A short history of sunscreen, from basting like a chook to preventing skin cancer
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australians have used commercial creams, lotions or gels to manage our skin’s sun exposure for nearly a century.
But why we do it, the preparations themselves, and whether they work, has changed over time.
In this short history of sunscreen in Australia, we look at how we’ve slathered, slopped and spritzed our skin for sometimes surprising reasons.
At first, suncreams helped you ‘tan with ease’
Trove/NLA
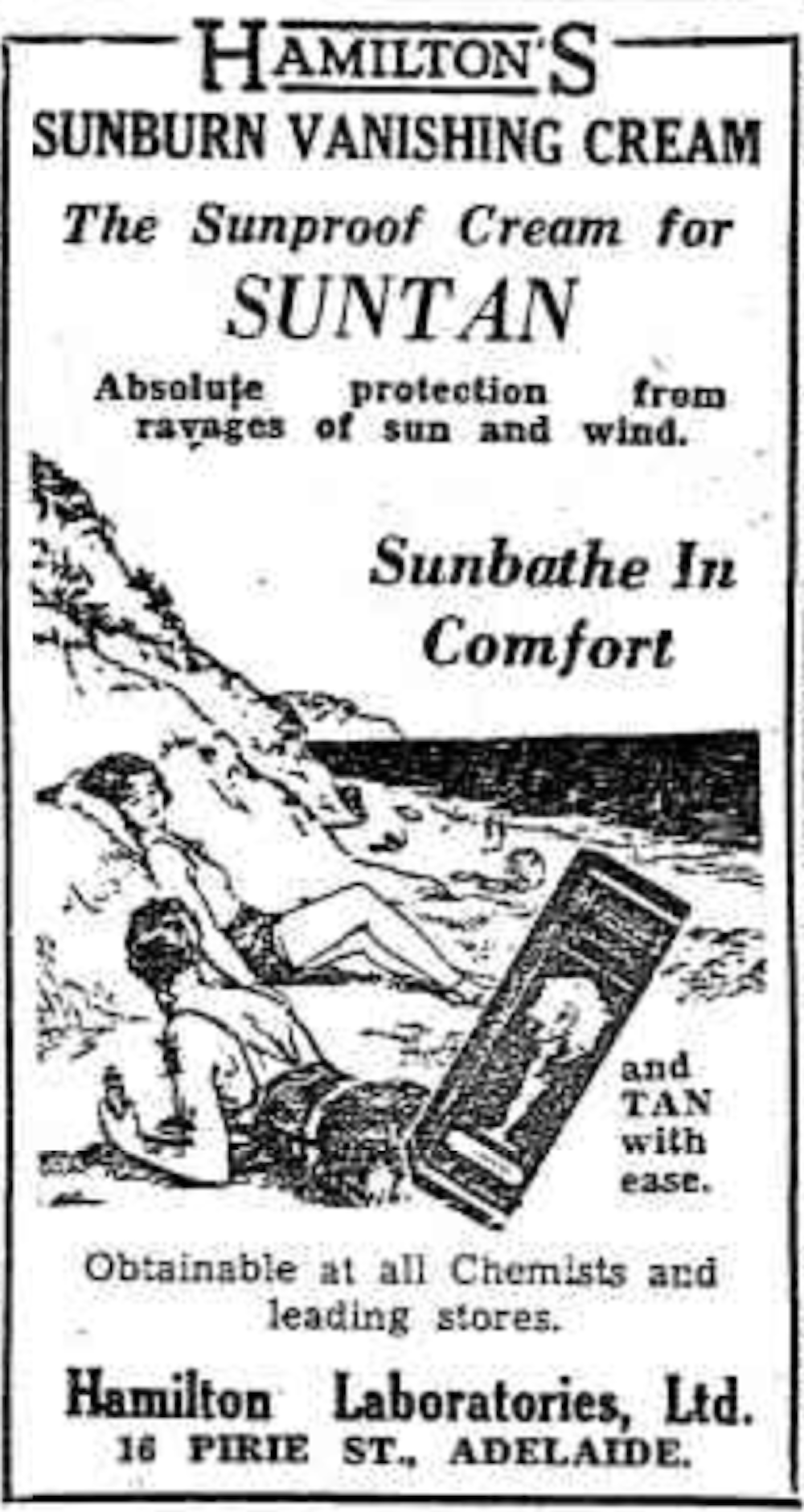
Sunscreens have been available in Australia since the 30s. Chemist Milton Blake made one of the first.
He used a kerosene heater to cook batches of “sunburn vanishing cream”, scented with French perfume.
His backyard business became H.A. Milton (Hamilton) Laboratories, which still makes sunscreens today.
Hamilton’s first cream claimed you could “
Sunbathe in Comfort and TAN with ease”. According to modern standards, it would have had an SPF (or sun protection factor) of 2.
The mirage of ‘safe tanning’
A tan was considered a “modern complexion” and for most of the 20th century, you might put something on your skin to help gain one. That’s when “safe tanning” (without burning) was thought possible.
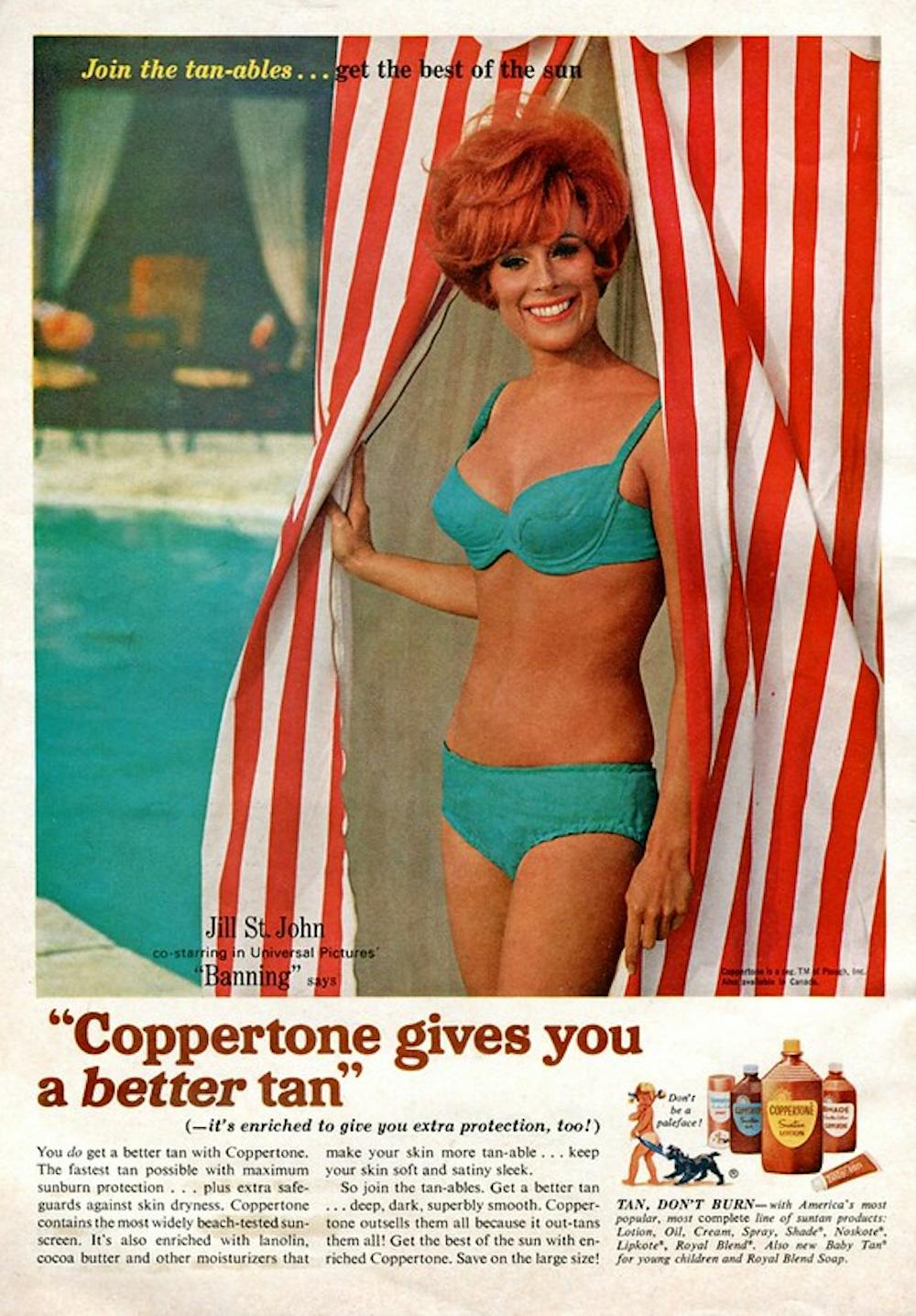
SenseiAlan/Flickr, CC BY-SA
Sunburn was known to be caused by the UVB component of ultraviolet (UV) light. UVA, however, was thought not to be involved in burning; it was just thought to darken the skin pigment melanin. So, medical authorities advised that by using a sunscreen that filtered out UVB, you could “safely tan” without burning.
But that was wrong.
From the 70s, medical research suggested UVA penetrated damagingly deep into the skin, causing ageing effects such as sunspots and wrinkles. And both UVA and UVB could cause skin cancer.
Sunscreens from the 80s sought to be “broad spectrum” – they filtered both UVB and UVA.
Researchers consequently recommended sunscreens for all skin tones, including for preventing sun damage in people with dark skin.
Delaying burning … or encouraging it?
Up to the 80s, sun preparations ranged from something that claimed to delay burning, to preparations that actively encouraged it to get that desirable tan – think, baby oil or coconut oil. Sun-worshippers even raided the kitchen cabinet, slicking olive oil on their skin.
One manufacturer’s “sun lotion” might effectively filter UVB; another’s merely basted you like a roast chicken.
Since labelling laws before the 80s didn’t require manufacturers to list the ingredients, it was often hard for consumers to tell which was which.
At last, SPF arrives to guide consumers
In the 70s, two Queensland researchers, Gordon Groves and Don Robertson, developed tests for sunscreens – sometimes experimenting on students or colleagues. They printed their ranking in the newspaper, which the public could use to choose a product.
An Australian sunscreen manufacturer then asked the federal health department to regulate the industry. The company wanted standard definitions to market their products, backed up by consistent lab testing methods.
In 1986, after years of consultation with manufacturers, researchers and consumers, Australian Standard AS2604 gave a specified a testing method, based on the Queensland researchers’ work. We also had a way of expressing how well sunscreens worked – the sun protection factor or SPF.
This is the ratio of how long it takes a fair-skinned person to burn using the product compared with how long it takes to burn without it. So a cream that protects the skin sufficiently so it takes 40 minutes to burn instead of 20 minutes has an SPF of 2.
Manufacturers liked SPF because businesses that invested in clever chemistry could distinguish themselves in marketing. Consumers liked SPF because it was easy to understand – the higher the number, the better the protection.
Australians, encouraged from 1981 by the Slip! Slop! Slap! nationwide skin cancer campaign, could now “slop” on a sunscreen knowing the degree of protection it offered.
How about skin cancer?
It wasn’t until 1999 that research proved that using sunscreen prevents skin cancer. Again, we have Queensland to thank, specifically the residents of Nambour. They took part in a trial for nearly five years, carried out by a research team led by Adele Green of the Queensland Institute of Medical Research. Using sunscreen daily over that time reduced rates of squamous cell carcinoma (a common form of skin cancer) by about 60%.
Follow-up studies in 2011 and 2013 showed regular sunscreen use almost halved the rate of melanoma and slowed skin ageing. But there was no impact on rates of basal cell carcinoma, another common skin cancer.
By then, researchers had shown sunscreen stopped sunburn, and stopping sunburn would prevent at least some types of skin cancer.
What’s in sunscreen today?
An effective sunscreen uses one or more active ingredients in a cream, lotion or gel. The active ingredient either works:
-
“chemically” by absorbing UV and converting it to heat. Examples include PABA (para-aminobenzoic acid) and benzyl salicylate, or
-
“physically” by blocking the UV, such as zinc oxide or titanium dioxide.
Physical blockers at first had limited cosmetic appeal because they were opaque pastes. (Think cricketers with zinc smeared on their noses.)
With microfine particle technology from the 90s, sunscreen manufacturers could then use a combination of chemical absorbers and physical blockers to achieve high degrees of sun protection in a cosmetically acceptable formulation.
Where now?
Australians have embraced sunscreen, but they still don’t apply enough or reapply often enough.
Although some people are concerned sunscreen will block the skin’s ability to make vitamin D this is unlikely. That’s because even SPF50 sunscreen doesn’t filter out all UVB.
There’s also concern about the active ingredients in sunscreen getting into the environment and whether their absorption by our bodies is a problem.
Sunscreens have evolved from something that at best offered mild protection to effective, easy-to-use products that stave off the harmful effects of UV. They’ve evolved from something only people with fair skin used to a product for anyone.
Remember, slopping on sunscreen is just one part of sun protection. Don’t forget to also slip (protective clothing), slap (hat), seek (shade) and slide (sunglasses).![]()
Laura Dawes, Research Fellow in Medico-Legal History, Australian National University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why Chronic Obstructive Pulmonary Disease (COPD) Is More Likely Than You Think

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Chronic Obstructive Pulmonary Disease (COPD): More Likely Than You Think
COPD is not so much one disease, as rather a collection of similar (and often overlapping) diseases. The main defining characteristic is that they are progressive lung diseases. Historically the most common have been chronic bronchitis and emphysema, though Long COVID and related Post-COVID conditions appear to have been making inroads.
Lung cancer is generally considered separately, despite being a progressive lung disease, but there is crossover too:
COPD prevalence is increased in lung cancer, independent of age, sex and smoking history
COPD can be quite serious:
“But I don’t smoke”
Great! In fact we imagine our readership probably has disproportionately few smokers compared to the general population, being as we all are interested in our health.
But, it’s estimated that 30,000,000 Americans have COPD, and approximately half don’t know it. Bear in mind, the population of the US is a little over 340,000,000, so that’s a little under 9% of the population.
Click here to see a state-by-state breakdown (how does your state measure up?)
How would I know if I have it?
It typically starts like any mild respiratory illness. Likely shortness of breath, especially after exercise, a mild cough, and a frequent need to clear your throat.
Then it will get worse, as the lungs become more damaged; each of those symptoms might become stronger, as well as chest tightness and a general lack of energy.
Later stages, you guessed it, the same but worse, and—tellingly—weight loss.
The reason for the weight loss is because you are getting less oxygen per breath, making carrying your body around harder work, meaning you burn more calories.
What causes it?
Lots of things, with smoking being up at the top, or being exposed to a lot of second-hand smoke. Working in an environment with a lot of air pollution (for example, working around chemical fumes) can cause it, as can inhaling dust. New Yorkers: yes, that dust too. It can also develop from other respiratory illnesses, and some people even have a genetic predisposition to it:
Alpha-1 antitrypsin deficiency: a commonly overlooked cause of lung disease
Is it treatable?
Treatment varies depending on what form of it you have, and most of the medical interventions are beyond the scope of this article. Suffice it to say, there are medications that can be taken (including bronchodilators taken via an inhaler device), corticosteroids, antibiotics and antivirals of various kinds if appropriate. This is definitely a “see your doctor” item though, because there are is far too much individual variation for us to usefully advise here.
However!
There are habits we can do to a) make COPD less likely and b) make COPD at least a little less bad if we get it.
Avoiding COPD:
- Don’t smoke. Just don’t.
- Avoid second-hand smoke if you can
- Avoid inhaling other chemicals/dust that may be harmful
- Breathe through your nose, not your mouth; it filters the air in a whole bunch of ways
- Seriously, we know it seems like nostril hairs surely can’t do much against tiny particles, but tiny particles are attracted to them and get stuck in mucous and dealt with by our immune system, so it really does make a big difference
Managing COPD:
- Continue the above things, of course
- Exercise regularly, even just light walking helps; we realize it will be difficult
- Maintain a healthy weight if you can
- This means both ways; COPD causes weight loss and that needs to be held in check. But similarly, you don’t want to be carrying excessive weight either; that will tire you even more.
- Look after the rest of your health; everything else will now hit you harder, so even small things need to be taken seriously
- If you can, get someone to help / do your household cleaning for you, ideally while you are not in the room.
Where can I get more help/advice?
As ever, speak to your doctor if you are concerned this may be affecting you. You can also find a lot of resources via the COPD Foundation’s website.
Take care of yourself!
Share This Post
- Don’t smoke. Just don’t.
-

Bell Pepper vs Eggplant – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing bell pepper to eggplant, we picked the eggplant.
Why?
First, you might remember that different color bell peppers have different nutritional profiles. So, you might be wondering why we didn’t specify the color. The reason is: the things that differ from one color to another are important differences between the respective bell peppers, but they make no difference to this comparison, as for any given nutrient that changes from one color to another, it doesn’t change whether or not it beats eggplant (in fact, for all the things that change, the weakest bell pepper for each one still beats eggplant).
With that latter comment in mind, you might be wondering how eggplant wins overall. It’s because…
In terms of macros, eggplant has notably more fiber for approximately the same carbs and protein, making it the winner in this category.
In the category of vitamins, bell pepper (of any color) has more of vitamins A, B2, B6, C, E, and K, while eggplant has more of vitamins B1, B5, and B9, meaning bell peppers win this round. Notably, the things that vary by color here are vitamins A, B6, and C. However, the color doesn’t change whether or not it beats eggplant; it only changes the amount (and in the case of vitamin A, the order of magnitude) by which it beats it.
When it comes to minerals, bell peppers have more iron and zinc, while eggplant has more calcium, copper, magnesium, manganese, phosphorus, potassium, and selenium. A clear win for eggplant here.
Adding up the sections gives an overall win for eggplant, but by all means enjoy either or both; they both have their merits and diversity is good!
Want to learn more?
You might like:
Which Bell Peppers To Pick? A Spectrum Of Specialties ← for the differences between the different colors
Enjoy!
Share This Post
-
Pineapple vs Raspberries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing pineapple to raspberries, we picked the raspberries.
Why?
In terms of macros, pineapple has slightly more carbs, while raspberries have more than 4x the fiber, and for what it’s worth (which isn’t much, because the numbers are tiny), 2x the protein. Thus, an easy win for raspberries in the macros category.
In the category of vitamins, pineapple has more of vitamins A, B1, B6, and C, while raspberries have more of vitamins B2, B3, B5, B7, B9, E, and K, winning easily again.
Looking at minerals, pineapple has slightly more copper and manganese, while raspberries have more calcium, iron, magnesium, phosphorus, potassium, selenium, and zinc, for a third win in a row.
In other considerations, pineapple has bromelain, which is unique to it and has many beneficial properties (see the “learn more” section below), while raspberries (like most berries) have a lot more polyphenols. So, we’re calling this round a tie.
Adding up the sections makes for a clear overall win for raspberries, but by all means enjoy either or both, as diversity is good!
Want to learn more?
You might like:
Bromelain vs Inflammation & Much More
Enjoy!
Share This Post


-

Salt Sugar Fat – by Michael Moss
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You are probably already aware that food giants put unhealthy ingredients in processed food. So what does this book offer of value?
Sometimes, better understanding leads to better movation. In this case, while a common (reasonable) view has been:
“The food giants fill their food with salt, sugar, and fat, because it makes that food irresistibly delicious”
…but that doesn’t exactly put us off the food, does it? It just makes it a guilty pleasure. Ah yes, the irresistible McDouble Dopamineburger. The time-honored tradition of Pizza Night; a happy glow; a special treat.
What Pulitzer-winning author Michael Moss brings to us is different.
He examines not just how they hooked us, but why. And the answer is not merely the obvious “profit and greed”, but also “survival, under capitalism”. That without regulation forcing companies to keep salt/sugar/fat levels down, companies that have tried to do so voluntarily have quickly had to u-turn to regain any hope of competitiveness.
He also looks at how the salt/sugar/fat components are needed to mask the foul taste of the substandard ingredients they use to maintain lower costs… Processed food, without the heavy doses of salt/sugar/fat, is not anywhere close to what you might make at home. Industry will cut costs where it can.
Bottom line: if you need a push to kick the processed food habit, this is the book that will do it.
Click here to check out Salt Sugar Fat, and reclaim your health!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Women don’t have a ‘surge’ in fertility before menopause – but surprise pregnancies can happen, even after 45
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Every now and then we see media reports about celebrities in their mid 40s having surprise pregnancies. Or you might hear stories like these from friends or relatives, or see them on TV.
Menopause signals the end of a woman’s reproductive years and happens naturally between age 45 and 55 (the average is 51). After 12 months with no periods, a woman is considered postmenopausal.
While the chance of pregnancy is very low in the years leading up to menopause – the so called menopausal transition or perimenopause – the chance is not zero.
So, what do we know about the chance of conceiving naturally after age 45? And what are the risks?

IKO-studio/Shutterstock Is there a spike in fertility before menopause?
The hormonal changes that accompany perimenopause cause changes to the menstrual cycle pattern, and some have suggested there can be a “surge” in fertility at perimenopause. But there’s no evidence this exists.
In the years leading up to menopause, a woman’s periods often become irregular, and she might have some of the common symptoms of menopause such as hot flushes and night sweats.
This might lead women to think they have hit menopause and can’t get pregnant anymore. But while pregnancy in a woman in her mid 40s is significantly less likely compared to a woman in her 20s or 30s, it’s still possible.
The stats for natural pregnancies after age 45
Although women in their mid- to late 40s sometimes have “miracle babies”, the chance of pregnancy is minimal in the five to ten years leading up to menopause.
The monthly chance of pregnancy in a woman aged 30 is about 20%. By age 40 it’s less than 5% and by age 45 the chance is negligible.
We don’t know exactly how many women become pregnant in their mid to late 40s, as many pregnancies at this age miscarry. The risk of miscarriage increases from 10% in women in their 20s to more than 50% in women aged 45 years or older. Also, for personal or medical reasons some pregnancies are terminated.
According to a review of demographic data on age when women had their final birth across several countries, the median age was 38.6 years. But the range of ages reported for last birth in the reviewed studies showed a small proportion of women give birth after age 45.
Having had many children before seems to increase the odds of giving birth after age 45. A study of 209 women in Israel who had conceived spontaneously and given birth after age 45 found 81% had already had six or more deliveries and almost half had had 11 or more previous deliveries.
Conceiving naturally at age 45 plus is not unheard of. pixelheadphoto digitalskillet/Shutterstock There’s no reliable data on how common births after age 45 are in Australia. The most recent report on births in Australia show that about 5% of babies are born to women aged 40 years or older.
However, most of those were likely born to women aged between 40 and 45. Also, the data includes women who conceive with assisted reproductive technologies, including with the use of donor eggs. For women in their 40s, using eggs donated by a younger woman significantly increases their chance of having a baby with IVF.
What to be aware of if you experience a late unexpected pregnancy
A surprise pregnancy late in life often comes as a shock and deciding what to do can be difficult.
Depending on their personal circumstances, some women decide to terminate the pregnancy. Contrary to the stereotype that abortions are most common among very young women, women aged 40–44 are more likely to have an abortion than women aged 15–19.
This may in part be explained by the fact older women are up to ten times more likely to have a fetus with chromosomal abnormalities.
There are some extra risks involved in pregnancy when the mother is older. More than half of pregnancies in women aged 45 and older end in miscarriage and some are terminated if prenatal testing shows the fetus has the wrong number of chromosomes.
This is because at that age, most eggs have chromosomal abnormalities. For example, the risk of having a pregnancy affected by Down syndrome is one in 86 at age 40 compared to one in 1,250 at age 20.
There are some added risks associated with pregnancy when the mother is older. Natalia Deriabina/Shutterstock Apart from the increased risk of chromosomal abnormalities, advanced maternal age also increases the risk of stillbirth, fetal growth restriction (when the unborn baby doesn’t grow properly), preterm birth, pre-eclampsia, gestational diabetes and caesarean section.
However, it’s important to remember that since the overall risk of all these things is small, even with an increase, the risk is still small and most babies born to older mothers are born healthy.
Multiple births are also more common in older women than in younger women. This is because older women are more likely to release more than one egg if and when they ovulate.
A study of all births in England and Wales found women aged 45 and over were the most likely to have a multiple birth.
The risks of babies being born prematurely and having health complications are higher in twin than singleton pregnancies, and the risks are highest in women of advanced maternal age.
What if you want to become pregnant in your 40s?
If you’re keen to avoid pregnancy during perimenopause, it’s recommended you use contraception.
But if you want to get pregnant in your 40s, there are some things you can do to boost your chance of conceiving and having a healthy baby.
These include preparing for pregnancy by seeing a GP for a preconception health check, taking folic acid and iodine supplements, not smoking, limiting alcohol consumption, maintaining a healthy weight, exercising regularly and having a nutritious diet.
If you get good news, talking to a doctor about what to expect and how to best manage a pregnancy in your 40s can help you be prepared and will allow you to get personalised advice based on your health and circumstances.
Karin Hammarberg, Adjunct Senior Research Fellow, Global and Women’s Health, School of Public Health & Preventive Medicine, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How Aging Changes At 44 And Again At 60 (And What To Do About It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
As it turns out, aging is not linear. Or rather: chronological aging may be, but biological aging isn’t, and there are parts of our life where it kicks into a different gear. This study looked at 108 people (65 of whom women) between the ages of 25 and 75, as part of a longitudinal cohort study, tracked for around 2–8 years (imprecise as not all follow-up durations were the same). They took frequent blood and urine samples, and tested them for thousands of different molecules and analyzing changes in gene expression, proteomic, blood biomarkers, and more. All things that are indicators of various kinds of health/disease, and which might seem more simple but it isn’t: aging.
Here’s what they found:
Landmark waypoints
At 44, significant changes occur in the metabolism, including notably the metabolism of carbs, caffeine, and alcohol. A large portion of this may be hormone related, as that’s a time of change not just for those undergoing the menopause, but also the andropause (not entirely analogous to the menopause, but it does usually entail a significant reduction in sex hormone production; in this case, testosterone).
However, the study authors also hypothesize that lifestyle factors may be relevant, as one’s 40s are often a stressful time, and an increase in alcohol consumption often occurs around the same time as one’s ability to metabolize it drops, resulting in further dysfunctional alcohol metabolism.
At 60, carb metabolism slows again, with big changes in glucose metabolism specifically, as well as an increased risk of cardiovascular disease, and a decline in kidney function. In case that wasn’t enough: also an increase free radical pathology, meaning a greatly increased risk of cancer. Immune function drops too.
What to do about this: the recommendation is of course to be proactive, and look after various aspects of your health before it becomes readily apparent that you need to. For example, good advice for anyone approaching 44 might be to quit alcohol, go easy on caffeine, and eat a diet that is conducive to good glucose metabolism. Similarly, good advice for anyone approaching 60 might be to do the same, and also pay close attention to keeping your kidneys healthy. Getting regular tests done is also key, including optional extras that your doctor might not suggest but you should ask for, such as blood urea nitrogen levels (biomarkers of kidney function). The more we look after each part of our body, the more they can look after us in turn, and the fewer/smaller problems we’ll have down the line.
If you, dear reader, are approaching the age 44 or 60… Be neither despondent nor complacent. We must avoid falling into the dual traps of “Well, that’s it, bad health is around the corner, nothing I can do about it; that’s nature”, vs “I’ll be fine, statistics are for other people, and don’t apply to me”.
Those are averages, and we do not have to be average. Every population has statistical outliers. But it would be hubris to think none of this will apply to us and we can just carry on regardless. So, for those of us who are approaching one of those two ages… It’s time to saddle up, knuckle down, and do our best!
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Also, if you’d like to read the actual paper by Dr. Xiaotao Shen et al., here it is:
Nonlinear dynamics of multi-omics profiles during human aging ← honestly, it’s a lot clearer and more informative than the video, and also obviously discusses things in a lot more detail than we have room to here
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: