The Truth About Handwashing
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Washing Our Hands Of It

In Tuesdays’s newsletter, we asked you how often you wash your hands, and got the above-depicted, below-described, set of self-reported answers:
- About 54% said “More times per day than [the other options]”
- About 38% said “Whenever using the bathroom or kitchen
- About 5% said “Once or twice per day”
- Two (2) said “Only when visibly dirty”
- Two (2) said “I prefer to just use sanitizer gel”
What does the science have to say about this?
People lie about their handwashing habits: True or False?
True and False (since some people lie and some don’t), but there’s science to this too. Here’s a great study from 2021 that used various levels of confidentiality in questioning (i.e., there were ways of asking that made it either obvious or impossible to know who answered how), and found…
❝We analysed data of 1434 participants. In the direct questioning group 94.5% of the participants claimed to practice proper hand hygiene; in the indirect questioning group a significantly lower estimate of only 78.1% was observed.❞
Note: the abstract alone doesn’t make it clear how the anonymization worked (it is explained later in the paper), and it was noted as a limitation of the study that the participants may not have understood how it works well enough to have confidence in it, meaning that the 78.1% is probably also inflated, just not as much as the 94.5% in the direct questioning group.
Here’s a pop-science article that cites a collection of studies, finding such things as for example…
❝With the use of wireless devices to record how many people entered the restroom and used the pumps of the soap dispensers, researchers were able to collect data on almost 200,000 restroom trips over a three-month period.
The found that only 31% of men and 65% of women washed their hands with soap.❞
Source: Study: Men Wash Their Hands Much Less Often Than Women (And People Lie About Washing Their Hands)
Sanitizer gel does the job of washing one’s hands with soap: True or False?
False, though it’s still not a bad option for when soap and water aren’t available or practical. Here’s an educational article about the science of why this is so:
UCI Health | Soap vs. Hand Sanitizer
There’s also some consideration of lab results vs real-world results, because while in principle the alcohol gel is very good at killing most bacteria / inactivating most viruses, it can take up to 4 minutes of alcohol gel contact to do so, as in this study with flu viruses:
In contrast, 20 seconds of handwashing with soap will generally do the job.
Antibacterial soap is better than other soap: True or False?
False, because the main way that soap protects us is not in its antibacterial properties (although it does also destroy the surface membrane of some bacteria and for that matter viruses too, killing/inactivating them, respectively), but rather in how it causes pathogens to simply slide off during washing.
Here’s a study that found that handwashing with soap reduced disease incidence by 50–53%, and…
❝Incidence of disease did not differ significantly between households given plain soap compared with those given antibacterial soap.❞
Read more: Effect of handwashing on child health: a randomised controlled trial
Want to wash your hands more than you do?
There have been many studies into motivating people to wash their hands more (often with education and/or disgust-based shaming), but an effective method you can use for yourself at home is to simply buy more luxurious hand soap, and generally do what you can to make handwashing a more pleasant experience (taking a moment to let the water run warm is another good thing to do if that’s more comfortable for you).
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Hanging Exercises For Complete Beginners & Older Adults

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hanging (not the kind with a gallows) is great for the heath, improving not just strength and mobility, but also—critically—looking after spinal health too. Amanda Raynor explains in this video how this exercise is accessible to anyone (unless you have no arms, in which case, sorry, this one is just not for you—though hanging by your legs will also give similar spinal benefits!).
Hanging out
Hanging can be done at home or at a park, with minimal equipment (a bar, a sturdy tree branch, etc).
Note: the greater the diameter of the bar, the more it will work your grip strength, and/but the harder it will be. So, it’s recommend to start with a narrow-diameter bar first.
Getting started:
- Start with a “dead hang”: grip the bar with hands shoulder-width apart, thumb wrapped around.
- Aim to hang without pulling up; build endurance gradually (10–30 seconds is fine at first).
- Work up to holding for 60 seconds in three sets as a fitness goal.
Progression:
- If unable to hang at all initially, use a chair or stool to support some body weight.
- Gradually reduce foot support to increase duration of free hanging.
- Start with 10 seconds, progressing by small increments (e.g: 15, 20, 25 seconds) until reaching 60 seconds.
Advanced variations:
- Move the body while hanging (e.g., circles, knee lifts).
- Experiment with different grips (overhand, underhand) for varied muscle engagement.
- Try scapular pulls or one-arm hangs for additional challenge and strength-building.
For more on all of this plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Share This Post
-

The Dirt Cure – by Dr. Maya Shetreat-Klein
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As we discussed in our article “Stop Sabotaging Your Gut”, there is indeed merit to living a little dirty, in particular when it comes to what we put in our mouths. Having the space of an entire book rather than a small article, Dr. Shetreat-Klein expands on this in great detail.
The subtitle mentions “growing healthy kids with food straight from the soil”; it’s worth noting that all the information here (with the exception of concerning breastfeeding etc) is equally applicable to adults too—so if it’s your own health you’re focused on rather than that of kids or grandkids, then that’s fine too.
You may be wondering: what more is there to say than “don’t scrub your vegetables as though you’re about to perform surgery with them”?
There’s a lot of background information on what things help or harm our bodies in the first place, most notably via our gut, and as an important extra consideration, the gut-brain axis. Incidentally, the author is a neurologist by professional background.
Then she gets more specific, into “include and exclude” recommendations. In this matter we have one criticism: she does recommend raw milk over pasteurized, and that is, by overwhelming scientific consensus, a terrible idea. Raw milk is an abundant source of pathogens and a breeding ground for even more. There is “living dirty” and there is “living dangerously”, and drinking raw milk is the latter. See also: Pasteurization: What It Does And Doesn’t Do
However, for the most part, the rest of her advice is sound, and there’s even a recipes section too.
The style is something of a polemic throughout, but the extensive venting does not take away from there being a lot of genuine information in here too.
Bottom line: please skip the raw milk, but aside from that, if you’d like to improve your diet to improve your gut and immune health, then this book can help with that.
Share This Post
-

This Is Your Brain on Food – by Dr. Uma Naidoo
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Diet will fix your brain” is a bold claim that often comes from wishful thinking and an optimistic place where anecdote is louder than evidence. But, diet does incontrovertibly also affect brain health. So, what does Dr. Naidoo bring to the table?
The author is a Harvard-trained psychiatrist, a professional chef who graduated with her culinary school’s most coveted award, and a trained-and-certified nutritionist. Between those three qualifications, it’s safe to she knows her stuff when it comes to the niche that is nutritional psychiatry. And it shows.
She takes us through the neurochemistry involved, what chemicals are consumed, made, affected, inhibited, upregulated, etc, what passes through the blood-brain barrier and what doesn’t, what part the gut really plays in its “second brain” role, and how we can leverage that—as well as mythbusting a lot of popular misconceptions about certain foods and moods.
There’s hard science in here, but presented in quite a pop-science way, making for a very light yet informative read.
Bottom line: if you’d like to better understand what your food is doing to your brain (and what it could be doing instead), then this is a top-tier book for you!
Click here to check out This Is Your Brain On Food, and get to know yours!
Share This Post
Related Posts
-
Are Fruit & Vegetable Extract Supplements Worth It?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
At 10almonds we are always extolling the virtues of fruits and vegetables, but how much do those benefits still exist when we’re looking at a fruit and vegetable extract supplement?
We examined one aspect of this previously, here;
Mediterranean Diet… In A Pill?
This looked at getting the anti-inflammatory benefits of the Mediterranean diet, in supplement form, by providing extracts of 16 key plant extracts—which also provides an excellent shopping list, by the way, if you just want to skip the supplements and buy those plants; if nine top scientists (anti-aging specialists, neurobiologists, pharmacologists, and at least one professor of applied statistics) came to the conclusion that to get the absolute most bang-for-buck possible, those are the plants to get the phytochemicals from, then we’re not going to ignore that!
And yes, the short answer was “it does very significantly improve anti-inflammatory markers”, by the way.
But when it comes to benefits from polyphenols, anti-inflammatory powers are very much “low-hanging fruit”, so to speak. It’s the “fork found in kitchen” level of shocking revelation. It’s what polyphenols are best at (tied with antioxidant powers, which directly mediate their anti-inflammatory powers).
So, what about something more challenging, like brain benefits?
Underrated Brain Boosters
A European research team (Dr. Begoña Cerdá et al.) looked at the effects of polyphenol-rich nutraceuticals (plant extracts) on cognitive function and neuroprotection biomarkers.
It was a randomized, crossover, double-blind, sex-stratified, placebo-controlled clinical trial that had people take the supplement or a placebo for 16 weeks, have a 4-week washout phase (to minimize leftover effects contaminating the data) and then switching groups (still blinded to the placebo control) for 16 weeks.
They tested cognitive function and neuroprotection biomarkers in various ways before and after each of the testing phases (so, four testing sessions in total per person: before and after the supplement + before and after the placebo).
The results:
❝The results suggested that participants who consumed the polyphenol-rich nutraceutical demonstrated significant improvements in cognitive performance compared to the placebo group.
The Stroop Test scores indicated enhanced attention and inhibitory control, while RIST results suggested improvements in logical reasoning and memory. The Trail Making Test also revealed increased cognitive flexibility, highlighting the supplement’s potential to boost overall mental agility.
Furthermore, the ELISA results showed a notable increase in BDNF and CREB levels among participants who took the active supplement. BDNF is a protein that is essential for neuronal growth and survival, and its levels were significantly elevated, reinforcing its role in synaptic plasticity and long-term memory formation.
Additionally, CREB, a transcription factor involved in learning processes, also showed increased levels, supporting its function in cognitive enhancement.
Importantly, the correlation between improved test scores and higher biomarker levels suggested that polyphenols may directly influence brain function rather than merely offering general health benefits.
While the study focused on healthy adults, the findings also raised questions about whether similar interventions could benefit populations at risk for cognitive decline, including older adults and individuals with neurodegenerative conditions.❞
Key to abbreviations:
- RIST = Reynolds Intellectual Screening Test
- ELISA = Enzyme-Linked ImmunoSorbent Assays
- BDNF = Brain-Derived Neurotrophic Factor
- CREB = cAMP-Response Element Binding Protein
- cAMP = Cyclic Adenosine MonoPhosphate
Source: Daily fruit and vegetable extracts may boost brain power ← we quoted a pop-sci article for the above summary, for easier readability while still having the critical conclusions in one place
For those who do want to dive into the actual data and a lot more detail about the study methodology (which is well worth reading if you have the time, as it’s very good), here is the actual study:
If nothing else, be aware that the usual benchmark for statistical significance is p < 0.05, whereas the results in this study ranged from p < 0.01 to p < 0.001, in other words, ranging from 5x more significant than is required to be called “significant”, to 50x more significant than is required to be called “significant”.
In fewer words: impressively significant
In lay terms: the scientists are about as sure as scientists ever get about anything, that this supplement produces significant results
What was the supplement they tested?
Good news! It was…
- a commercially available supplement (JuicePlus), which is convenient, because it means we (and you, dear reader) can get it if we so choose
- not paid for by JuicePlus or anyone associated with them (indeed, the funding declaration on the study is “This research received no external funding”), so not subject to any conflict of interest that might introduce bias into the study
As for why they chose that one:
❝A unique aspect of the polyphenol-rich nutraceutical evaluated in this study lies in its composition, which integrates a blend of fruit, vegetable, and berry juice powders.
This product, Juice Plus+ Premium®, contains over 119 distinct polyphenolic compounds, including flavanols, anthocyanins, and flavones, as demonstrated in prior compositional analyses.
Compared to other polyphenol-based interventions, this nutraceutical stands out due to its comprehensive formulation, combining a wide range of bioactive compounds with complementary antioxidant and neuroprotective effects.
These characteristics ensure a more diverse interaction with neurobiological pathways, including those related to oxidative stress mitigation, synaptic plasticity, and cognitive function❞
Source: Ibid. (it’s in the introduction)
Want to try some?
We don’t sell it, but for your convenience, here’s where to get JuicePlus supplements Amazon 😎
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
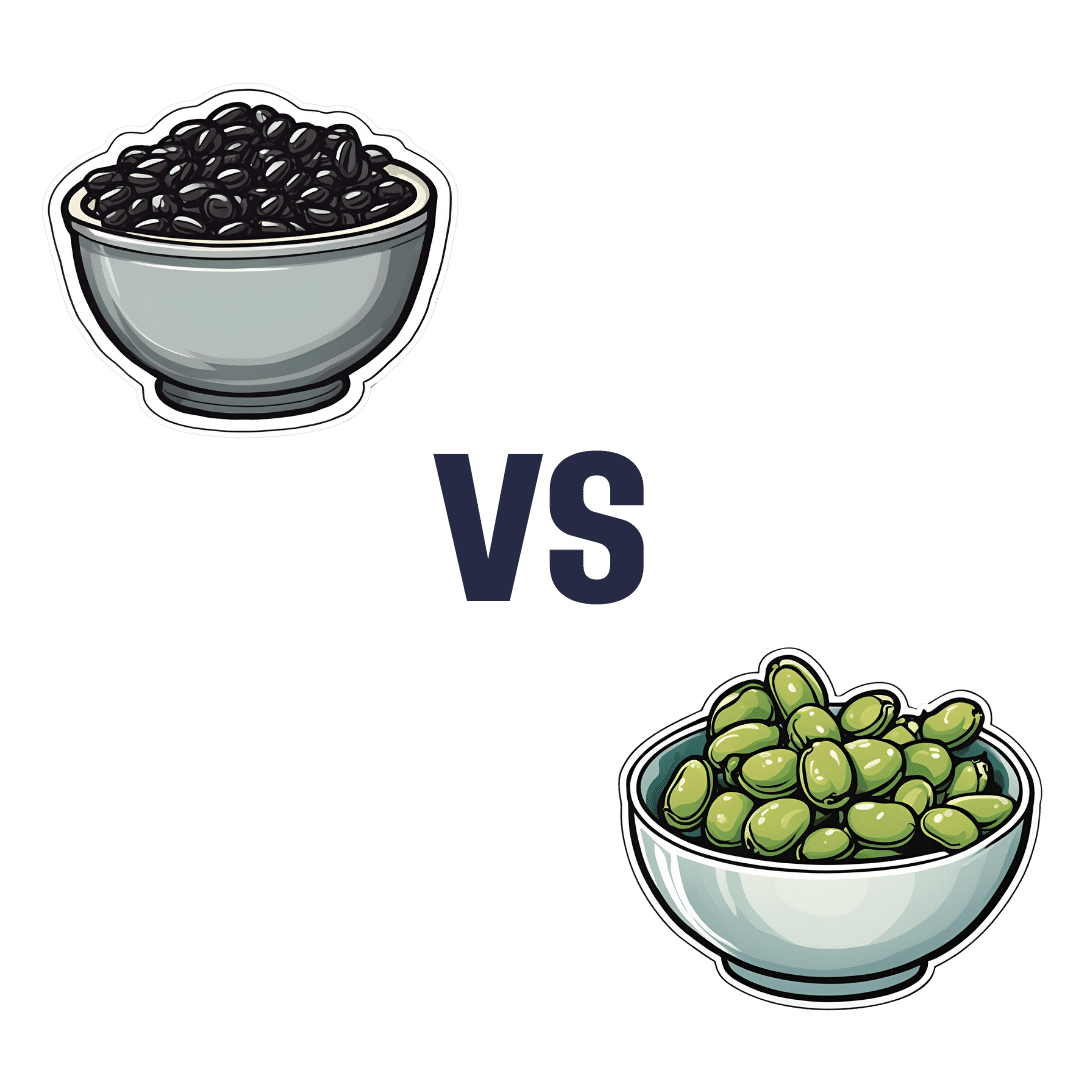
Black Beans vs Fava Beans – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing black beans to fava beans, we picked the black beans.
Why?
In terms of macros, black beans have more protein, carbs, and notably more fiber, the ratio of the latter two also being such that black beans enjoy the lower glycemic index (but both are still good). All in all, a clear win for black beans in this category.
In the category of vitamins, black beans have more of vitamins B1, B5, B6, E, K, and choline, while fava beans have more of vitamins A, B2, B3, B9, and C. That’s a marginal 6:5 win for black beans, before we take into account that they also have 43x as much vitamin E, which is quite a margin, while fava beans doesn’t have any similarly stand-out nutrient. So, another clear win for black beans.
When it comes to minerals, black beans have more calcium, copper, iron, magnesium, phosphorus, and potassium, while fava beans have more manganese, selenium, and zinc. Superficially this is a 6:3 win for black beans; it’s worth noting however that the margins aren’t high on either side in the case of any mineral, so this one’s closer than it looks. Still a win for black beans, though.
Adding up the sections makes for an easy overall win for black beans, but by all means, enjoy either or both—diversity is good!
Want to learn more?
You might like to read:
Eat More (Of This) For Lower Blood Pressure
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How we can prepare for future public health emergencies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The U.S. is experiencing an increasing number of disease outbreaks and extreme weather events. While state and national preparedness for public health emergencies has improved in some areas, dangerous gaps remain, says a recent report from Trust for America’s Health.
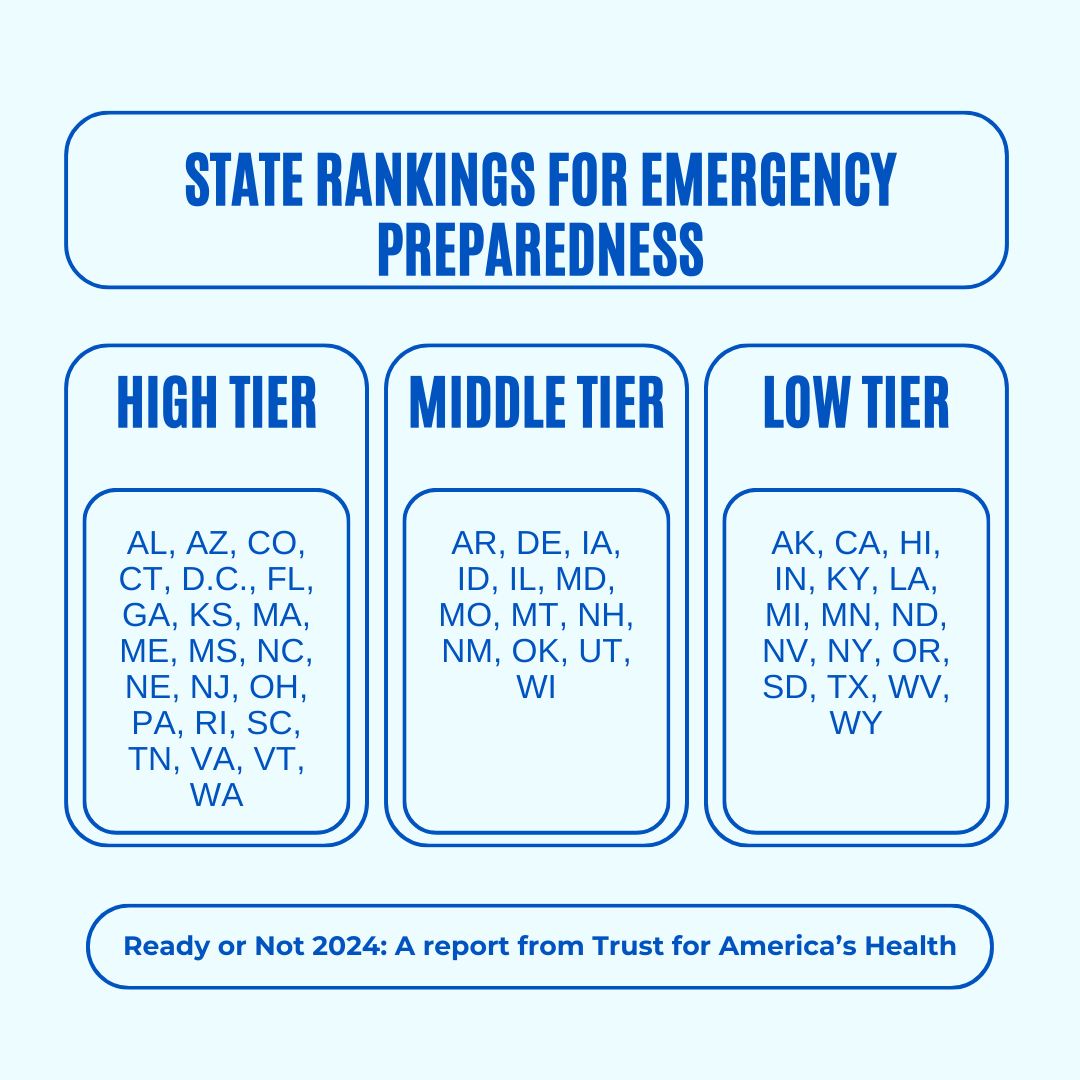
Titled, “Ready or Not 2024: Protecting the Public’s Health from Diseases, Disasters, and Bioterrorism,” the report identifies gaps in national and state preparedness for public health emergencies and provides recommendations for improvement.
Using nine key indicators, the report categorizes all U.S. states and the District of Columbia into three readiness levels: high, medium, and low. The writers hope the report will help policymakers in under-performing states improve public health infrastructure.
Read on to learn more about what the research found and how we can individually prepare for future public health emergencies.
There’s work to be done

The report highlights areas with strong performance as well as those that need improvement.
Some areas with strong performance:
- State public health funding: Most states and the District of Columbia either maintained or increased their public health funding during the 2023 fiscal year.
- Health care labor force preparedness: Most states have started expanding the health care labor force for improved emergency response. As of 2023, 39 states participated in the Nurse Licensure Compact, which allows nurses to work in multiple member states without the need for additional state licenses.
Some areas that need improvement:
- Hospital safety scores: Only 25 percent of acute care hospitals earned the highest patient safety grade in fall 2023. These scores measure health care-associated infection rates, intensive care unit capacity, and other metrics. More high-scoring hospitals would improve preparedness for future public health emergencies.
- Access to paid time off: From March 2018 to March 2023, only 55 percent of U.S. workers used paid time off. Access to paid time off is important for reducing the spread of infectious diseases.
We can all do our part by staying up to date on vaccines
While the report focuses on policy changes that would improve emergency preparedness, Trust for America’s Health’s research identifies one way that we can individually prepare for future public health emergencies: staying up to date on vaccines.
The report found that during the 2022-2023 flu season, only 49 percent of those eligible for the flu vaccine received it. Public health experts are concerned that false claims about COVID-19 vaccines have resulted in overall vaccine hesitancy.
A decline in vaccination rates has led to an uptick in life-threatening, vaccine-preventable diseases, such as measles. Increasing vaccine uptake would prevent the spread of vaccine-preventable diseases and reduce strain on hospital systems during public health crises.
Make sure that you and your children have received all recommended vaccines to prevent severe illness, hospitalization, and death. Learn more about recommended vaccines for adults and children from the CDC.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: