Cure – by Dr. Jo Marchant
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The subtitle here, “a journey into the science of mind over body”, prompts an immediate question: is this book actually about science?
And yes, yes it is. It’s not about “positive energy” or “tapping into your divine essence” or anysuch. It’s about science, and scientific studies.
The author’s PhD is in genetics and medical microbiology, not metaphysics or something.
For those of us who read a lot of clinical studies about a lot of things (hi, regular researcher/writer here), we’re very used to placebo being used as a control in medical science.
“This drug performed no better than placebo” is generally considered a disappointing statement… But what if the placebo was already having a profound effect? Shouldn’t that be worthy of note too?
Dr. Marchant looks at more than just drugs, though, and also looks into the science (complete with EEGs and such) of hypnosis and virtual reality.
The writing style here is very accessible without skimping on science. This is to be expected; Dr. Marchant also has an MSc in science communication, and spent a time as senior editor of New Scientist magazine.
This isn’t a how-to book, but there are some practical takeaways too, specific things we can do to augment (or avoid sabotaging) any medications we take, for example.
Bottom line: placebo effect (and its evil twin, the nocebo effect) has a profound impact on all of us whether we want it or not, so we might as well learn about how it works and how to leverage it. This book gives a very good, hard science grounding.
Click here to check out “Cure” and get the most out of whatever you take (or do) for your health!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A short history of sunscreen, from basting like a chook to preventing skin cancer

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australians have used commercial creams, lotions or gels to manage our skin’s sun exposure for nearly a century.
But why we do it, the preparations themselves, and whether they work, has changed over time.
In this short history of sunscreen in Australia, we look at how we’ve slathered, slopped and spritzed our skin for sometimes surprising reasons.
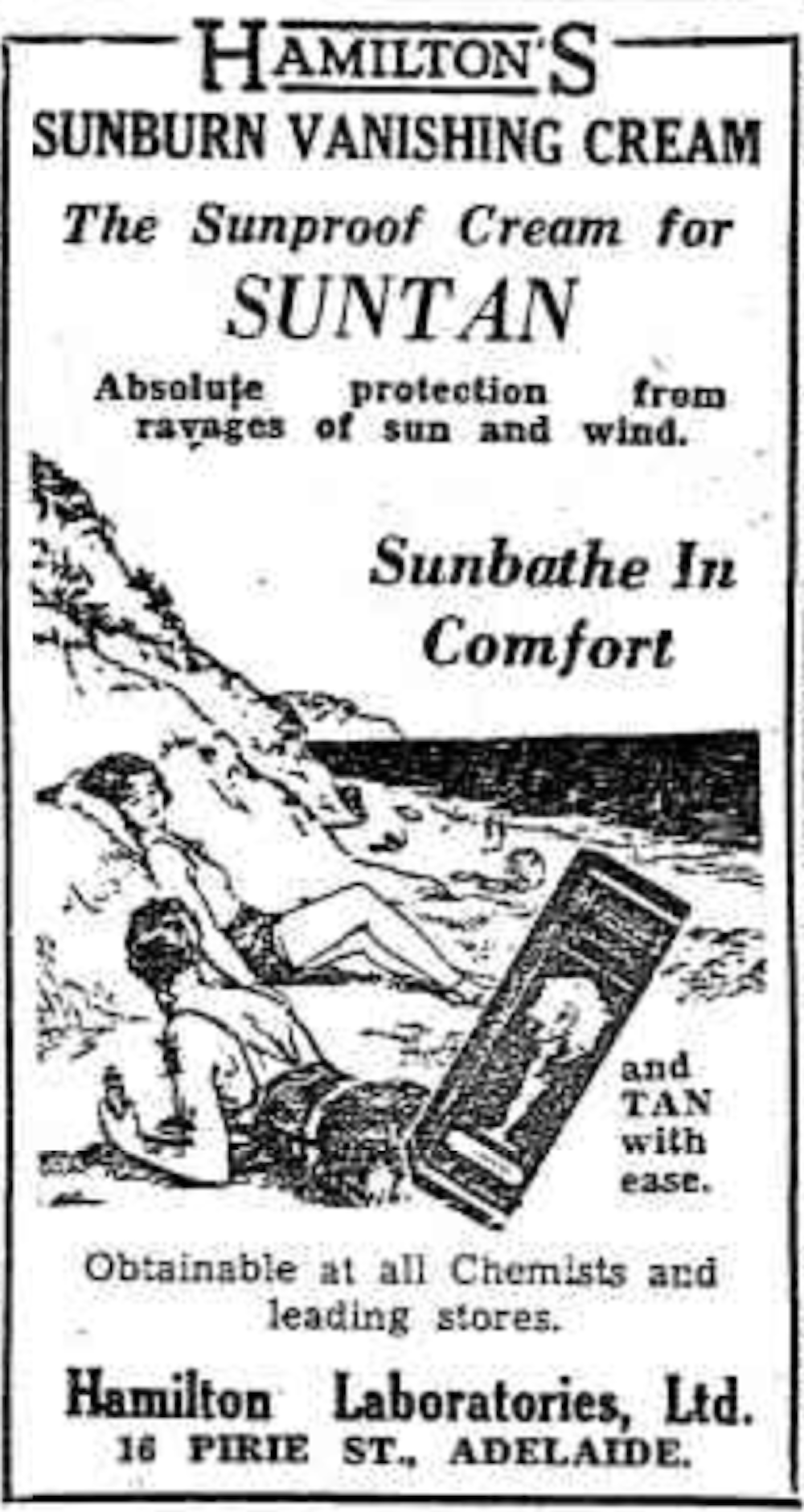
At first, suncreams helped you ‘tan with ease’

This early sunscreen claimed you could ‘tan with ease’.
Trove/NLASunscreens have been available in Australia since the 30s. Chemist Milton Blake made one of the first.
He used a kerosene heater to cook batches of “sunburn vanishing cream”, scented with French perfume.
His backyard business became H.A. Milton (Hamilton) Laboratories, which still makes sunscreens today.
Hamilton’s first cream claimed you could “
Sunbathe in Comfort and TAN with ease”. According to modern standards, it would have had an SPF (or sun protection factor) of 2.The mirage of ‘safe tanning’
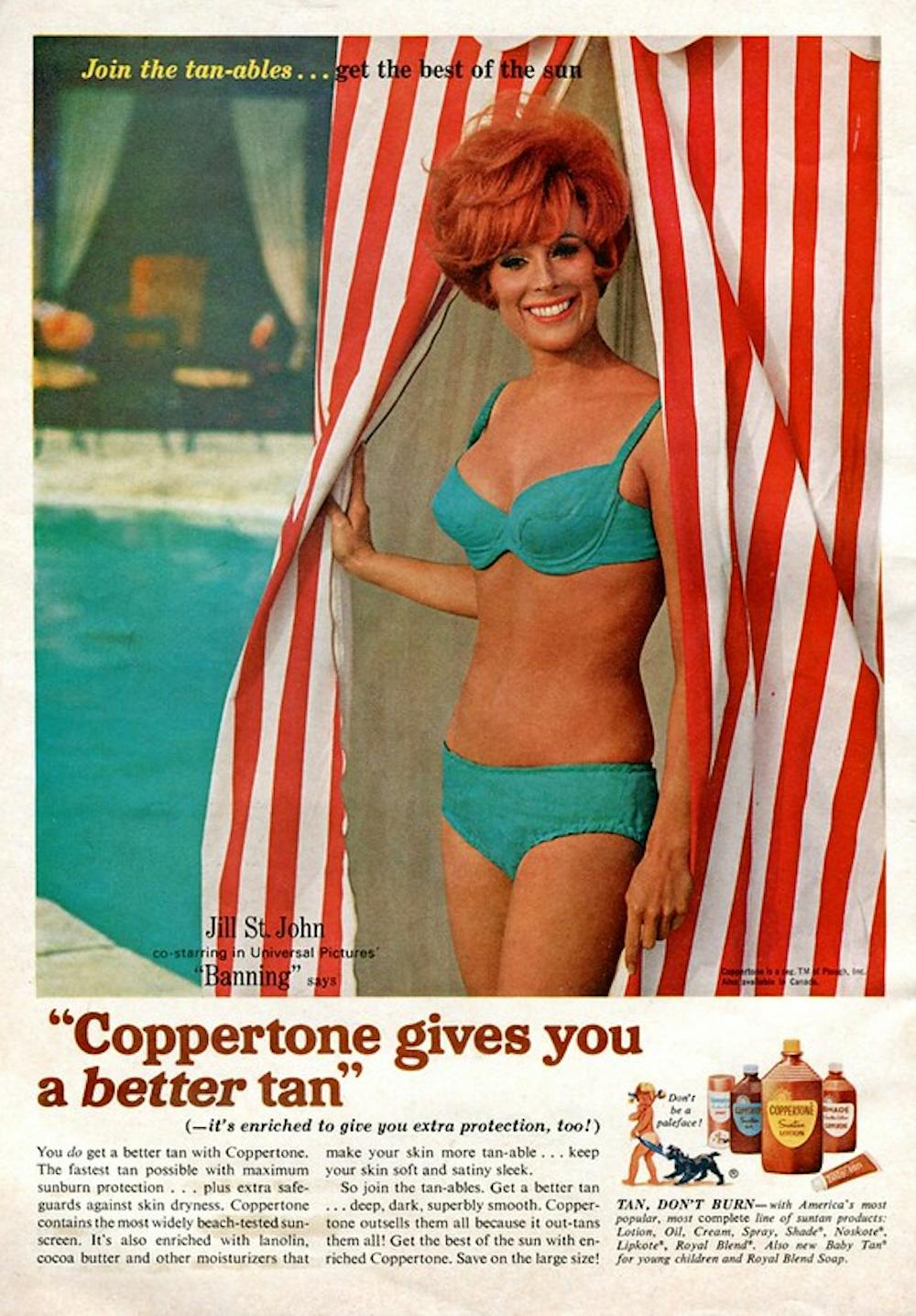
A tan was considered a “modern complexion” and for most of the 20th century, you might put something on your skin to help gain one. That’s when “safe tanning” (without burning) was thought possible.

This 1967 Coppertone advertisement urged you to ‘tan, not burn’.
SenseiAlan/Flickr, CC BY-SASunburn was known to be caused by the UVB component of ultraviolet (UV) light. UVA, however, was thought not to be involved in burning; it was just thought to darken the skin pigment melanin. So, medical authorities advised that by using a sunscreen that filtered out UVB, you could “safely tan” without burning.
But that was wrong.
From the 70s, medical research suggested UVA penetrated damagingly deep into the skin, causing ageing effects such as sunspots and wrinkles. And both UVA and UVB could cause skin cancer.
Sunscreens from the 80s sought to be “broad spectrum” – they filtered both UVB and UVA.
Researchers consequently recommended sunscreens for all skin tones, including for preventing sun damage in people with dark skin.
Delaying burning … or encouraging it?
Up to the 80s, sun preparations ranged from something that claimed to delay burning, to preparations that actively encouraged it to get that desirable tan – think, baby oil or coconut oil. Sun-worshippers even raided the kitchen cabinet, slicking olive oil on their skin.
One manufacturer’s “sun lotion” might effectively filter UVB; another’s merely basted you like a roast chicken.
Since labelling laws before the 80s didn’t require manufacturers to list the ingredients, it was often hard for consumers to tell which was which.
At last, SPF arrives to guide consumers
In the 70s, two Queensland researchers, Gordon Groves and Don Robertson, developed tests for sunscreens – sometimes experimenting on students or colleagues. They printed their ranking in the newspaper, which the public could use to choose a product.
An Australian sunscreen manufacturer then asked the federal health department to regulate the industry. The company wanted standard definitions to market their products, backed up by consistent lab testing methods.
In 1986, after years of consultation with manufacturers, researchers and consumers, Australian Standard AS2604 gave a specified a testing method, based on the Queensland researchers’ work. We also had a way of expressing how well sunscreens worked – the sun protection factor or SPF.
This is the ratio of how long it takes a fair-skinned person to burn using the product compared with how long it takes to burn without it. So a cream that protects the skin sufficiently so it takes 40 minutes to burn instead of 20 minutes has an SPF of 2.
Manufacturers liked SPF because businesses that invested in clever chemistry could distinguish themselves in marketing. Consumers liked SPF because it was easy to understand – the higher the number, the better the protection.
Australians, encouraged from 1981 by the Slip! Slop! Slap! nationwide skin cancer campaign, could now “slop” on a sunscreen knowing the degree of protection it offered.
How about skin cancer?
It wasn’t until 1999 that research proved that using sunscreen prevents skin cancer. Again, we have Queensland to thank, specifically the residents of Nambour. They took part in a trial for nearly five years, carried out by a research team led by Adele Green of the Queensland Institute of Medical Research. Using sunscreen daily over that time reduced rates of squamous cell carcinoma (a common form of skin cancer) by about 60%.
Follow-up studies in 2011 and 2013 showed regular sunscreen use almost halved the rate of melanoma and slowed skin ageing. But there was no impact on rates of basal cell carcinoma, another common skin cancer.
By then, researchers had shown sunscreen stopped sunburn, and stopping sunburn would prevent at least some types of skin cancer.
What’s in sunscreen today?
An effective sunscreen uses one or more active ingredients in a cream, lotion or gel. The active ingredient either works:
-
“chemically” by absorbing UV and converting it to heat. Examples include PABA (para-aminobenzoic acid) and benzyl salicylate, or
-
“physically” by blocking the UV, such as zinc oxide or titanium dioxide.
Physical blockers at first had limited cosmetic appeal because they were opaque pastes. (Think cricketers with zinc smeared on their noses.)
With microfine particle technology from the 90s, sunscreen manufacturers could then use a combination of chemical absorbers and physical blockers to achieve high degrees of sun protection in a cosmetically acceptable formulation.
Where now?
Australians have embraced sunscreen, but they still don’t apply enough or reapply often enough.
Although some people are concerned sunscreen will block the skin’s ability to make vitamin D this is unlikely. That’s because even SPF50 sunscreen doesn’t filter out all UVB.
There’s also concern about the active ingredients in sunscreen getting into the environment and whether their absorption by our bodies is a problem.
Sunscreens have evolved from something that at best offered mild protection to effective, easy-to-use products that stave off the harmful effects of UV. They’ve evolved from something only people with fair skin used to a product for anyone.
Remember, slopping on sunscreen is just one part of sun protection. Don’t forget to also slip (protective clothing), slap (hat), seek (shade) and slide (sunglasses).

Laura Dawes, Research Fellow in Medico-Legal History, Australian National University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
-

Coughing/Wheezing After Dinner?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The After-Dinner Activities You Don’t Want
A quick note first: our usual medical/legal disclaimer applies here, and we are not here to diagnose you or treat you; we are not doctors, let alone your doctors. Do see yours if you have any reason to believe there may be cause for concern.
Coughing and/or wheezing after eating is more common the younger or older someone is. Lest that seem contradictory: it’s a U-shaped bell-curve.
It can happen at any age and for any of a number of reasons, but there are patterns to the distribution:
Mostly affects younger people:
Allergies, asthma
Young people are less likely to have a body that’s fully adapted to all foods yet, and asthma can be triggered by certain foods (for example sulfites, a common preservative additive):
Adverse reactions to the sulphite additives
Foods/drinks that commonly contain sulfites include soft drinks, wines and beers, and dried fruit
As for the allergies side of things, you probably know the usual list of allergens to watch out for, e.g: dairy, fish, crustaceans, eggs, soy, wheat, nuts.
However, that’s far from an exhaustive list, so it’s good to see an allergist if you suspect it may be an allergic reaction.
Affects young and old people equally:
Again, there’s a dip in the middle where this doesn’t tend to affect younger adults so much, but for young and old people:
Dysphagia (difficulty swallowing)
For children, this can be a case of not having fully got used to eating yet if very small, and when growing, can be a case of “this body is constantly changing and that makes things difficult”.
For older people, this can can come from a variety of reasons, but common culprits include neurological disorders (including stroke and/or dementia), or a change in saliva quality and quantity—a side-effect of many medications:
Hyposalivation in Elderly Patients
(particularly useful in the article above is the table of drugs that are associated with this problem, and the various ways they may affect it)
Managing this may be different depending on what is causing your dysphagia (as it could be anything from antidepressants to cancer), so this is definitely one to see your doctor about. For some pointers, though:
NHS Inform | Dysphagia (swallowing problems)
Affects older people more:
Gastroesophagal reflux disease (GERD)
This is a kind of acid reflux, but chronic, and often with a slightly different set of symptoms.
GERD has no known cure once established, but its symptoms can be managed (or avoided in the first place) by:
- Healthy eating (Mediterranean diet is, as usual, great)
- Weight loss (if and only if obese)
- Avoiding trigger foods
- Eating smaller meals
- Practicing mindful eating
- Staying upright for 3–4 hours after eating
And of course, don’t smoke, and ideally don’t drink alcohol.
You can read more about this (and the different ways it can go from there), here:
NICE | Gastro-oesophageal reflux disease
Note: this above page refers to it as “GORD”, because of the British English spelling of “oesophagus” rather than “esophagus”. It’s the exact same organ and condition, just a different spelling.
Take care!
Share This Post
-

Health Insurers Limit Coverage of Prosthetic Limbs, Questioning Their Medical Necessity
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
When Michael Adams was researching health insurance options in 2023, he had one very specific requirement: coverage for prosthetic limbs.
Adams, 51, lost his right leg to cancer 40 years ago, and he has worn out more legs than he can count. He picked a gold plan on the Colorado health insurance marketplace that covered prosthetics, including microprocessor-controlled knees like the one he has used for many years. That function adds stability and helps prevent falls.
But when his leg needed replacing last January after about five years of everyday use, his new marketplace health plan wouldn’t authorize it. The roughly $50,000 leg with the electronically controlled knee wasn’t medically necessary, the insurer said, even though Colorado law leaves that determination up to the patient’s doctor, and his has prescribed a version of that leg for many years, starting when he had employer-sponsored coverage.
“The electronic prosthetic knee is life-changing,” said Adams, who lives in Lafayette, Colorado, with his wife and two kids. Without it, “it would be like going back to having a wooden leg like I did when I was a kid.” The microprocessor in the knee responds to different surfaces and inclines, stiffening up if it detects movement that indicates its user is falling.
People who need surgery to replace a joint typically don’t encounter similar coverage roadblocks. In 2021, 1.5 million knee or hip joint replacements were performed in United States hospitals and hospital-owned ambulatory facilities, according to the federal Agency for Healthcare Research and Quality, or AHRQ. The median price for a total hip or knee replacement without complications at top orthopedic hospitals was just over $68,000 in 2020, according to one analysis, though health plans often negotiate lower rates.
To people in the amputee community, the coverage disparity amounts to discrimination.
“Insurance covers a knee replacement if it’s covered with skin, but if it’s covered with plastic, it’s not going to cover it,” said Jeffrey Cain, a family physician and former chair of the board of the Amputee Coalition, an advocacy group. Cain wears two prosthetic legs, having lost his after an airplane accident nearly 30 years ago.
AHIP, a trade group for health plans, said health plans generally provide coverage when the prosthetic is determined to be medically necessary, such as to replace a body part or function for walking and day-to-day activity. In practice, though, prosthetic coverage by private health plans varies tremendously, said Ashlie White, chief strategy and programs officer at the Amputee Coalition. Even though coverage for basic prostheses may be included in a plan, “often insurance companies will put caps on the devices and restrictions on the types of devices approved,” White said.
An estimated 2.3 million people are living with limb loss in the U.S., according to an analysis by Avalere, a health care consulting company. That number is expected to as much as double in coming years as people age and a growing number lose limbs to diabetes, trauma, and other medical problems.
Fewer than half of people with limb loss have been prescribed a prosthesis, according to a report by the AHRQ. Plans may deny coverage for prosthetic limbs by claiming they aren’t medically necessary or are experimental devices, even though microprocessor-controlled knees like Adams’ have been in use for decades.
Cain was instrumental in getting passed a 2000 Colorado law that requires insurers to cover prosthetic arms and legs at parity with Medicare, which requires coverage with a 20% coinsurance payment. Since that measure was enacted, about half of states have passed “insurance fairness” laws that require prosthetic coverage on par with other covered medical services in a plan or laws that require coverage of prostheses that enable people to do sports. But these laws apply only to plans regulated by the state. Over half of people with private coverage are in plans not governed by state law.
The Medicare program’s 80% coverage of prosthetic limbs mirrors its coverage for other services. Still, an October report by the Government Accountability Office found that only 30% of beneficiaries who lost a limb in 2016 received a prosthesis in the following three years.
Cost is a factor for many people.
“No matter your coverage, most people have to pay something on that device,” White said. As a result, “many people will be on a payment plan for their device,” she said. Some may take out loans.
The federal Consumer Financial Protection Bureau has proposed a rule that would prohibit lenders from repossessing medical devices such as wheelchairs and prosthetic limbs if people can’t repay their loans.
“It is a replacement limb,” said White, whose organization has heard of several cases in which lenders have repossessed wheelchairs or prostheses. Repossession is “literally a punishment to the individual.”
Adams ultimately owed a coinsurance payment of about $4,000 for his new leg, which reflected his portion of the insurer’s negotiated rate for the knee and foot portion of the leg but did not include the costly part that fits around his stump, which didn’t need replacing. The insurer approved the prosthetic leg on appeal, claiming it had made an administrative error, Adams said.
“We’re fortunate that we’re able to afford that 20%,” said Adams, who is a self-employed leadership consultant.
Leah Kaplan doesn’t have that financial flexibility. Born without a left hand, she did not have a prosthetic limb until a few years ago.
Growing up, “I didn’t want more reasons to be stared at,” said Kaplan, 32, of her decision not to use a prosthesis. A few years ago, the cycling enthusiast got a prosthetic hand specially designed for use with her bike. That device was covered under the health plan she has through her county government job in Spokane, Washington, helping developmentally disabled people transition from school to work.
But when she tried to get approval for a prosthetic hand to use for everyday activities, her health plan turned her down. The myoelectric hand she requested would respond to electrical impulses in her arm that would move the hand to perform certain actions. Without insurance coverage, the hand would cost her just over $46,000, which she said she can’t afford.
Working with her doctor, she has appealed the decision to her insurer and been denied three times. Kaplan said she’s still not sure exactly what the rationale is, except that the insurer has questioned the medical necessity of the prosthetic hand. The next step is to file an appeal with an independent review organization certified by the state insurance commissioner’s office.
A prosthetic hand is not a luxury device, Kaplan said. The prosthetic clinic has ordered the hand and made the customized socket that will fit around the end of her arm. But until insurance coverage is sorted out, she can’t use it.
At this point she feels defeated. “I’ve been waiting for this for so long,” Kaplan said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
This article first appeared on KFF Health News and is republished here under a Creative Commons license.
Share This Post

Related Posts
-

Growing Young – by Marta Zaraska
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This one will be a slightly mixed review, but we think the book has more than enough of value to make it a very worthwhile read.
The premise of the book is that, as the subtitle suggests, positive social qualities increase personal longevity.
Author (and science journalist) Marta Zaraska looks at a lot of research to back this up, and also did a lot of travelling and digging into stories. This is of great value, because she notes where a lot of misconceptions have arisen.
To give one example, it’s commonly noted that marriage (or as-though-marriage life partnerships) is generally* associated with longer life.
*Statistics suggest that marriage-related longevity is enjoyed by men married to women, and people in same-sex marriages regardless of gender, but is not so much the case for women married to men.
However! Zaraska notes a factor she learned from Gottman’s research (yes, that Gottman), that what matters is not the official status of a relationship, so much as the sense of secure lifelong commitment to it.
These kinds of observations (throughout the book) add an extra layer beyond “common wisdom”, and allow us to better understand what’s really going on. The book’s main weaknesses, meanwhile, are twofold:
- The author is (in this reviewer’s opinion) unduly dismissive of physical health lifestyle factors such as diet and exercise, because they “only” account for a similar bonus to healthy longevity.
- Like many, she does not always consider where correlation might not mean causation. For example, she cites that volunteering free time increases healthspan by 22%, but neglects to note that perhaps it is having the kind of socioeconomic situation that allows one free time to volunteer, that gives the benefit.
Bottom line: the book has its flaws, but we think that only serves to make it more engaging. After all, reading should not be a purely passive activity! Zaraska’s well-studied insights give plenty of pointers for tweaking the social side of anyone’s quest for healthy longevity.
Click here to check out Growing Young, increase your healthspan, and take joy in doing it!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

The Gym For Your Mental Health
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Getting The Most Out Of Therapy
If you’ve never had therapy, what image do you have of it? Perhaps you imagine a bearded and bespectacled man in a suit, impassively making notes on a clipboard. Perhaps you imagine an empathetic woman, with tissues and camomile tea on standby.
The reality is: the experience of therapy can vary, a lot.
In its results, too! Sometimes we may try therapy and think “well that was a waste of time and money”. Sometimes we may try therapy and it’ll change our life.
So… Is there any way to make it less of a lottery?
First: knowledge is power
And while the therapist-client relationship certainly shouldn’t be a power struggle, you do want to be empowered.
So, read about different styles of therapy, and also, read some how-to guides for self-therapy. We’ve recommended some before in previous editions of 10almonds; you can check those books out here:
- How to Be Your Own Therapist: Boost your mood and reduce your anxiety in 10 minutes a day – by Owen O’Kane
- You Are the One You’ve Been Waiting For: Applying Internal Family Systems to Intimate Relationships – by Dr. Richard Schwartz
- DBT Made Simple: A Step-by-Step Guide to Dialectical Behavior Therapy – by Sheri van Dijk
- How to Do the Work: Recognize Your Patterns, Heal from Your Past, and Create Your Self – by Dr. Nicole LaPera
This will serve two purposes:
- You’ll know what to expect out of a therapist
- You can more efficiently “get to work” in therapy
It also, of course, could help you already, without even going to therapy!
Second: begin with the end in mind
A person who does not know what they want to get out of therapy, will likely not get much out of therapy. Or rather, their first task will be to figure that out. So, figure it out in advance, if you can.
Maybe you have a problem that has a specific name, for example poor self-esteem, anxiety, stress, depression, trauma, neuroticism, phobia, etc.
This isn’t Alcoholics Anonymous, and in this case you don’t want a lifetime of “Hello, my name is ______ and I have ______”, if you can help it.
So, what do you want?
- Maybe you want to be able to go to social events without feeling anxious
- Maybe you want your relationship(s) to be more secure and fulfilling
- Maybe you want to no longer have nightmares about that traumatic thing
- Maybe you want to be able to greet each day’s tasks with confidence and without overwhelm
…etc.
A good therapist will help you to set such goals (if you haven’t already), and attain them.
If you’re going the self-therapy route, then this is your job now!
It will probably start with the question: imagine that everything currently troubling you is now healed.
What would that look like, to you?
Third: get a good match for you
Unless you are going entirely the self-therapy route (which can work for some), you will want a therapist who’s a good match for you.
It may take a degree of “suck it and see” trial runs before you find the right one, but that takes time and money, so you’ll want to streamline the process as much as you can. If you do this well, you may be able to find a good therapist for you first time.
For this, personal recommendations (such as from friends) may help more than exmaining academic and institutional affiliations.
Yes, you want a well-qualified therapist who is a member in good standing of a respectable regulated body… but whether your therapist is easy for you to “get on with” will matter at least as much as whether their approach is psychodynamic, or 4th wave CBT, or IFS, or whatever seems popular in your time and place.
Bear in mind:
- Some therapists are specialized in helping with some kinds of things and not others. It will obviously help if the therapist you choose is specialized in the thing you are seeking help for.
- Some therapists may be able to relate to you better (or not), based on simple factors of who they are. To this end, while your therapist certainly doesn’t have to be a mirror image of you, factors like age, gender, race, etc can be relevant and may be worth considering, depending on what you are seeking help with, and what factors impact that thing.
Prefer keeping things to yourself?
Therapy isn’t for everyone, but having a good relationship with oneself definitely is. You might want to invest in one of the books whose reviews we linked above, and you might also get value from previous Psychology Sunday articles, which you can find in our archive (every seventh edition here has a Psychology Sunday main feature):
Click Here To Check Out The 10almonds Archive
To borrow the catchphrase of Dr. Kirk Honda (a therapist and therapy educator with decades of experience):
❝Take care of yourself, because you deserve it; you really, really do.❞
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Radiant Rebellion – by Karen Walrond
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In health terms, we are often about fighting aging here. But to be more specific, what we’re fighting in those cases is not truly aging itself, so much as age-related decline.
Karen Walrond makes a case that we’ve made from the very start of 10almonds (but she wrote a whole book about it), that there’s merit in looking at what we can and can’t control about aging, doing what we reasonably can, and embracing what we can’t.
And yes, embracing, not merely accepting. This is not a downer of a book; it’s a call to revolution. It asks us to be proud of our grey hairs, to see our smile-lines around our eyes as the sign of a lived-in body, and even to embrace some of the unavoidable “actual decline” things as part of the journey of life. Maybe we’re not as strong as we used to be and now need a grippety-doodah to open jars; not everyone gets to live long enough to experience that! How lucky we are.
Perhaps most importantly, she bids us be the change we want to see in the world, and inspire others with our choices and actions, and shake off ageist biases for good.
Bottom line: if you want to foster a better attitude to aging not only for yourself, but also those around you, then this is a top-tier book for that.
Click here to check out Radiant Rebellion, and reclaim aging!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: