The 5 Love Languages Gone Wrong
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Levelling up the 5 love languages
The saying “happy wife; happy life” certainly goes regardless of gender, and if we’re partnered, it’s difficult to thrive in our individual lives if we’re not thriving as a couple. So, with the usual note that mental health is also just health, let’s take a look at getting beyond the basics of a well-known, often clumsily-applied model:
The 5 love languages
You’re probably familiar with “the 5 love languages”, as developed by Dr. Gary Chapman. If not, they are:
- Acts of Service
- Gift-Giving
- Physical Touch
- Quality Time
- Words of Affirmation
The idea is that we each weight these differently, and problems can arise when a couple are “speaking a different language”.
So, is this a basic compatibility test?
It doesn’t have to be!
We can, if we’re aware of each other’s primary love languages, make an effort to do a thing we wouldn’t necessarily do automatically, to ensure they’re loved the way they need to be.
But…
What a lot of people overlook is that we can also have different primary love languages for giving and for receiving. And, missing that can mean that even taking each other’s primarily love languages into account, efforts to make a partner feel loved, or to feel loved oneself, can miss 50% of the time.
For example, I (your writer here today, hi) could be asked my primary love language and respond without hesitation “Acts of Service!” because that’s my go-to for expressing love.
I’m the person who’ll run around bringing drinks, do all the housework, and without being indelicate, will tend towards giving in the bedroom. But…
A partner trying to act on that information to make me feel loved by giving Acts of Service would be doomed to catastrophic failure, because my knee-jerk reaction would be “No, here, let me do that for you!”
So it’s important for partners to ask each other…
- Not: “what’s your primary love language?” ❌
- But: “what’s your primary way of expressing love?” ✅
- And: “which love language makes you feel most loved?” ✅
For what it’s worth, I thrive on Words of Affirmation, so thanks again to everyone who leaves kind feedback on our articles! It lets me know I provided a good Act of Service
So far, so simple, right? You and your partner (or: other person! Because as we’ve just seen, these go for all kinds of dynamics, not just romantic partnerships) need to be aware of each other’s preferred love languages for giving and receiving.
But…
There’s another pitfall that many fall into, and that’s assuming that the other person has the same idea about what a given love language means, when there’s more to clarify.
For example:
- Acts of Service: is it more important that the service be useful, or that it took effort?
- Gift-Giving: is it better that a gift be more expensive, or more thoughtful and personal?
- Physical Touch: what counts here? If we’re shoulder-to-shoulder on the couch, is that physical touch or is something more active needed?
- Quality Time: does it count if we’re both doing our own thing but together in the same room, comfortable in silence together? Or does it need to be a more active and involved activity together? And is it quality time if we’re at a social event together, or does it need to be just us?
- Words of Affirmation: what, exactly, do we need to hear? For romantic partners, “I love you” can often be important, but is there something else we need to hear? Perhaps a “because…”, or perhaps a “so much that…”, or perhaps something else entirely? Does it no longer count if we have to put the words in our partner’s mouth, or is that just good two-way communication?
Bottom line:
There’s a lot more to this than a “What’s your love language?” click-through quiz, but with a little application and good communication, this model can really resolve a lot of would-be problems that can grow from feeling unappreciated or such. And, the same principles go just the same for friends and others as they do for romantic partners.
In short, it’s one of the keys to good interpersonal relationships in general—something critical for our overall well-being!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Plum vs Nectarine – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing plums to nectarines, we picked the nectarines.
Why?
Both are great! But nectarines win at least marginally in each category we look at.
In terms of macros, plums have more carbs while nectarines have more fiber, resulting of course in a lower glycemic index. Plums do have a low GI also; just, nectarines have it better.
When it comes to vitamins, plums have more of vitamins A, B6, C, and K, while nectarines have more of vitamins B1, B2, B3, B5, E, and choline.
In the category of minerals, plums are great but not higher in any mineral than nectarines; nectarines meanwhile have more copper, iron, magnesium, manganese, phosphorus, potassium, and zinc.
All in all, enjoy both. And if having dried fruit, then prunes (dried plums) are generally more widely available than dried nectarines. But if you’re choosing one fruit or the other, nectarine is the way to go.
Want to learn more?
You might like to read:
- Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
- Replacing Sugar: Top 10 Anti-Inflammatory Sweet Foods
- Top 8 Fruits That Prevent & Kill Cancer
Take care!
Share This Post
-
The FDA Just Redefined “Healthy”—But How?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In the ongoing war of labelling regulations (usually with advertisers on one side and regulators on the other), the FDA has updated what’s required in order to label a food as “healthy”.
Here’s what they’re now* requiring:
To bear the “healthy” claim, a food product needs to:
- Contain a certain amount of food (food group equivalent) from at least one of the food groups or subgroups (such as fruits, vegetables, fat-free and low-fat dairy etc.) recommended by the Dietary Guidelines.
- Adhere to specified limits for the following nutrients: saturated fat, sodium, and added sugars.
Source: FDA | Press Releases | FDA Finalizes Updated “Healthy” Nutrient Content Claim
*however, manufacturers have 3 years to conform, which if we’re being cynical about it, looks suspiciously like just short of a US presidential election cycle so that actual enforcement will be someone else’s problem.
Will it help?
Maybe! It’s not too dissimilar to the “traffic light system” already in use in Europe, although that currently emphasizes the absence/presence of “bad things” e.g. saturated fat, sodium, and added sugars.
It has its faults, because for example…
- not all saturated fat is bad, and a jar of coconut oil is now definitely going to get labelled as very unhealthy
- low-sodium salt is, ironically, going to to get flagged as being very high in sodium and therefore unhealthy
This latter is because on a g/100g basis, a product that’s ⅓ sodium chloride is going to have a lot of sodium, even if it’s approaching ⅔ less sodium than the product it’s (healthily!) replacing.
However, on a large scale, these kinds of problems are surely going to be small next to (hopefully) manufacturers scrambling to find ways to cut down on the saturated fats, sodium, and added sugars.
You may be wondering…
What will they replace them with?
Sometimes, companies trying to make something healthier will mess up, like when the health risks of smoking hit public consciousness, one cigarette company had the bright idea of putting asbestos in their filter tips, to market them as healthier. So, could something similar happen here?
- Saturated fat: definitely could; because the health benefits/risks of different kinds of fats and their constituent fatty acids are a lot more nuanced than just “saturated” vs “mono-/polyunsaturated”, it is definitely possible that companies may replace healthier saturated-heavy fats with less healthy unsaturated fats, depending on what is cheaper.
- See also: Can Saturated Fats Be Healthy?
- Sodium: probably not; likely go-to replacements for sodium chloride will be potassium chloride (healthier than sodium chloride) and MSG (has an unearned bad reputation in the US, but is healthier than sodium chloride).
- Added sugars: probably—things get very complicated very quickly when it comes to artificial sweeteners, and also the crux will definitely lie in what gets defined as an “added sugar”; watch out for a rise in the use of things that slide by the definition of added sugar while still being chemically (and, which is important, metabolically) the same thing.
Well that doesn’t sound great
It doesn’t, but on the flipside, the positive inclusions will probably be mostly good.
For example, the only way to get a “healthy” labelling in including fiber is to include more fiber, same with vitamins and minerals.
The low-fat dairy thing could possibly get abused (much like with the general “low-fat” trend of the 80s).
The “portion of fruit” thing will need to be carefully defined to avoid running straight back into the “this is just added sugar by another name” problem; mostly that it’ll need to still include the same amount of fiber as was in the whole fruit, gram for gram.
See also: What Matters Most For Your Heart? ← it’s about fiber, not salt or saturated fats!
Take care!
Share This Post
-
Passion Fruit vs Blueberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing passion fruit to blueberries, we picked the passion fruit.
Why?
It wasn’t close!
In terms of macros, the passion fruit has 3x the protein, 1.5x the carbs, and more than 4x the fiber. An easy win for passion fruit!
In the category of vitamins, passion fruit has more of vitamins A, B2, B3, B5, B6, B7, B9, C, and choline, while blueberries have more of vitamins B1, E, and K. So, blueberries are not without their merits, but all in all, another win for passion fruit here.
When it comes to minerals, passion fruit has more calcium, copper, iron, magnesium, manganese, phosphorus, potassium, and selenium, while blueberries have slightly more zinc.
Looking at polyphenols, this is one category where blueberry wins, and by a fair margin. We think that’s a great reason to enjoy blueberries, but not enough to reverse the win for passion fruit based on all the other categories!
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Enjoy!
Share This Post
Related Posts
-

7 Steps to Get Off Sugar and Carbohydrates – by Susan Neal
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We will not keep the steps a mystery; abbreviated, they are:
- decide to really do this thing
- get knowledge and support
- clean out that pantry/fridge/etc and put those things behind you
- buy in healthy foods while starving your candida
- plan for an official start date, so that everything is ready
- change the way you eat (prep methods, timings, etc)
- keep on finding small ways to improve, without turning back
Particularly important amongst those are starving the candida (the fungus in your gut that is responsible for a lot of carb cravings, especially sugar and alcohol—which latter can be broken down easily into sugar), and changing the “how” of eating as well as the “what”; those are both things that are often overlooked in a lot of guides, but this one delivers well.
Walking the reader by the hand through things like that is probably the book’s greatest strength.
In the category of subjective criticism, the author does go off-piste a little at the end, to take a moment while she has our attention to talk about other things.
For example, you may not need “Appendix 7: How to Become A Christian and Disciple of Jesus Christ”.
Of course if that calls to you, then by all means, follow your heart, but it certainly isn’t a necessary step of quitting sugar. Nevertheless, the diversion doesn’t detract from the good dietary change advice that she has just spent a book delivering.
Bottom line: there’s no deep science here, but there’s a lot of very good, very practical advice, that’s consistent with good science.
Click here to check out 7 Steps to Get Off Sugar, and watch your health improve!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Fatigue? Unexplained weight gain and dry skin? Could it be Hashimoto’s disease?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Maybe you feel worn out. Perhaps you’re also having trouble losing weight. Generally, you just don’t feel 100%.
Could it be Hashimoto’s disease? This common autoimmune thyroid disorder is when your immune system (which fights off viruses and bacteria), mistakenly attacks a part of your body. In this case, it’s your thyroid – a gland located at the base of your neck – and can cause low thyroid hormones levels (hypothyroidism).
Hypothyroidism affects one in 33 Australians and Hashimoto’s is one of the most common thyroid conditions in first-world countries.
While symptoms can be subtle, untreated Hashimoto’s can cause long-term problems with your heart, memory and fertility. Here is what you need to know.
What happens when you have Hashimoto’s?
Your thyroid gland is a butterfly-shaped gland in the neck. It is essential in regulating things like muscle function, digestion, metabolism, the heart and lungs. In children, thyroid hormones are also needed for normal growth and development.
Hashimoto’s thyroid disease, named after the Japanese doctor who discovered it in 1912, is also known as Hashimoto’s thyroiditis or chronic lymphocytic thyroiditis. The disease can cause the immune system to mistakenly produce proteins called antibodies (thyroid peroxidase and thyroglobulin). These can cause inflammation and long-term damage to the thyroid gland. Over time, as thyroid tissue is inflamed and/or destroyed, there can be a decrease in the production of thyroid hormones (hypothyroidism).
Hashimoto’s can present subtly at first. If you only have antibodies with no change in thyroid levels, it is likely you won’t have any symptoms.
However, as the disease progresses, you may experience fatigue, weight gain (or difficulty losing weight), increased sensitivity to the cold, constipation, dry skin, muscle aches, irregular or heavy menstrual cycles, enlarged thyroid (goitre) and occasionally hair loss, including at the ends of your eyebrows.
What causes Hashimoto’s thyroid disease?
Several risk factors can contribute to the development of Hashimoto’s including:
-
genetic risk – your risk is higher if you have family members with Hashimoto’s
-
gender – women are up to ten times more likely than men to develop the disease
-
age – you are more likely to develop the disease from 30 to 50 years of age
-
autoimmune condition – having another autoimmune condition like systemic lupus, Type 1 diabetes and celiac disease increases your risk
-
excessive iodine intake and radiation exposure may also increase risk in people who are already genetically at greater risk.
What are the long-term risks?
Long-term, untreated Hashimoto’s thyroiditis can cause heart issues, higher cholesterol levels, nerve damage (peripheral neuropathy), reduced cognition and infertility.
In pregnancy, Hashimoto’s has a higher risk of pre-eclampsia (high blood pressure affecting several organs), premature birth, placental abruption (when the placenta separates from the inner wall of the uterus before birth) and, in severe cases, pregnancy loss.
The disease has also been linked with an increased risk (but low incidence) of the lymphocytes of the thyroid turning into cancer cells to cause thyroid lymphoma.
How is Hashimoto’s diagnosed?
Diagnosis can be confirmed with a blood test to check thyroid levels and antibodies.
Thyroid peroxidase antibodies are commonly present but about 5% of patients test antibody-negative. In those people, diagnosis depends on the thyroid levels, clinical presentation and ultrasound appearance of general inflammation. An ultrasound may not be required though, especially if the diagnosis is obvious.
Three hormone levels are tested to determine if you have Hashimoto’s.
Thyroid stimulating hormone (TSH) is produced by the brain to speak to the thyroid, telling it to produce two types of thyroid hormones – T3 and T4.
If you have either relative or absolute thyroid hormone deficiency, a test will show the stimulating hormones as high because the brain is trying to get the thyroid to work harder.

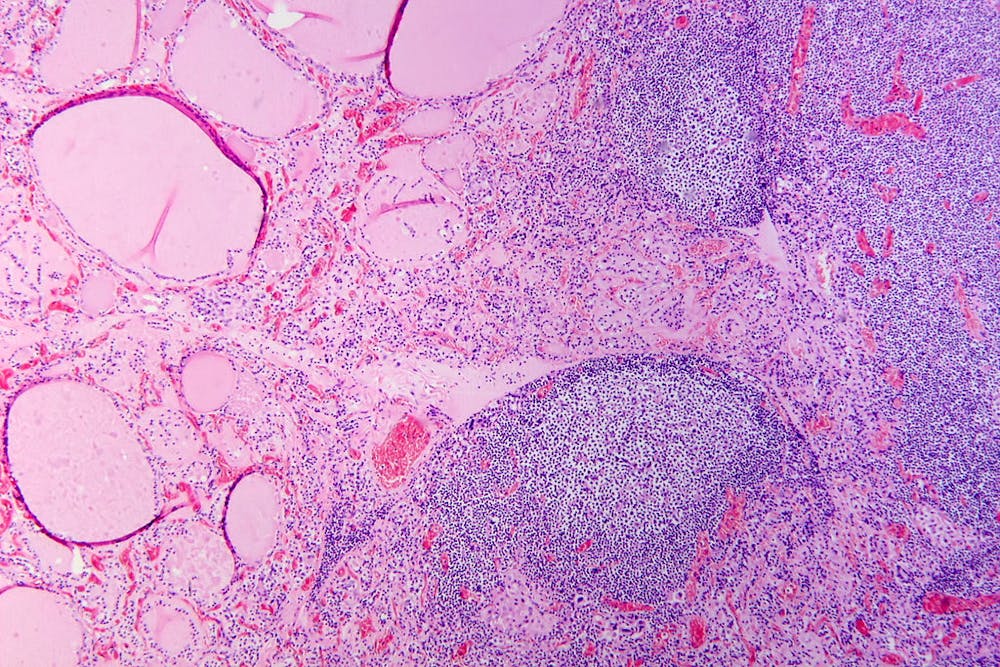
Hashimoto’s thyroiditis under the microscope. Antibodies against thyroid peroxidase and thyroglobulin were elevated.
Patho/Wikimedia Commons, CC BY-SACan it be treated?
The management of Hashimoto’s depends on the severity of the thyroid levels. Up to 20% of the population can have antibodies but normal thyroid levels. This is still Hashimoto’s thyroid disease, but it is very mild and does not require treatment. There is no current treatment to reduce antibody levels alone.
Because thyroid peroxidase antibodies increase the risk of abnormal thyroid levels in the future, regular thyroid testing is recommended.
When the thyroid stimulating hormone is high with normal thyroid hormone levels it is termed “subclinical hypothyroidism”. When it is paired with low hormone levels it is called “overt hypothyroidism”. The first is a mild form of the disease and treatment depends on the degree of stimulating hormone elevation.
Overt hypothyroidism warrants treatment. The main form of this is thyroid hormone replacement therapy (levothyroxine) with the dose of the drug adjusted until thyroid levels are within the normal range. This is usually a lifelong treatment but, once the dose is optimised, hormone levels usually remain relatively stable.
In some people with very enlarged thyroid glands causing compressive symptoms (such as difficulty swallowing or breathing), thyroidectomy (surgical removal of the thyroid) is considered.
Hashimoto’s thyroiditis is a common condition caused by your body’s immune system incorrectly damaging to your thyroid and can go undetected. Long-term, untreated, it can cause issues with your heart, cognition, and fertility. It can be diagnosed with a simple blood test. Speak to your doctor if you have any concerns as early diagnosis and treatment can help prevent complications.

Aakansha Zala, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
-

How to Think More Effectively – by Alain de Botton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our brain is our most powerful organ, and our mind is an astonishing thing. So why do we sometimes go off-piste?
The School of Life‘s Alain de Botton lays out for us a framework of cumulative thinking, directions for effort, and unlikely tools for cognitive improvement.
The book especially highlights the importance of such things as…
- making time for cumulative thinking
- not, however, trying to force it
- working with, rather than in spite of, distractions
- noting and making use of our irrationalities
- taking what we think/do both seriously and lightly, at once
- practising constructive self-doubt
The style is as clear and easy as you may have come to expect from Alain de Botton / The School of Life, and yet, its ideas are still likely to challenge every reader in some (good!) way.
Bottom line: if you would like what you think, say, do to be more meaningful, this book will help you to make the most of your abilities!
Click here to check out How To Think More Effectively, and upgrade your thought processes!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: