in the reading) and diastolic blood pressure (the second number).
A meta-analysis of 25 trials on the influence of weight reduction on blood pressure also found every kilo of weight loss improved blood pressure by one point.
3. Reducing risk for type 2 diabetes
Excess body weight is the primary manageable risk factor for type 2 diabetes, particularly for people carrying a lot of visceral fat around the abdomen (belly fat).
Carrying this excess weight can cause fat cells to release pro-inflammatory chemicals that disrupt how our bodies regulate and use the insulin produced by our pancreas, leading to high blood sugar levels.
Type 2 diabetes can lead to serious medical conditions if it’s not carefully managed, including damaging our heart, blood vessels, major organs, eyes and nervous system.
Research shows just 7% weight loss reduces risk of developing type 2 diabetes by 58%.
4. Reducing joint pain and the risk of osteoarthritis
Carrying excess weight can cause our joints to become inflamed and damaged, making us more prone to osteoarthritis.
Observational studies show being overweight doubles a person’s risk of developing osteoarthritis, while obesity increases the risk fourfold.
Small amounts of weight loss alleviate this stress on our joints. In one study each kilogram of weight loss resulted in a fourfold decrease in the load exerted on the knee in each step taken during daily activities.

Shutterstock/Rostislav_Sedlacek
Focus on long-term habits
If you’ve ever tried to lose weight but found the kilos return almost as quickly as they left, you’re not alone.
An analysis of 29 long-term weight-loss studies found participants regained more than half of the weight lost within two years. Within five years, they regained more than 80%.
When we lose weight, we take our body out of its comfort zone and trigger its survival response. It then counteracts weight loss, triggering several physiological responses to defend our body weight and “survive” starvation.
Just as the problem is evolutionary, the solution is evolutionary too. Successfully losing weight long-term comes down to:
losing weight in small manageable chunks you can sustain, specifically periods of weight loss, followed by periods of weight maintenance, and so on, until you achieve your goal weight
making gradual changes to your lifestyle to ensure you form habits that last a lifetime.
Setting a goal to reach a healthy weight can feel daunting. But it doesn’t have to be a pre-defined weight according to a “healthy” BMI range. Losing 5–10% of our body weight will result in immediate health benefits.
At the Boden Group, Charles Perkins Centre, we are studying the science of obesity and running clinical trials for weight loss. You can register here to express your interest.![]()
Nick Fuller, Charles Perkins Centre Research Program Leader, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Zero Sugar / One Month – by Becky Gillaspy

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We’ve reviewed books about the evils of sugar before, so what makes this one different?
This one has a focus on helping the reader quit it. It assumes we already know the evils of sugar (though it does cover that too).
It looks at the mechanisms of sugar addiction (habits-based and physiological), and how to safely and painlessly cut through those to come out the other side, free from sugar.
The author gives a day-by-day plan, for not only eliminating sugar, but also adding and including things to fill the gap it leaves, keeping us sated, energized, and happy along the way.
In the category of subjective criticism, it does also assume we want to lose weight, which may not be the case for many readers. But that’s a by-the-by and doesn’t detract from the useful guide to quitting sugar, whatever one’s reasons.
Bottom line: if you would like to quit sugar but find it hard, this book thinks of everything and walks you by the hand, making it easy.
Click here to check out Zero Sugar / One Month, and reap the health benefits!
Share This Post
-

Amid Wildfire Trauma, L.A. County Dispatches Mental Health Workers to Evacuees
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
PASADENA, Calif. — As Fernando Ramirez drove to work the day after the Eaton Fire erupted, smoke darkened the sky, ash and embers rained onto his windshield, and the air smelled of melting rubber and plastic.
He pulled to the side of the road and cried at the sight of residents trying to save their homes.
“I could see people standing on the roof, watering it, trying to protect it from the fire, and they just looked so hopeless,” said Ramirez, a community outreach worker with the Pasadena Public Health Department.
That evening, the 49-year-old volunteered for a 14-hour shift at the city’s evacuation center, as did colleagues who had also been activated for emergency medical duty. Running on adrenaline and little sleep after finding shelter for homeless people all day, Ramirez spent the night circulating among more than a thousand evacuees, offering wellness checks, companionship, and hope to those who looked distressed.
Local health departments, such as Ramirez’s, have become a key part of governments’ response to wildfires, floods, and other extreme weather events, which scientists say are becoming more intense and frequent due to climate change. The emotional toll of fleeing and possibly losing a home can help cause or exacerbate mental health conditions such as anxiety, depression, post-traumatic stress disorder, suicidal ideation, and substance use, according to health and climate experts.
Wildfires have become a recurring experience for many Angelenos, making it difficult for people to feel safe in their home or able to go about daily living, said Lisa Wong, director of the Los Angeles County Department of Mental Health. However, with each extreme weather event, the county has improved its support for evacuees, she said.
For instance, Wong said the county deployed a team of mental health workers trained to comfort evacuees without retraumatizing them, including by avoiding asking questions likely to bring up painful memories. The department has also learned to better track people’s health needs and redirect those who may find massive evacuation settings uncomfortable to other shelters or interim housing, Wong said. In those first days, the biggest goal is often to reduce people’s anxiety by providing them with information.
“We’ve learned that right when a crisis happens, people don’t necessarily want to talk about mental health,” said Wong, who staffed the evacuation site Jan. 8 with nine colleagues.
Instead, she and her team deliver a message of support: “This is really bad right now, but you’re not going to do this alone. We have a whole system set up for recovery too. Once you get past the initial shock of what happened — initial housing needs, medication needs, all those things — then there’s this whole pathway to recovery that we set up.”
The convention center in downtown Pasadena, which normally hosts home shows, comic cons, and trade shows, was transformed into an evacuation site with hundreds of cots. It was one of at least 13 shelters opened to serve more than 200,000 residents under evacuation orders.
The January wildfires have burned an estimated 64 square miles — an area larger than the city of Paris — and destroyed at least 12,300 buildings since they started Jan. 7. AccuWeather estimates the region will likely face more than $250 billion in economic losses from the blazes, surpassing the estimates from the state’s record-breaking 2020 wildfire season.
Lisa Patel, executive director of the Medical Society Consortium on Climate and Health, said she’s most concerned about low-income residents, who are less likely to access mental health support.
“There was a mental health crisis even before the pandemic,” said Patel, who is also a clinical associate professor of pediatrics at Stanford School of Medicine, referring to the covid-19 pandemic. “The pandemic made it worse. Now you lace in all of this climate change and these disasters into a health care system that isn’t set up to care for the people that already have mental health illness.”
Early research suggests exposure to large amounts of wildfire smoke can damage the brain and increase the risk of developing anxiety, she added.
At the Pasadena Convention Center, Elaine Santiago sat on a cot in a hallway as volunteers pulled wagons loaded with soup, sandwiches, bottled water, and other necessities.
Santiago said she drew comfort from being at the Pasadena evacuation center, knowing that she wasn’t alone in the tragedy.
“It sort of gives me a sense of peace at times,” Santiago said. “Maybe that’s weird. We’re all experiencing this together.”
She had been celebrating her 78th birthday with family when she fled her home in the small city of Sierra Madre, east of Pasadena. As she watched flames whip around her neighborhood, she, along with children and grandkids, scrambled to secure their dogs in crates and grabbed important documents before they left.
The widower had leaned on her husband in past emergencies, and now she felt lost.
“I did feel helpless,” Santiago said. “I figured I’m the head of the household; I should know what to do. But I didn’t know.”
Donny McCullough, who sat on a neighboring green cot draped in a Red Cross blanket, had fled his Pasadena home with his family early on the morning of Jan. 8. Without power at home, the 68-year-old stayed up listening for updates on a battery-powered radio. His eyes remained red from smoke irritation hours later.
“I had my wife and two daughters, and I was trying not to show fear, so I quietly, inside, was like, ‘Oh my God,’” said McCullough, a music producer and writer. “I’m driving away, looking at the house, wondering if it’s going to be the last time I’m going to see it.”
He saved his master recording from a seven-year music project, but he left behind his studio with all his other work from a four-decade career in music.
Not all evacuees arrived with family. Some came searching for loved ones. That’s one of the hardest parts of his shift, Ramirez said. The community outreach worker helped walk people around the building, cot by cot.
A week in, at least two dozen people had been killed in the wildfires.
The work takes a toll on disaster relief workers too. Ramirez said many feared losing their homes in the fires and some already had. He attends therapy weekly, which he said helps him manage his emotions.
At the evacuation center, Ramirez described being on autopilot.
“Some of us react differently. I tend to go into fight mode,” Ramirez said. “I react. I run towards the fire. I run towards personal service. Then once that passes, that’s when my trauma catches up with me.”
Need help? Los Angeles County residents in need of support can call the county’s mental health helpline at 1-800-854-7771. The national Suicide & Crisis Lifeline, 988, is also available for those who’d like to speak with someone confidentially, free of charge.
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post
-

Without Medicare Part B’s Shield, Patient’s Family Owes $81,000 for a Single Air-Ambulance Flight
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Without Medicare Part B’s Shield, Patient’s Family Owes $81,000 for a Single Air-Ambulance Flight
Debra Prichard was a retired factory worker who was careful with her money, including what she spent on medical care, said her daughter, Alicia Wieberg. “She was the kind of person who didn’t go to the doctor for anything.”
That ended last year, when the rural Tennessee resident suffered a devastating stroke and several aneurysms. She twice was rushed from her local hospital to Vanderbilt University Medical Center in Nashville, 79 miles away, where she was treated by brain specialists. She died Oct. 31 at age 70.
One of Prichard’s trips to the Nashville hospital was via helicopter ambulance. Wieberg said she had heard such flights could be pricey, but she didn’t realize how extraordinary the charge would be — or how her mother’s skimping on Medicare coverage could leave the family on the hook.
Then the bill came.
The Patient: Debra Prichard, who had Medicare Part A insurance before she died.
Medical Service: An air-ambulance flight to Vanderbilt University Medical Center.
Service Provider: Med-Trans Corp., a medical transportation service that is part of Global Medical Response, an industry giant backed by private equity investors. The larger company operates in all 50 states and says it has a total of 498 helicopters and airplanes.
Total Bill: $81,739.40, none of which was covered by insurance.
What Gives: Sky-high bills from air-ambulance providers have sparked complaints and federal action in recent years.
For patients with private insurance coverage, the No Surprises Act, which went into effect in 2022, bars air-ambulance companies from billing people more than they would pay if the service were considered “in-network” with their health insurers. For patients with public coverage, such as Medicare or Medicaid, the government sets payment rates at much lower levels than the companies charge.
But Prichard had opted out of the portion of Medicare that covers ambulance services.
That meant when the bill arrived less than two weeks after her death, her estate was expected to pay the full air-ambulance fee of nearly $82,000. The main assets are 12 acres of land and her home in Decherd, Tennessee, where she lived for 48 years and raised two children. The bill for a single helicopter ride could eat up roughly a third of the estate’s value, said Wieberg, who is executor.
The family’s predicament stems from the complicated nature of Medicare coverage.
Prichard was enrolled only in Medicare Part A, which is free to most Americans 65 or older. That section of the federal insurance program covers inpatient care, and it paid most of her hospital bills, her daughter said.
But Prichard declined other Medicare coverage, including Part B, which handles such things as doctor visits, outpatient treatment, and ambulance rides. Her daughter suspects she skipped that coverage to avoid the premiums most recipients pay, which currently are about $175 a month.
Loren Adler, a health economist for the Brookings Institution who studies ambulance bills, estimated the maximum charge that Medicare would have allowed for Prichard’s flight would have been less than $10,000 if she’d signed up for Part B. The patient’s share of that would have been less than $2,000. Her estate might have owed nothing if she’d also purchased supplemental “Medigap” coverage, as many Medicare members do to cover things like coinsurance, he said.
Nicole Michel, a spokesperson for Global Medical Response, the ambulance provider, agreed with Adler’s estimate that Medicare would have limited the charge for the flight to less than $10,000. But she said the federal program’s payment rates don’t cover the cost of providing air-ambulance services.
“Our patient advocacy team is actively engaged with Ms. Wieberg’s attorney to determine if there was any other applicable medical coverage on the date of service that we could bill to,” Michel wrote in an email to KFF Health News. “If not, we are fully committed to working with Ms. Wieberg, as we do with all our patients, to find an equitable solution.”
The Resolution: In mid-February, Wieberg said the company had not offered to reduce the bill.
Wieberg said she and the attorney handling her mother’s estate both contacted the company, seeking a reduction in the bill. She said she also contacted Medicare officials, filled out a form on the No Surprises Act website, and filed a complaint with Tennessee regulators who oversee ambulance services. She said she was notified Feb. 12 that the company filed a legal claim against the estate for the entire amount.
Wieberg said other health care providers, including ground ambulance services and the Vanderbilt hospital, wound up waiving several thousand dollars in unpaid fees for services they provided to Prichard that are normally covered by Medicare Part B.
But as it stands, Prichard’s estate owes about $81,740 to the air-ambulance company.
More from Bill of the Month
- The Colonoscopies Were Free. But the ‘Surgical Trays’ Came With $600 Price Tags. Jan 25, 2024
- When a Quick Telehealth Visit Yields Multiple Surprises Beyond a Big Bill Dec 19, 2023
- Out for Blood? For Routine Lab Work, the Hospital Billed Her $2,400 Nov 21, 2023
The Takeaway: People who are eligible for Medicare are encouraged to sign up for Part B, unless they have private health insurance through an employer or spouse.
“If someone with Medicare finds that they are having difficulty paying the Medicare Part B premiums, there are resources available to help compare Medicare coverage choices and learn about options to help pay for Medicare costs,” Meena Seshamani, director of the federal Center for Medicare, said in an email to KFF Health News.
She noted that every state offers free counseling to help people navigate Medicare.
In Tennessee, that counseling is offered by the State Health Insurance Assistance Program. Its director, Lori Galbreath, told KFF Health News she wishes more seniors would discuss their health coverage options with trained counselors like hers.
“Every Medicare recipient’s experience is different,” she said. “We can look at their different situations and give them an unbiased view of what their next best steps could be.”
Counselors advise that many people with modest incomes enroll in a Medicare Savings Program, which can cover their Part B premiums. In 2023, Tennessee residents could qualify for such assistance if they made less than $1,660 monthly as a single person or $2,239 as a married couple. Many people also could obtain help with other out-of-pocket expenses, such as copays for medical services.
Wieberg, who lives in Missouri, has been preparing the family home for sale.
She said the struggle over her mother’s air-ambulance bill makes her wonder why Medicare is split into pieces, with free coverage for inpatient care under Part A, but premiums for coverage of other crucial services under Part B.
“Anybody past the age of 70 is likely going to need both,” she said. “And so why make it a decision of what you can afford or not afford, or what you think you’re going to use or not use?”
Bill of the Month is a crowdsourced investigation by KFF Health News and NPR that dissects and explains medical bills. Do you have an interesting medical bill you want to share with us? Tell us about it!
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post

-

‘Naked carbs’ and ‘net carbs’ – what are they and should you count them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
According to social media, carbs come in various guises: naked carbs, net carbs, complex carbs and more.
You might be wondering what these terms mean or if all carbs are really the same. If you are into “carb counting” or “cutting carbs”, it’s important to make informed decisions about what you eat.
What are carbs?
Carbohydrates, or “carbs” for short, are one of the main sources of energy we need for brain function, muscle movement, digestion and pretty much everything our bodies do.
There are two classifications of carbs, simple and complex. Simple carbs have one or two sugar molecules, while complex carbs are three or more sugar molecules joined together. For example, table sugar is a simple carb, but starch in potatoes is a complex carb.
All carbs need to be broken down into individual molecules by our digestive enzymes to be absorbed. Digestion of complex carbs is a much slower process than simple carbs, leading to a more gradual blood sugar increase.
Fibre is also considered a complex carb, but it has a structure our body is not capable of digesting. This means we don’t absorb it, but it helps with the movement of our stool and prevents constipation. Our good gut bacteria also love fibre as they can digest it and use it for energy – important for a healthy gut.
What about ‘naked carbs’?
“Naked carbs” is a popular term usually used to refer to foods that are mostly simple carbs, without fibre or accompanying protein or fat. White bread, sugary drinks, jams, sweets, white rice, white flour, crackers and fruit juice are examples of these foods. Ultra-processed foods, where the grains are stripped of their outer layers (including fibre and most nutrients) leaving “refined carbs”, also fall into this category.
One of the problems with naked carbs or refined carbs is they digest and absorb quickly, causing an immediate rise in blood sugar. This is followed by a rapid spike in insulin (a hormone that signals cells to remove sugar from blood) and then a drop in blood sugar. This can lead to hunger and cravings – a vicious cycle that only gets worse with eating more of the same foods.

Naked carbs can make blood sugars spike then crash.
Pexels/Alexander GreyWhat about ‘net carbs’?
This is another popular term tossed around in dieting discussions. Net carbs refer to the part of the carb food that we actually absorb.
Again, fibre is not easily digestible. And some carb-rich foods contain sugar alcohols, such as sweeteners (like xylitol and sorbitol) that have limited absorption and little to no effect on blood sugar. Deducting the value of fibre and sugar alcohols from the total carbohydrate content of a food gives what’s considered its net carb value.
For example, canned pear in juice has around 12.3g of “total carbohydrates” per 100g, including 1.7g carb + 1.7g fibre + 1.9g sugar alcohol. So its net carb is 12.3g – 1.7g – 1.9g = 8.7g. This means 8.7g of the 12.3g total carbs impacts blood sugar.
The nutrition labels on packaged foods in Australia and New Zealand usually list fibre separately to carbohydrates, so the net carbs have already been calculated. This is not the case in other countries, where “total carbohydrates” are listed.
Does it matter though?
Whether or not you should care about net or naked carbs depends on your dietary preferences, health goals, food accessibility and overall nutritional needs. Generally speaking, we should try to limit our consumption of simple and refined carbs.
The latest World Health Organization guidelines recommend our carbohydrate intake should ideally come primarily from whole grains, vegetables, fruits and pulses, which are rich in complex carbs and fibre. This can have significant health benefits (to regulate hunger, improve cholesterol or help with weight management) and reduce the risk of conditions such as heart disease, obesity and colon cancer.
In moderation, naked carbs aren’t necessarily bad. But pairing them with fats, protein or fibre can slow down the digestion and absorption of sugar. This can help to stabilise blood sugar levels, prevent spikes and crashes and support personal weight management goals. If you’re managing diabetes or insulin resistance, paying attention to the composition of your meals, and the quality of your carbohydrate sources is essential.
A ketogenic (high fat, low carb) diet typically restricts carb intake to between 20 and 50g each day. But this carb amount refers to net carbs – so it is possible to eat more carbs from high-fibre sources.
Choose complex carbohydrates with lots of fibre.
ShutterstockSome tips to try
Some simple strategies can help you get the most out of your carb intake:
reduce your intake of naked carbs and foods high in sugar and white flour, such as white bread, table sugar, honey, lollies, maple syrup, jam, and fruit juice
opt for protein- and fibre-rich carbs. These include oats, sweet potatoes, nuts, avocados, beans, whole grains and broccoli
if you are eating naked carbs, dress them up with some protein, fat and fibre. For example, top white bread with a nut butter rather than jam
if you are trying to reduce the carb content in your diet, be wary of any symptoms of low blood glucose, including headaches, nausea, and dizziness
- working with a health-care professional such as an accredited practising dietitian or your GP can help develop an individualised diet plan that meets your specific needs and goals.
Correction: this article has been updated to indicate how carbohydrates are listed on food nutrition labels in Australia and New Zealand.

Saman Khalesi, Senior Lecturer and Discipline Lead in Nutrition, School of Health, Medical and Applied Sciences, CQUniversity Australia; Anna Balzer, Lecturer, Medical Science School of Health, Medical and Applied Sciences, CQUniversity Australia; Charlotte Gupta, Postdoctoral research fellow, CQUniversity Australia; Chris Irwin, Senior Lecturer in Nutrition and Dietetics, School of Health Sciences & Social Work, Griffith University, and Grace Vincent, Senior Lecturer, Appleton Institute, CQUniversity Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
The Exercises That Help Keep Breast Cancer At Bay
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
For women, our lifetime risk of being diagnosed with breast cancer is about 1 in 7, before we take into account any added risk or protective factors.
For men, it’s more like 1 in 556, which again, is before taking into account any added risk or protective factors.
Here’s a good place to start on improving those odds: How To Triple Your Breast Cancer Survival Chances
And for that matter, check out: 8 Signs On Your Breast You Shouldn’t Ignore
And for those concerned (or even just curious) about the pros and cons of menopausal HRT when it comes to breast cancer:
The Hormone Therapy That Reduces Breast Cancer Risk & More ← this is actually very important to understand, as otherwise it’s easy to accidentally self-sabotage and increase one’s overall mortality risk
So, what’s this about exercise and breast cancer?
There are two things to focus on
No, not those.
Well, yes, those, but also: aerobic exercise and resistance training.
A research team (Dr. Alice Avancini et al.) analysed data from 22 randomized controlled trials (total n=968 participants) that investigated the effects of exercise on various pro-inflammatory biomarkers (mostly interleukin variants, but also c-reactive proteins) that are known to increase breast cancer reoccurrence risk.
What they found was:
❝Exercise induced small to large significant reductions in IL-6 (SMD = -0.85; 95% CI = -1.68 to -0.02; p = .05) and TNF-α (SMD = -0.40; 95% CI = -0.81 to 0.01; p = .05) and a trend for a decrease in CRP.
When stratifying by exercise mode, trends toward reduction in IL-6 and TNF-α were observed for combined exercise, whilst changes were not generally affected by exercise program duration❞
The “combined exercise” mentioned?
Aerobic exercise and resistance training.
This is important, because as regular 10almonds readers may remember…
What Your Metabolism Says About How Aggressive Breast Cancer Is Likely To Be For You ← this makes a huge difference to survival chances
So, this study’s findings are very consistent with that, because:
- Aerobic training increases cardiovascular fitness, improving metabolism
- Resistance training increases muscle mass, improving metabolism*
*because muscle “costs” calories to maintain, prompting an increase in metabolism, whereas fat prompts our metabolism to slow, to conserve energy to face the obvious food shortage that must be coming
See also: Stop Cancer 20 Years Ago
Want to learn more?
Here’s the best book we’ve read on breast cancer survival:
The Smart Woman’s Guide to Breast Cancer – by Dr. Jenn Simmons
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Taking A Trip Through The Evidence On Psychedelics
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.

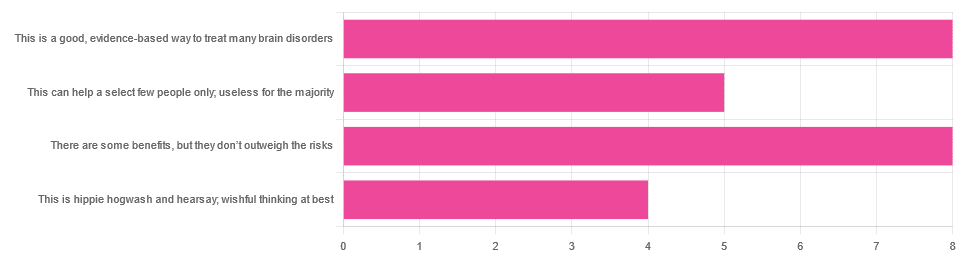
In Tuesday’s newsletter, we asked you for your opinions on the medicinal use of psychedelics, and got the above-depicted, below-described, set of responses:
- 32% said “This is a good, evidence-based way to treat many brain disorders”
- 32% said “There are some benefits, but they don’t outweigh the risks”
- 20% said “This can help a select few people only; useless for the majority”
- 16% said “This is hippie hogwash and hearsay; wishful thinking at best”
Quite a spread of answers, so what does the science say?
This is hippie hogwash and hearsay; wishful thinking at best! True or False?
False! We’re tackling this one first, because it’s easiest to answer:
There are some moderately-well established [usually moderate] clinical benefits from some psychedelics for some people.
If that sounds like a very guarded statement, it is. Part of this is because “psychedelics” is an umbrella term; perhaps we should have conducted separate polls for psilocybin, MDMA, ayahuasca, LSD, ibogaine, etc, etc.
In fact: maybe we will do separate main features for some of these, as there is a lot to say about each of them separately.
Nevertheless, looking at the spread of research as it stands for psychedelics as a category, the answers are often similar across the board, even when the benefits/risks may differ from drug to drug.
To speak in broad terms, if we were to make a research summary for each drug it would look approximately like this in each case:
- there has been research into this, but not nearly enough, as “the war on drugs” may well have manifestly been lost (the winner of the war being: drugs; still around and more plentiful than ever), but it did really cramp science for a few decades.
- the studies are often small, heterogenous (often using moderately wealthy white student-age population samples), and with a low standard of evidence (i.e. the methodology often has some holes that leave room for reasonable doubt).
- the benefits recorded are often small and transient.
- in their favor, though, the risks are also generally recorded as being quite low, assuming proper safe administration*.
*Illustrative example:
Person A takes MDMA in a club, dances their cares away, has had only alcohol to drink, sweats buckets but they don’t care because they love everyone and they see how we’re all one really and it all makes sense to them and then they pass out from heat exhaustion and dehydration and suffer kidney damage (not to mention a head injury when falling) and are hospitalized and could die;
Person B takes MDMA in a lab, is overwhelmed with a sense of joy and the clarity of how their participation in the study is helping humanity; they want to hug the researcher and express their gratitude; the researcher reminds them to drink some water.
Which is not to say that a lab is the only safe manner of administration; there are many possible setups for supervised usage sites. But it does mean that the risks are often as much environmental as they are risks inherent to the drug itself.
Others are more inherent to the drug itself, such as adverse cardiac events for some drugs (ibogaine is one that definitely needs medical supervision, for example).
For those who’d like to see numbers and clinical examples of the bullet points we gave above, here you go; this is a great (and very readable) overview:
NIH | Evidence Brief: Psychedelic Medications for Mental Health and Substance Use Disorders
Notwithstanding the word “brief” (intended in the sense of: briefing), this is not especially brief and is rather an entire book (available for free, right there!), but we do recommend reading it if you have time.
This can help a select few people only; useless for the majority: True or False?
True, technically, insofar as the evidence points to these drugs being useful for such things as depression, anxiety, PTSD, addiction, etc, and estimates of people who struggle with mental health issues in general is often cited as being 1 in 4, or 1 in 5. Of course, many people may just have moderate anxiety, or a transient period of depression, etc; many, meanwhile, have it worth.
In short: there is a very large minority of people who suffer from mental health issues that, for each issue, there may be one or more psychedelic that could help.
This is a good, evidence-based way to treat many brain disorders: True or False?
True if and only if we’re willing to accept the so far weak evidence that we discussed above. False otherwise, while the jury remains out.
One thing in its favor though is that while the evidence is weak, it’s not contradictory, insofar as the large preponderance of evidence says such therapies probably do work (there aren’t many studies that returned negative results); the evidence is just weak.
When a thousand scientists say “we’re not completely sure, but this looks like it helps; we need to do more research”, then it’s good to believe them on all counts—the positivity and the uncertainty.
This is a very different picture than we saw when looking at, say, ear candling or homeopathy (things that the evidence says simply do not work).
We haven’t been linking individual studies so far, because that book we linked above has many, and the number of studies we’d have to list would be:
n = number of kinds of psychedelic drugs x number of conditions to be treated
e.g. how does psilocybin fare for depression, eating disorders, anxiety, addiction, PTSD, this, that, the other; now how does ayahuasca fare for each of those, and so on for each drug and condition; at least 25 or 30 as a baseline number, and we don’t have that room.
But here are a few samples to finish up:
- Psilocybin as a New Approach to Treat Depression and Anxiety in the Context of Life-Threatening Diseases—A Systematic Review and Meta-Analysis of Clinical Trials
- Therapeutic Use of LSD in Psychiatry: A Systematic Review of Randomized-Controlled Clinical Trials
- Efficacy of Psychoactive Drugs for the Treatment of Posttraumatic Stress Disorder: A Systematic Review of MDMA, Ketamine, LSD and Psilocybin
- Changes in self-rumination and self-compassion mediate the effect of psychedelic experiences on decreases in depression, anxiety, and stress.
- Psychedelic Treatments for Psychiatric Disorders: A Systematic Review and Thematic Synthesis of Patient Experiences in Qualitative Studies
- Repeated lysergic acid diethylamide (LSD) reverses stress-induced anxiety-like behavior, cortical synaptogenesis deficits and serotonergic neurotransmission decline
In closing…
The general scientific consensus is presently “many of those drugs may ameliorate many of those conditions, but we need a lot more research before we can say for sure”.
On a practical level, an important take-away from this is twofold:
- drugs, even those popularly considered recreational, aren’t ontologically evil, generally do have putative merits, and have been subject to a lot of dramatization/sensationalization, especially by the US government in its famous war on drugs.
- drugs, even those popularly considered beneficial and potentially lifechangingly good, are still capable of doing great harm if mismanaged, so if putting aside “don’t do drugs” as a propaganda of the past, then please do still hold onto “don’t do drugs alone”; trained professional supervision is a must for safety.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: