Overdosing on Chemo: A Common Gene Test Could Save Hundreds of Lives Each Year
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
One January morning in 2021, Carol Rosen took a standard treatment for metastatic breast cancer. Three gruesome weeks later, she died in excruciating pain from the very drug meant to prolong her life.
Rosen, a 70-year-old retired schoolteacher, passed her final days in anguish, enduring severe diarrhea and nausea and terrible sores in her mouth that kept her from eating, drinking, and, eventually, speaking. Skin peeled off her body. Her kidneys and liver failed. “Your body burns from the inside out,” said Rosen’s daughter, Lindsay Murray, of Andover, Massachusetts.
Rosen was one of more than 275,000 cancer patients in the United States who are infused each year with fluorouracil, known as 5-FU, or, as in Rosen’s case, take a nearly identical drug in pill form called capecitabine. These common types of chemotherapy are no picnic for anyone, but for patients who are deficient in an enzyme that metabolizes the drugs, they can be torturous or deadly.
Those patients essentially overdose because the drugs stay in the body for hours rather than being quickly metabolized and excreted. The drugs kill an estimated 1 in 1,000 patients who take them — hundreds each year — and severely sicken or hospitalize 1 in 50. Doctors can test for the deficiency and get results within a week — and then either switch drugs or lower the dosage if patients have a genetic variant that carries risk.
Yet a recent survey found that only 3% of U.S. oncologists routinely order the tests before dosing patients with 5-FU or capecitabine. That’s because the most widely followed U.S. cancer treatment guidelines — issued by the National Comprehensive Cancer Network — don’t recommend preemptive testing.
The FDA added new warnings about the lethal risks of 5-FU to the drug’s label on March 21 following queries from KFF Health News about its policy. However, it did not require doctors to administer the test before prescribing the chemotherapy.
The agency, whose plan to expand its oversight of laboratory testing was the subject of a House hearing, also March 21, has said it could not endorse the 5-FU toxicity tests because it’s never reviewed them.
But the FDA at present does not review most diagnostic tests, said Daniel Hertz, an associate professor at the University of Michigan College of Pharmacy. For years, with other doctors and pharmacists, he has petitioned the FDA to put a black box warning on the drug’s label urging prescribers to test for the deficiency.
“FDA has responsibility to assure that drugs are used safely and effectively,” he said. The failure to warn, he said, “is an abdication of their responsibility.”
The update is “a small step in the right direction, but not the sea change we need,” he said.
Europe Ahead on Safety
British and European Union drug authorities have recommended the testing since 2020. A small but growing number of U.S. hospital systems, professional groups, and health advocates, including the American Cancer Society, also endorse routine testing. Most U.S. insurers, private and public, will cover the tests, which Medicare reimburses for $175, although tests may cost more depending on how many variants they screen for.
In its latest guidelines on colon cancer, the Cancer Network panel noted that not everyone with a risky gene variant gets sick from the drug, and that lower dosing for patients carrying such a variant could rob them of a cure or remission. Many doctors on the panel, including the University of Colorado oncologist Wells Messersmith, have said they have never witnessed a 5-FU death.
In European hospitals, the practice is to start patients with a half- or quarter-dose of 5-FU if tests show a patient is a poor metabolizer, then raise the dose if the patient responds well to the drug. Advocates for the approach say American oncology leaders are dragging their feet unnecessarily, and harming people in the process.
“I think it’s the intransigence of people sitting on these panels, the mindset of ‘We are oncologists, drugs are our tools, we don’t want to go looking for reasons not to use our tools,’” said Gabriel Brooks, an oncologist and researcher at the Dartmouth Cancer Center.
Oncologists are accustomed to chemotherapy’s toxicity and tend to have a “no pain, no gain” attitude, he said. 5-FU has been in use since the 1950s.
Yet “anybody who’s had a patient die like this will want to test everyone,” said Robert Diasio of the Mayo Clinic, who helped carry out major studies of the genetic deficiency in 1988.
Oncologists often deploy genetic tests to match tumors in cancer patients with the expensive drugs used to shrink them. But the same can’t always be said for gene tests aimed at improving safety, said Mark Fleury, policy director at the American Cancer Society’s Cancer Action Network.
When a test can show whether a new drug is appropriate, “there are a lot more forces aligned to ensure that testing is done,” he said. “The same stakeholders and forces are not involved” with a generic like 5-FU, first approved in 1962, and costing roughly $17 for a month’s treatment.
Oncology is not the only area in medicine in which scientific advances, many of them taxpayer-funded, lag in implementation. For instance, few cardiologists test patients before they go on Plavix, a brand name for the anti-blood-clotting agent clopidogrel, although it doesn’t prevent blood clots as it’s supposed to in a quarter of the 4 million Americans prescribed it each year. In 2021, the state of Hawaii won an $834 million judgment from drugmakers it accused of falsely advertising the drug as safe and effective for Native Hawaiians, more than half of whom lack the main enzyme to process clopidogrel.
The fluoropyrimidine enzyme deficiency numbers are smaller — and people with the deficiency aren’t at severe risk if they use topical cream forms of the drug for skin cancers. Yet even a single miserable, medically caused death was meaningful to the Dana-Farber Cancer Institute, where Carol Rosen was among more than 1,000 patients treated with fluoropyrimidine in 2021.
Her daughter was grief-stricken and furious after Rosen’s death. “I wanted to sue the hospital. I wanted to sue the oncologist,” Murray said. “But I realized that wasn’t what my mom would want.”
Instead, she wrote Dana-Farber’s chief quality officer, Joe Jacobson, urging routine testing. He responded the same day, and the hospital quickly adopted a testing system that now covers more than 90% of prospective fluoropyrimidine patients. About 50 patients with risky variants were detected in the first 10 months, Jacobson said.
Dana-Farber uses a Mayo Clinic test that searches for eight potentially dangerous variants of the relevant gene. Veterans Affairs hospitals use a 11-variant test, while most others check for only four variants.
Different Tests May Be Needed for Different Ancestries
The more variants a test screens for, the better the chance of finding rarer gene forms in ethnically diverse populations. For example, different variants are responsible for the worst deficiencies in people of African and European ancestry, respectively. There are tests that scan for hundreds of variants that might slow metabolism of the drug, but they take longer and cost more.
These are bitter facts for Scott Kapoor, a Toronto-area emergency room physician whose brother, Anil Kapoor, died in February 2023 of 5-FU poisoning.
Anil Kapoor was a well-known urologist and surgeon, an outgoing speaker, researcher, clinician, and irreverent friend whose funeral drew hundreds. His death at age 58, only weeks after he was diagnosed with stage 4 colon cancer, stunned and infuriated his family.
In Ontario, where Kapoor was treated, the health system had just begun testing for four gene variants discovered in studies of mostly European populations. Anil Kapoor and his siblings, the Canadian-born children of Indian immigrants, carry a gene form that’s apparently associated with South Asian ancestry.
Scott Kapoor supports broader testing for the defect — only about half of Toronto’s inhabitants are of European descent — and argues that an antidote to fluoropyrimidine poisoning, approved by the FDA in 2015, should be on hand. However, it works only for a few days after ingestion of the drug and definitive symptoms often take longer to emerge.
Most importantly, he said, patients must be aware of the risk. “You tell them, ‘I am going to give you a drug with a 1 in 1,000 chance of killing you. You can take this test. Most patients would be, ‘I want to get that test and I’ll pay for it,’ or they’d just say, ‘Cut the dose in half.’”
Alan Venook, the University of California-San Francisco oncologist who co-chairs the panel that sets guidelines for colorectal cancers at the National Comprehensive Cancer Network, has led resistance to mandatory testing because the answers provided by the test, in his view, are often murky and could lead to undertreatment.
“If one patient is not cured, then you giveth and you taketh away,” he said. “Maybe you took it away by not giving adequate treatment.”
Instead of testing and potentially cutting a first dose of curative therapy, “I err on the latter, acknowledging they will get sick,” he said. About 25 years ago, one of his patients died of 5-FU toxicity and “I regret that dearly,” he said. “But unhelpful information may lead us in the wrong direction.”
In September, seven months after his brother’s death, Kapoor was boarding a cruise ship on the Tyrrhenian Sea near Rome when he happened to meet a woman whose husband, Atlanta municipal judge Gary Markwell, had died the year before after taking a single 5-FU dose at age 77.
“I was like … that’s exactly what happened to my brother.”
Murray senses momentum toward mandatory testing. In 2022, the Oregon Health & Science University paid $1 million to settle a suit after an overdose death.
“What’s going to break that barrier is the lawsuits, and the big institutions like Dana-Farber who are implementing programs and seeing them succeed,” she said. “I think providers are going to feel kind of bullied into a corner. They’re going to continue to hear from families and they are going to have to do something about it.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.

Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What Seasonal Allergies Mean For Your Heart

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Most people associate seasonal allergies with itchy eyes and stuffy noses, but the effects can go a lot deeper.
This is because allergic reactions don’t just affect the respiratory system; they trigger chronic inflammation throughout the body, and in fact:
❝Allergic disease is a systemic and inflammatory condition❞
~ Dr. Rauno Joks, whose work we will cite in a moment
The important thing to understand in terms of heart health, is that chronic* systemic inflammation can contribute to coronary artery disease, where plaque buildup in arteries (bearing in mind, arterial plaque is in large part made of dead immune cells) raises the risk of heart attacks and strokes.
*Yes, a season once or twice per year counts as “chronic”.
A large (n=603,140) study found that allergic rhinitis (hay fever) increased the odds of coronary heart disease by 25% and heart attacks by 20%. Asthma, especially during flare-ups, posed an even greater risk:
Beyond biology
The effects aren’t just biological; allergies can limit physical activity, leading to a sedentary lifestyle that harms heart health.
In other words: if you’re not going outdoors because there’s pollen, and you’re not exercising because you’re exhausted, then the rest of your health is going to take a nose-dive (so to speak) too.
So, one more reason to take it seriously and not just dismiss it as “it’s just allergies, I’ll survive”.
Practical takeaways
Some things we can all do:
- Monitor your risk factors; i.e. keep on top of your heart health metrics, especially blood pressure and cholesterol, as well as any known genetic predisposition to cardiovascular disease.
- Watch out for alternative causes: symptoms like fatigue or shortness of breath may not always be allergies; they could signal asthma, reflux (for example if wheezing), or even heart disease. An allergist is a good first port-of-call, though.
- Be cautious with medications: some decongestants / allergy meds / asthma meds can raise blood pressure and/or interfere with other medications. Your pharmacist is the best person to speak to about this; they know this kind of thing much better than doctors, as a rule. And whenever you get a new medication, it is good practice to make a habit of always reading the information leaflet that comes with it, and/or look it up on a reputable website such as Drugs.com or the the BNF, to learn about what it is, how it works, what the risks are, what its contraindications are, etc.
- Don’t ignore warning signs: lightheadedness or chest pain could indicate a heart issue and should be addressed immediately. It’s better to be wrong and temporarily embarrassed, than wrong and permanently dead. Besides, even if it’s not a heart issue, it may be something else that would benefit from attention, so taking it seriously is always a good idea.
Want to know more?
Check out:
- What Your Mucus Says About Your Health
- Antihistamines’ Generation Gap
- Oh, Honey: The Bee’s Knees? ← what science has to say about “honey will inoculate you against allergies”
Take care!
Share This Post
-
Quercetin Quinoa Probiotic Salad
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This quercetin-rich salad is a bit like a tabbouleh in feel, with half of the ingredients switched out to maximize phenolic and gut-healthy benefits.
You will need
- ½ cup quinoa
- ½ cup kale, finely chopped
- ½ cup flat leaf parsley, finely chopped
- ½ cup green olives, thinly sliced
- ½ cup sun-dried tomatoes, roughly chopped
- 1 pomegranate, peel and pith removed
- 1 preserved lemon, finely chopped
- 1 oz feta cheese or plant-based equivalent, crumbled
- 1 tsp black pepper, coarse ground
- 1 tbsp capers
- 1 tbsp chia seeds
- 1 tbsp extra virgin olive oil
Note: you shouldn’t need salt or similar here, because of the diverse gut-healthy fermented products bringing their own salt with them
Method
(we suggest you read everything at least once before doing anything)
1) Rinse the quinoa, add the tbsp of chia seeds, cook as normal for quinoa (i.e. add hot water, bring to boil, simmer for 15 minutes or so until pearly and tender), carefully (don’t lose the chia seeds; use a sieve) drain and rinse with cold water to cool. Shake off excess water and/or pat dry on kitchen paper if necessary.
2) Mix everything gently but thoroughly.
3) Serve:

Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Tasty Tabbouleh with Tahini ← in case you want an actual tabbouleh
- Making Friends With Your Gut (You Can Thank Us Later)
- Fight Inflammation & Protect Your Brain, With Quercetin
Take care!
Share This Post
-

The Osteoporosis Breakthrough – by Dr. Doug Lucas
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“Osteoporosis” and “break” often don’t go well together, but here they do. So, what’s the breakthrough here?
There isn’t one, honestly. But if we overlook the marketing choices and focus on the book itself, the content here is genuinely good:
The book offers a comprehensive multivector approach to combatting osteoporosis, e.g:
- Diet
- Exercise
- Other lifestyle considerations
- Supplements
- Hormones
- Drugs
The author considers drugs a good and important tool for some people with osteoporosis, but not most. The majority of people, he considers, will do better without drugs—by tackling things more holistically.
The advice here is sound and covers all reasonable angles without getting hung up on the idea of there being a single magical solution for all.
Bottom line: if you’re looking for a book that’s a one-stop-shop for strategies against osteoporosis, this is a good option.
Click here to check out The Osteoporosis Breakthrough, and keep your bones strong!
Share This Post

Related Posts
-
Here’s how to help protect babies and kids from RSV
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What you need to know
- RSV is a respiratory virus that is especially dangerous for babies and young children.
- There are two ways to help protect babies from RSV: vaccination during pregnancy and giving babies nirsevimab, an RSV antibody shot.
- If someone in your household has RSV, watch for signs of severe illness and take steps to help prevent it from spreading.
Respiratory syncytial virus, or RSV, is a very contagious seasonal respiratory illness that is especially dangerous for infants and young children. Cases rose dramatically last month, and an increasing number of kids and older adults with RSV are being hospitalized across the United States.
Fortunately, pregnant people can get vaccinated during pregnancy or get their infants and young children an RSV antibody shot to help them stay healthy.
Read on to learn about symptoms of RSV, how to help prevent infants and children from getting very sick, and what families should do if someone in their household is sick with the virus.
What are the symptoms of RSV in babies and young children?
RSV symptoms in young children may include a runny nose, decreased eating and drinking, and coughing, which may lead to wheezing and difficulty breathing.
Infants with RSV may show symptoms like irritability, decreased activity and appetite, and life-threatening pauses in breathing (apnea) that last for more than 10 seconds. Most infants with RSV will not develop a fever, but babies who are born prematurely, have weakened immune systems, or have chronic lung disease are more likely to become very sick.
Who is eligible for an RSV antibody shot?
The Centers for Disease Control and Prevention recommends that babies younger than 8 months whose gestational parent did not receive an RSV vaccine during pregnancy receive nirsevimab between October and March, when RSV typically peaks. This antibody shot delivers proteins that can help protect them against RSV.
Nirsevimab is also recommended for children between 8 and 19 months who are at increased risk of severe RSV, including children who are born prematurely, have chronic lung disease or severe cystic fibrosis, are immunocompromised, or are American Indians or Alaska Natives.
Nirsevimab is typically covered by insurance or costs $495 out of pocket. Children who are eligible for the CDC’s Vaccines for Children Program can receive nirsevimab at no cost.
How can families help prevent RSV from spreading?
It’s recommended that children and adults who are sick with RSV stay home and away from others. If your infant or child has difficulty breathing or develops blue or gray skin, take them to an emergency room right away.
People who are infected with RSV can spread the disease when they cough or sneeze; have close contact with others; or touch, cough, or sneeze on shared surfaces. Help protect your family from catching and spreading RSV at home and in public places by ensuring that everyone covers their mouths during coughing and sneezing, washes their hands often, and wears a high-quality, well-fitting mask.
For more information, talk to your health care provider.
This article first appeared on Public Good News and is republished here under a Creative Commons license.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

A person in Texas caught bird flu after mixing with dairy cattle. Should we be worried?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The United States’ Centers for Disease Control and Prevention (CDC) has issued a health alert after the first case of H5N1 avian influenza, or bird flu, seemingly spread from a cow to a human.
A farm worker in Texas contracted the virus amid an outbreak in dairy cattle. This is the second human case in the US; a poultry worker tested positive in Colorado in 2022.
The virus strain identified in the Texan farm worker is not readily transmissible between humans and therefore not a pandemic threat. But it’s a significant development nonetheless.
Some background on bird flu
There are two types of avian influenza: highly pathogenic or low pathogenic, based on the level of disease the strain causes in birds. H5N1 is a highly pathogenic avian influenza.
H5N1 first emerged in 1997 in Hong Kong and then China in 2003, spreading through wild bird migration and poultry trading. It has caused periodic epidemics in poultry farms, with occasional human cases.
Influenza A viruses such as H5N1 are further divided into variants, called clades. The unique variant causing the current epidemic is H5N1 clade 2.3.4.4b, which emerged in late 2020 and is now widespread globally, especially in the Americas.
In the past, outbreaks could be controlled by culling of infected birds, and H5N1 would die down for a while. But this has become increasingly difficult due to escalating outbreaks since 2021.
Wild animals are now in the mix
Waterfowl (ducks, swans and geese) are the main global spreaders of avian flu, as they migrate across the world via specific routes that bypass Australia. The main hub for waterfowl to migrate around the world is Quinghai lake in China.
But there’s been an increasing number of infected non-waterfowl birds, such as true thrushes and raptors, which use different flyways. Worryingly, the infection has spread to Antarctica too, which means Australia is now at risk from different bird species which fly here.
H5N1 has escalated in an unprecedented fashion since 2021, and an increasing number of mammals including sea lions, goats, red foxes, coyotes, even domestic dogs and cats have become infected around the world.
Wild animals like red foxes which live in peri-urban areas are a possible new route of spread to farms, domestic pets and humans.
Dairy cows and goats have now become infected with H5N1 in at least 17 farms across seven US states.
What are the symptoms?
Globally, there have been 14 cases of H5N1 clade 2.3.4.4b virus in humans, and 889 H5N1 human cases overall since 2003.
Previous human cases have presented with a severe respiratory illness, but H5N1 2.3.4.4b is causing illness affecting other organs too, like the brain, eyes and liver.
For example, more recent cases have developed neurological complications including seizures, organ failure and stroke. It’s been estimated that around half of people infected with H5N1 will die.
The case in the Texan farm worker appears to be mild. This person presented with conjunctivitis, which is unusual.
Food safety
Contact with sick poultry is a key risk factor for human infection. Likewise, the farm worker in Texas was likely in close contact with the infected cattle.
The CDC advises pasteurised milk and well cooked eggs are safe. However, handling of infected meat or eggs in the process of cooking, or drinking unpasteurised milk, may pose a risk.
Although there’s no H5N1 in Australian poultry or cattle, hygienic food practices are always a good idea, as raw milk or poorly cooked meat, eggs or poultry can be contaminated with microbes such as salmonella and E Coli.
If it’s not a pandemic, why are we worried?
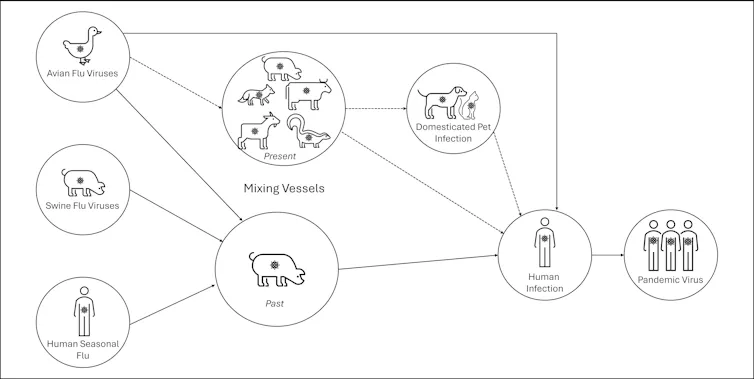
Scientists have feared avian influenza may cause a pandemic since about 2005. Avian flu viruses don’t easily spread in humans. But if an avian virus mutates to spread in humans, it can cause a pandemic.
One concern is if birds were to infect an animal like a pig, this acts as a genetic mixing vessel. In areas where humans and livestock exist in close proximity, for example farms, markets or even in homes with backyard poultry, the probability of bird and human flu strains mixing and mutating to cause a new pandemic strain is higher.
There are a number of potential pathways to a pandemic caused by influenza. Author provided The cows infected in Texas were tested because farmers noticed they were producing less milk. If beef cattle are similarly affected, it may not be as easily identified, and the economic loss to farmers may be a disincentive to test or report infections.
How can we prevent a pandemic?
For now there is no spread of H5N1 between humans, so there’s no immediate risk of a pandemic.
However, we now have unprecedented and persistent infection with H5N1 clade 2.3.4.4b in farms, wild animals and a wider range of wild birds than ever before, creating more chances for H5N1 to mutate and cause a pandemic.
Unlike the previous epidemiology of avian flu, where hot spots were in Asia, the new hot spots (and likely sites of emergence of a pandemic) are in the Americas, Europe or in Africa.
Pandemics grow exponentially, so early warnings for animal and human outbreaks are crucial. We can monitor infections using surveillance tools such as our EPIWATCH platform.
The earlier epidemics can be detected, the better the chance of stamping them out and rapidly developing vaccines.
Although there is a vaccine for birds, it has been largely avoided until recently because it’s only partially effective and can mask outbreaks. But it’s no longer feasible to control an outbreak by culling infected birds, so some countries like France began vaccinating poultry in 2023.
For humans, seasonal flu vaccines may provide a small amount of cross-protection, but for the best protection, vaccines need to be matched exactly to the pandemic strain, and this takes time. The 2009 flu pandemic started in May in Australia, but the vaccines were available in September, after the pandemic peak.
To reduce the risk of a pandemic, we must identify how H5N1 is spreading to so many mammalian species, what new wild bird pathways pose a risk, and monitor for early signs of outbreaks and illness in animals, birds and humans. Economic compensation for farmers is also crucial to ensure we detect all outbreaks and avoid compromising the food supply.
C Raina MacIntyre, Professor of Global Biosecurity, NHMRC L3 Research Fellow, Head, Biosecurity Program, Kirby Institute, UNSW Sydney; Ashley Quigley, Senior Research Associate, Global Biosecurity, UNSW Sydney; Haley Stone, PhD Candidate, Biosecurity Program, Kirby Institute, UNSW Sydney; Matthew Scotch, Associate Dean of Research and Professor of Biomedical Informatics, College of Health Solutions, Arizona State University, and Rebecca Dawson, Research Associate, The Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
How To Manage Your Mood With Food (8 Ways)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It is hard to be mentally healthy for long without good diet. Food can not only affect our mood directly, but also indirectly because of how our brain works (or doesn’t, if we don’t have the right nutrients, or it is being sabotaged in some other dietary fashion).
Selecting the food for setting the mood
Mind, the mental health charity, have these advices to share (with some bonus notes of our own):
- Eat regularly: blood sugar peaks and troughs can heighten feelings of tiredness, irritability, or depression. Instead, enjoy foods that are high in energy but low in glycemic index, such as nuts, seeds, and oats—that way you’ll have plenty of energy, that lasts longer.
- Choose the right fats: omega-3 fatty acids are essential for the brain. So are omega-6 fatty acids, but it is rare to have a deficiency in omega-6, and indeed, many people have the ratio of omega-3 to omega-6 far too imbalanced in omega-6’s favor. So, focussing on getting more omega-3 fatty acids is important. Nuts and seeds are again great, as are avocados, eggs, and oily fish.
- Get a healthy amount of protein: and importantly, with a good mix of amino acids—so a variety of sources of protein is best. In particular, if you are vegan, paying attention to ensure you get a full spread of amino acids is critical, as not many plants have all the ones we need (soy does, though). The reason this is important for mood is because many of those amino acids double up as the building blocks of neurotransmitters, so they’re not entirely interchangeable.
- Stay hydrated: our bodies are famously made of mostly water, and our brain will not work well if it’s dehydrated. The human body can squeeze water out of almost anything that has water in it, but water from food (such as fruit, or soups) is best. If enjoying actual drinks, then herbal teas are excellent for hydration.
- Eat a rainbow of fruits and vegetables: these have many nutrients that are important for brain health, and the point of the colors is that most of those pigments are themselves nutrients. Additionally, the fiber content of fruits and vegetables is of topmost important for your heart, and as you’ll remember (we say it often, because it’s true): what’s good for your heart is good for your brain.
- Limit caffeine intake: for many people, excess caffeine can lead to feelings of anxiety, disrupt your sleep, and for everyone who has developed an addiction to it, it will cause withdrawal symptoms if stopped abruptly. Cutting back on caffeine, or even eliminating it, may improve your mood and sleep quality. Note, however, that if you have ADHD, then your brain’s physiological relationship with caffeine is a little different, and stimulants will be more beneficial (and less deleterious) for you than for most people. If unsure, speak with your doctor about this one.
- Support your gut health: because of the gut-brain axis (via the vagal nerve), and also because nearly all of our endogenous serotonin is made in the gut (along with other neurotransmitters/hormones), getting plenty of fiber is important, and probiotics can help too.
- Consider food intolerances: if you know you have one, then keep that in mind and tailor your diet accordingly. If you suspect you have one, seek a nutritionist’s help to find out for sure. These can affect many aspects of health, including mood, so should not be dismissed as a triviality.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
The 6 Pillars Of Nutritional Psychiatry
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: