Hazelnuts vs Cashews – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing hazelnuts to cashews, we picked the hazelnuts.
Why?
It’s close! This one’s interesting…
In terms of macros, hazelnuts have more fiber and fats, while cashews have more protein and carbs. All in all, all good stuff all around; maybe a win for one or the other depending on your priorities. We’d pick hazelnuts here, but your preference may vary.
When it comes to vitamins, hazelnuts have more of vitamins A, B1, B2, B3, B5, B6, B9, C, and E, while cashews have more vitamin K. An easy win for hazelnuts here, and the margins weren’t close.
In the category of minerals, hazelnuts have more calcium, manganese, and potassium, while cashews have more copper, iron, magnesium, phosphorus, selenium, and zinc. This is a win for cashews, but it’s worth noting that cup for cup, both of these nuts provide more than the daily requirement of most of those minerals. This means that in practical terms, it doesn’t matter too much that (for example), while cashews provide 732% of the daily requirement for copper, hazelnuts “only” provide 575%. So while this category remains a victory for cashews, it’s something of a “on paper” thing for the most part.
Adding up the sections (ambivalent + clear win for hazelnuts + nominal win for cashews) means that in total today we’re calling it in favour of hazelnuts… But as ever, enjoy both, because both are good and so is diversity!
Want to learn more?
You might like to read:
Why You Should Diversify Your Nuts
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is a ‘vaginal birth after caesarean’ or VBAC?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A vaginal birth after caesarean (known as a VBAC) is when a woman who has had a caesarean has a vaginal birth down the track.
In Australia, about 12% of women have a vaginal birth for a subsequent baby after a caesarean. A VBAC is much more common in some other countries, including in several Scandinavian ones, where 45-55% of women have one.
So what’s involved? What are the risks? And who’s most likely to give birth vaginally the next time round?

MVelishchuk/Shutterstock What happens? What are the risks?
When a woman chooses a VBAC she is cared for much like she would during a planned vaginal birth.
However, an induction of labour is avoided as much as possible, due to the slightly increased risk of the caesarean scar opening up (known as uterine rupture). This is because the medication used in inductions can stimulate strong contractions that put a greater strain on the scar.
In fact, one of the main reasons women may be recommended to have a repeat caesarean over a vaginal birth is due to an increased chance of her caesarean scar rupturing.
This is when layers of the uterus (womb) separate and an emergency caesarean is needed to deliver the baby and repair the uterus.
Uterine rupture is rare. It occurs in about 0.2-0.7% of women with a history of a previous caesarean. A uterine rupture can also happen without a previous caesarean, but this is even rarer.
However, uterine rupture is a medical emergency. A large European study found 13% of babies died after a uterine rupture and 10% of women needed to have their uterus removed.
The risk of uterine rupture increases if women have what’s known as complicated or classical caesarean scars, and for women who have had more than two previous caesareans.
Most care providers recommend you avoid getting pregnant again for around 12 months after a caesarean, to allow full healing of the scar and to reduce the risk of the scar rupturing.
National guidelines recommend women attempt a VBAC in hospital in case emergency care is needed after uterine rupture.
During a VBAC, recommendations are for closer monitoring of the baby’s heart rate and vigilance for abnormal pain that could indicate a rupture is happening.
If labour is not progressing, a caesarean would then usually be advised.
Giving birth in hospital is recommended for a vaginal birth after a caesarean. christinarosepix/Shutterstock Why avoid multiple caesareans?
There are also risks with repeat caesareans. These include slower recovery, increased risks of the placenta growing abnormally in subsequent pregnancies (placenta accreta), or low in front of the cervix (placenta praevia), and being readmitted to hospital for infection.
Women reported birth trauma and post-traumatic stress more commonly after a caesarean than a vaginal birth, especially if the caesarean was not planned.
Women who had a traumatic caesarean or disrespectful care in their previous birth may choose a VBAC to prevent re-traumatisation and to try to regain control over their birth.
We looked at what happened to women
The most common reason for a caesarean section in Australia is a repeat caesarean. Our new research looked at what this means for VBAC.
We analysed data about 172,000 low-risk women who gave birth for the first time in New South Wales between 2001 and 2016.
We found women who had an initial spontaneous vaginal birth had a 91.3% chance of having subsequent vaginal births. However, if they had a caesarean, their probability of having a VBAC was 4.6% after an elective caesarean and 9% after an emergency one.
We also confirmed what national data and previous studies have shown – there are lower VBAC rates (meaning higher rates of repeat caesareans) in private hospitals compared to public hospitals.
We found the probability of subsequent elective caesarean births was higher in private hospitals (84.9%) compared to public hospitals (76.9%).
Our study did not specifically address why this might be the case. However, we know that in private hospitals women access private obstetric care and experience higher caesarean rates overall.
What increases the chance of success?
When women plan a VBAC there is a 60-80% chance of having a vaginal birth in the next birth.
The success rates are higher for women who are younger, have a lower body mass index, have had a previous vaginal birth, give birth in a home-like environment or with midwife-led care.
For instance, an Australian study found women who accessed continuity of care with a midwife were more likely to have a successful VBAC compared to having no continuity of care and seeing different care providers each time.
An Australian national survey we conducted found having continuity of care with a midwife when planning a VBAC can increase women’s sense of control and confidence, increase their chance to be upright and active in labour and result in a better relationship with their health-care provider.
Seeing the same midwife throughout your maternity care can help. Tyler Olson/Shutterstock Why is this important?
With the rise of caesareans globally, including in Australia, it is more important than ever to value vaginal birth and support women to have a VBAC if this is what they choose.
Our research is also a reminder that how a woman gives birth the first time greatly influences how she gives birth after that. For too many women, this can lead to multiple caesareans, not all of them needed.
Hannah Dahlen, Professor of Midwifery, Associate Dean Research and HDR, Midwifery Discipline Leader, Western Sydney University; Hazel Keedle, Senior Lecturer of Midwifery, Western Sydney University, and Lilian Peters, Adjunct Research Fellow, Western Sydney University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Treat Your Own Hip – by Robin McKenzie
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We previously reviewed another book by this author in this series, “Treat Your Own Knee”, and today it’s the same deal, but for the hip.
A quick note about the author first: a physiotherapist and not a doctor, but with over 40 years of practice to his name and 33 letters after his name (CNZM OBE FCSP (Hon) FNZSP (Hon) Dip MDT Dip MT), he seems to know his stuff.
He takes the reader through first diagnosing the nature of the pain (and how to rule out, for example, a back problem manifesting as hip pain, rather than a hip problem per se—and points to his own “Treat Your Own Back” manual if it turns out that that’s your problem instead), and then treating it. A bold claim, the kind that many people’s lawyers don’t let them make, but once again, this guy is pretty much the expert when it comes to this. Ask any other physiotherapist, and they probably have several of his books on their shelf.
The treatments recommend are tailored to the results of various diagnostic flowcharts; essentially troubleshooting your hip. However, they mainly consist of exercises (perhaps the greatest value of the book), and lifestyle adjustments (these ones, 10almonds readers probably know already, but a reminder never hurts).
The explanations are thorough while still being comprehensible, and there is zero sensationalization or fluff. It is straight to the point, and clearly illustrated too with diagrams and photographs.
Bottom line: if you’re looking for a “one-stop shop” for diagnosing and treating your bad hip, then this is it.
Click here to check out Treat Your Own Hip, and indeed Treat Your Own Hip!
PS: if you have musculoskeletal problems elsewhere in your body, you might want to check out the rest of his body parts series (neck, back, shoulder, wrist, knee, ankle) for the one that’s tailored to your specific problem.
Share This Post
-

An Important Way That Love Gets Eroded
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It is unusual for a honeymoon period to last forever, but some relationships fair a lot better than others. Not just in terms of staying together vs separating, but in terms of happiness and satisfaction in the relationship. What’s the secret? There are many, but here’s one of them…
Communication
In this video, the case is made for a specific aspect of communication: airing grievances.
Superficially, this doesn’t seem like a recipe for happiness, but it is one important ingredient—that it’s dangerously easy to let small grievances add up and eat away at one’s love and patience, until one day resentment outweighs attachment, and at that point, it often becomes a case of “checking out before you leave”, remaining in the relationship more due to inertia than volition.
Which, in turn, will likely start to cause resentment on the other side, and eventually things will crumble and/or explode.
In contrast, if we make sure to speak our feelings clearly (10almonds note, not in the video: we think that doing so compassionately is also important), the bad as well as the good, then it means that:
- things don’t stack up and fester (there will less likely be a “final straw” if we are regularly removing straws)
- there is an opportunity for change (in contrast, our partner would be unlikely to adjust anything to correct a problem they don’t know about)
- all but the most inclined-to-anxiety partners can rest easy, because they know that if we had a problem, we’d tell them
This is definitely only one critical aspect of communication; this video for example says nothing about actually being affectionate with one’s partner, or making sure to accept emotional bids for connection (per that story that goes “I knew my marriage was over when he wouldn’t come look at the tomatoes I grew”), but it is one worth considering—even if we at 10almonds would advise being gentle yet honest, and where possible balancing, in aggregate if not in the moment, with positive things (per Gottman’s ratio of 5:1 good moments to bad, being the magic number for marriages that “work”).
For more on why it’s so important to be able to safely air grievances, see:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Seriously Useful Communication Skills! ← this deals with some of the important gaps left by the video
Take care!
Share This Post



Related Posts
-

Frozen/Thawed/Refrozen Meat: How Much Is Safety, And How Much Is Taste?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What You Can (And Can’t) Safely Do With Frozen Meat

Yesterday, we asked you:
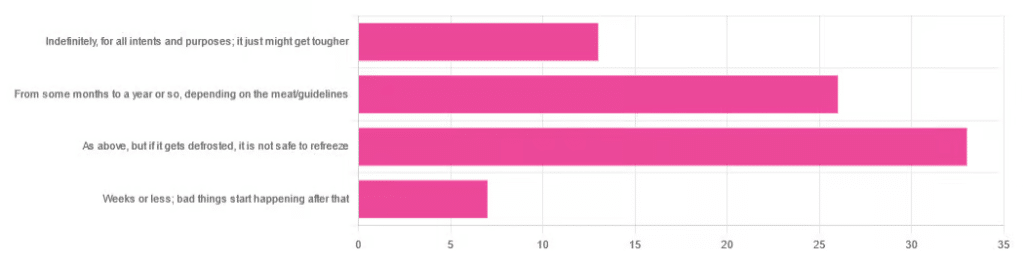
❝You have meat in the freezer. How long is it really safe to keep it?❞
…and got a range of answers, mostly indicating to a) follow the instructions (a very safe general policy) and b) do not refreeze if thawed because that would be unsafe. Fewer respondents indicated that meat could be kept for much longer than guidelines say, or conversely, that it should only be kept for weeks or less.
So, what does the science say?
Meat can be kept indefinitely (for all intents and purposes) in a freezer; it just might get tougher: True or False?
False, assuming we are talking about a normal household electrical freezer that bottoms out at about -18℃ / 0℉.
Fun fact: cryobiologists cryopreserve tissue samples (so basically, meat) at -196℃ / -320℉, and down at those temperatures, the tissues will last a lot longer than you will (and, for all practical purposes: indefinitely). There are other complications with doing so (such as getting the sample through the glass transition point without cracking it during the vitrification process) but those are beyond the scope of this article.
If you remember back to your physics or perhaps chemistry classes at school, you’ll know that molecules move more quickly at higher temperatures, and more slowly at lower ones, only approaching true stillness as they near absolute zero (-273℃ / -459℉ / 0K ← we’re not saying it’s ok, although it is; rather, that is zero kelvin; no degree sign is used with kelvins)
That means that when food is frozen, the internal processes aren’t truly paused; it’s just slowed to a point of near imperceptibility.
So, all the way up at the relatively warm temperatures of a household freezer, a lot of processes are still going on.
What this means in practical terms: those guidelines saying “keep in the freezer for up to 4 months”, “keep in the freezer for up to 9 months”, “keep in the freezer for up to 12 months” etc are being honest with you.
More or less, anyway! They’ll usually underestimate a little to be on the safe side—but so should you.
Bad things start happening within weeks at most: True or False?
False, for all practical purposes. Again, assuming a normal and properly-working household freezer as described above.
(True, technically but misleadingly: the bad things never stopped; they just slowed down to a near imperceptible pace—again, as described above)
By “bad” here we should clarify we mean “dangerous”. One subscriber wrote:
❝Meat starts losing color and flavor after being in the freezer for too long. I keep meat in the freezer for about 2 months at the most❞
…and as a matter of taste, that’s fair enough!
It is unsafe to refreeze meat that has been thawed: True or False?
False! Assuming it has otherwise been kept chilled, just the same as for fresh meat.
Food poisoning comes from bacteria, and there is nothing about the meat previously having been frozen that will make it now have more bacteria.
That means, for example…
- if it was thawed (but chilled) for a period of time, treat it like you would any other meat that has been chilled for that period of time (so probably: use it or freeze it, unless it’s been more than a few days)
- if it was thawed (and at room temperature) for a period of time, treat it like you would any other meat that has been at room temperature for that period of time (so probably: throw it out, unless the period of time is very small indeed)
The USDA gives for 2 hours max at room temperature before considering it unsalvageable, by the way.
However! Whenever you freeze meat (or almost anything with cells, really), ice crystals will form in and between cells. How much ice crystallization occurs depends on several variables, with how much water there is present in the food is usually the biggest factor (remember that animal cells are—just like us—mostly water).
Those ice crystals will damage the cell walls, causing the food to lose structural integrity. When you thaw it out, the ice crystals will disappear but the damage will be left behind (this is what “freezer burn” is).
So if your food seems a little “squishy” after having been frozen and thawed, that’s why. It’s not rotten; it’s just been stabbed countless times on a microscopic level.
The more times you freeze and thaw and refreeze food, the more this will happen. Your food will degrade in structural integrity each time, but the safety of it won’t have changed meaningfully.
Want to know more?
Further reading:
You can thaw and refreeze meat: five food safety myths busted
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
For many who are suffering with prolonged grief, the holidays can be a time to reflect and find meaning in loss
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The holiday season is meant to be filled with joy, connection and celebration of rituals. Many people, however, are starkly reminded of their grief this time of year and of whom – or what – they have lost.
The added stress of the holiday season doesn’t help. Studies show that the holidays negatively affect many people’s mental health.
While COVID-19-related stressors may have lessened, the grief from change and loss that so many endured during the pandemic persists. This can cause difficult emotions to resurface when they are least expected.
I am a licensed therapist and trauma-sensitive yoga instructor. For the last 12 years, I’ve helped clients and families manage grief, depression, anxiety and complex trauma. This includes many health care workers and first responders who have recounted endless stories to me about how the pandemic increased burnout and affected their mental health and quality of life.
I developed an online program that research shows has improved their well-being. And I’ve observed firsthand how much grief and sadness can intensify during the holidays.
Post-pandemic holidays and prolonged grief
During the pandemic, family dynamics, close relationships and social connections were strained, mental health problems increased or worsened, and most people’s holiday traditions and routines were upended.
Those who lost a loved one during the pandemic may not have been able to practice rituals such as holding a memorial service, further delaying the grieving process. As a result, holiday traditions may feel more painful now for some. Time off from school or work can also trigger more intense feelings of grief and contribute to feelings of loneliness, isolation or depression.
Sometimes feelings of grief are so persistent and severe that they interfere with daily life. For the past several decades, researchers and clinicians have been grappling with how to clearly define and treat complicated grief that does not abate over time.
In March 2022, a new entry to describe complicated grief was added to the Diagnostic and Statistical Manual of Mental Disorders, or DSM, which classifies a spectrum of mental health disorders and problems to better understand people’s symptoms and experiences in order to treat them.
This newly defined condition is called prolonged grief disorder. About 10% of bereaved adults are at risk, and those rates appear to have increased in the aftermath of the pandemic.
People with prolonged grief disorder experience intense emotions, longing for the deceased, or troublesome preoccupation with memories of their loved one. Some also find it difficult to reengage socially and may feel emotionally numb. They commonly avoid reminders of their loved one and may experience a loss of identity and feel bleak about their future. These symptoms persist nearly every day for at least a month. Prolonged grief disorder can be diagnosed at least one year after a significant loss for adults and at least six months after a loss for children.
I am no stranger to complicated grief: A close friend of mine died by suicide when I was in college, and I was one of the last people he spoke to before he ended his life. This upended my sense of predictability and control in my life and left me untangling the many existential themes that suicide loss survivors often face.
How grieving alters brain chemistry
Research suggests that grief not only has negative consequences for a person’s physical health, but for brain chemistry too.
The feeling of grief and intense yearning may disrupt the neural reward systems in the brain. When bereaved individuals seek connection to their lost loved one, they are craving the chemical reward they felt before their loss when they connected with that person. These reward-seeking behaviors tend to operate on a feedback loop, functioning similar to substance addiction, and could be why some people get stuck in the despair of their grief.
One study showed an increased activation of the amygdala when showing death-related images to people who are dealing with complicated grief, compared to adults who are not grieving a loss. The amygdala, which initiates our fight or flight response for survival, is also associated with managing distress when separated from a loved one. These changes in the brain might explain the great impact prolonged grief has on someone’s life and their ability to function.
Recognizing prolonged grief disorder
Experts have developed scales to help measure symptoms of prolonged grief disorder. If you identify with some of these signs for at least one year, it may be time to reach out to a mental health professional.
Grief is not linear and doesn’t follow a timeline. It is a dynamic, evolving process that is different for everyone. There is no wrong way to grieve, so be compassionate to yourself and don’t make judgments on what you should or shouldn’t be doing.
Increasing your social supports and engaging in meaningful activities are important first steps. It is critical to address any preexisting or co-occurring mental health concerns such as anxiety, depression or post-traumatic stress.
It can be easy to confuse grief with depression, as some symptoms do overlap, but there are critical differences.
If you are experiencing symptoms of depression for longer than a few weeks and it is affecting your everyday life, work and relationships, it may be time to talk with your primary care doctor or therapist.
A sixth stage of grief
I have found that naming the stage of grief that someone is experiencing helps diminish the power it might have over them, allowing them to mourn their loss.
For decades, most clinicians and researchers have recognized five stages of grief: denial/shock, anger, depression, bargaining and acceptance.
But “accepting” your grief doesn’t sit well for many. That is why a sixth stage of grief, called “finding meaning,” adds another perspective. Honoring a loss by reflecting on its meaning and the weight of its impact can help people discover ways to move forward. Recognizing how one’s life and identity are different while making space for your grief during the holidays might be one way to soften the despair.
When my friend died by suicide, I found a deeper appreciation for what he brought into my life, soaking up the moments he would have enjoyed, in honor of him. After many years, I was able to find meaning by spreading mental health awareness. I spoke as an expert presenter for suicide prevention organizations, wrote about suicide loss and became certified to teach my local community how to respond to someone experiencing signs of mental health distress or crisis through Mental Health First Aid courses. Finding meaning is different for everyone, though.
Sometimes, adding a routine or holiday tradition can ease the pain and allow a new version of life, while still remembering your loved one. Take out that old recipe or visit your favorite restaurant you enjoyed together. You can choose to stay open to what life has to offer, while grieving and honoring your loss. This may offer new meaning to what – and who – is around you.
If you need emotional support or are in a mental health crisis, dial 988 or chat online with a crisis counselor.

Mandy Doria, Assistant Professor of Psychiatry, University of Colorado Anschutz Medical Campus
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

If I’m diagnosed with one cancer, am I likely to get another?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Receiving a cancer diagnosis is life-changing and can cause a range of concerns about ongoing health.
Fear of cancer returning is one of the top health concerns. And managing this fear is an important part of cancer treatment.
But how likely is it to get cancer for a second time?
Why can cancer return?
While initial cancer treatment may seem successful, sometimes a few cancer cells remain dormant. Over time, these cancer cells can grow again and may start to cause symptoms.
This is known as cancer recurrence: when a cancer returns after a period of remission. This period could be days, months or even years. The new cancer is the same type as the original cancer, but can sometimes grow in a new location through a process called metastasis.
Actor Hugh Jackman has gone public about his multiple diagnoses of basal cell carcinoma (a type of skin cancer) over the past decade.
The exact reason why cancer returns differs depending on the cancer type and the treatment received. Research is ongoing to identify genes associated with cancers returning. This may eventually allow doctors to tailor treatments for high-risk people.
What are the chances of cancer returning?
The risk of cancer returning differs between cancers, and between sub-types of the same cancer.
New screening and treatment options have seen reductions in recurrence rates for many types of cancer. For example, between 2004 and 2019, the risk of colon cancer recurring dropped by 31-68%. It is important to remember that only someone’s treatment team can assess an individual’s personal risk of cancer returning.
For most types of cancer, the highest risk of cancer returning is within the first three years after entering remission. This is because any leftover cancer cells not killed by treatment are likely to start growing again sooner rather than later. Three years after entering remission, recurrence rates for most cancers decrease, meaning that every day that passes lowers the risk of the cancer returning.
Every day that passes also increases the numbers of new discoveries, and cancer drugs being developed.
What about second, unrelated cancers?
Earlier this year, we learned Sarah Ferguson, Duchess of York, had been diagnosed with malignant melanoma (a type of skin cancer) shortly after being treated for breast cancer.
Although details have not been confirmed, this is likely a new cancer that isn’t a recurrence or metastasis of the first one.
Australian research from Queensland and Tasmania shows adults who have had cancer have around a 6-36% higher risk of developing a second primary cancer compared to the risk of cancer in the general population.
Who’s at risk of another, unrelated cancer?
With improvements in cancer diagnosis and treatment, people diagnosed with cancer are living longer than ever. This means they need to consider their long-term health, including their risk of developing another unrelated cancer.
Reasons for such cancers include different types of cancers sharing the same kind of lifestyle, environmental and genetic risk factors.
The increased risk is also likely partly due to the effects that some cancer treatments and imaging procedures have on the body. However, this increased risk is relatively small when compared with the (sometimes lifesaving) benefits of these treatment and procedures.
While a 6-36% greater chance of getting a second, unrelated cancer may seem large, only around 10-12% of participants developed a second cancer in the Australian studies we mentioned. Both had a median follow-up time of around five years.
Similarly, in a large US study only about one in 12 adult cancer patients developed a second type of cancer in the follow-up period (an average of seven years).
The kind of first cancer you had also affects your risk of a second, unrelated cancer, as well as the type of second cancer you are at risk of. For example, in the two Australian studies we mentioned, the risk of a second cancer was greater for people with an initial diagnosis of head and neck cancer, or a haematological (blood) cancer.
People diagnosed with cancer as a child, adolescent or young adult also have a greater risk of a second, unrelated cancer.
What can I do to lower my risk?
Regular follow-up examinations can give peace of mind, and ensure any subsequent cancer is caught early, when there’s the best chance of successful treatment.
Maintenance therapy may be used to reduce the risk of some types of cancer returning. However, despite ongoing research, there are no specific treatments against cancer recurrence or developing a second, unrelated cancer.
But there are things you can do to help lower your general risk of cancer – not smoking, being physically active, eating well, maintaining a healthy body weight, limiting alcohol intake and being sun safe. These all reduce the chance of cancer returning and getting a second cancer.
Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, Walter and Eliza Hall Institute and Terry Boyle, Senior Lecturer in Cancer Epidemiology, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: