Can Saunas Make You Live Longer?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Max Levy explains:
When the heat is on…
In a traditional sauna with temperatures up to 90°C (194°F), heat sensors in the skin trigger the dilation of blood vessels and, simultaneously, faster heart rate. Skin temperature rises to around 41°C (106°F), and sweating helps release excess heat.
How it works: sauna heat stress resembles a moderate workout. Though not a substitute for exercise, regular use can strengthen the cardiovascular system and support recovery too. This is because like during exercise, muscle repair causes inflammation and waste buildup. Sauna-induced blood flow can also help deliver nutrients, remove waste, and balance inflammation for faster recovery.
About anti-aging properties more specifically: saunas increase levels of heat shock proteins, which repair DNA and maintain enzyme function. Normally with age, cells accumulate inflammatory damage. Evidence suggests sauna use can help regulate this process, but it’s surprisingly early days science-wise and there’s still a lot more experimenting to be done.
Spotlight study: in a study cited in the video, Finnish men who used saunas 4–7 times per week had lower risks of high blood pressure, improved cholesterol profiles, and reduced all-cause mortality. However, other lifestyle differences weren’t fully controlled for, and results may not be equally applicable to other demographics for a multitude of reasons (genetic adaptations, climate considerations, etc).
Caveat: obvious anything in the extreme can be dangerous, and saunas are by their very nature extreme (insofar as they deliver extreme heat). There are definitely some contraindications, including if you are pregnant, or on any number of medications that increase heat sensitivity. Talk with your doctor (and/or as applicable, pharmacist) first if unsure.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Saunas: Health Benefits (& Caveats)
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Spirulina vs Sun-Dried Tomatoes – Which is Healthier?

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing spirulina to sun-dried tomatoes, we picked the sun-dried tomatoes.
Why?
Both are great! But…
In terms of macros, spirulina has a tiny bit more protein, while sun-dried tomatoes have 12x the fiber for 9x the carbs, winning this round, mostly on account of the dodectuple fiber.
In the category of vitamins, spirulina has a tiny bit more of vitamins E and K, while sun-dried tomatoes have a lot more of vitamins A, B3, B5, B6, B9, and C, winning easily.
Looking at minerals, spirulina has a tiny bit more copper and iron, while sun-dried tomatoes have a lot more calcium, magnesium, manganese, phosphorus, potassium, selenium, and zinc, for another overwhelming win.
In other considerations, spirulina has no beneficial phytochemicals (because it is not a plant; it’s mostly a big colony of cyanobacteria), and unlike some seaweed, the B12 it does have is in an inactive form, while sun-dried tomatoes have abundant polyphenols, and also lycopene which is not be definition a polyphenol (it’s a carotenoid), but does a similar job and is a very potent antioxidant. In any case, this category is one more win for sun-dried tomatoes.
Lest this all seem very damning for spirulina, we’ll take a moment to reiterate that spirulina is very nutritionally dense, and it only looks bad here because it’s standing next to sun-dried tomatoes which are better in almost every way.
Nevertheless, adding up the sections does make for a very clear overall win for sun-dried tomatoes, so, enjoy!
Want to learn more?
You might like:
Enjoy!
Share This Post
-

Stretching & Mobility – by James Atkinson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
“I will stretch for just 10 minutes per day”, we think, and do our best. Then there are a plethora of videos saying “Stretching mistakes that you are making!” and it turns out we haven’t been doing them in a way that actually helps.
This book fixes that. Unlike some books of the genre, it’s not full of jargon and you won’t need an anatomy and physiology degree to understand it. It is, however, dense in terms of the information it gives—it’s not padded out at all; it contains a lot of value.
The stretches are all well-explained and well-illustrated; the cover art will give you an idea of the anatomical illustration style contained with in.
Atkinson also gives workout plans, so that we know we’re not over- or under-training or trying to do too much or missing important things out.
Bottom line: if you’re looking to start a New Year routine to develop better suppleness, this book is a great primer for that.
Click here to check out Stretching and Mobility, and improve yours!
Share This Post
-
How Old Is Too Old For HRT?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I think you guys do a great job. Wondering if I can suggest a topic? Older women who were not offered hormone replacement therepy because of a long term study that was misread. Now, we need science to tell us if we are too old to benefit from begininng to take HRT. Not sure how old your readers are on average but it would be a great topic for older woman. Thanks❞
Thank you for the kind words, and the topic suggestion!
About the menopause and older age thereafter
We’ve talked a bit before about the menopause, for example:
What You Should Have Been Told About The Menopause Beforehand
And we’ve even discussed the unfortunate social phenomenon of post-menopausal women thinking “well, that’s over and done with now, time to forget about that”, because spoiler, it will never be over and done with—your body is always changing every day, and will continue to do so until you no longer have a body to change.
This means, therefore, that since changes are going to happen no matter what, the onus is on us to make the changes as positive (rather than negative) as possible:
Menopause, & When Not To Let Your Guard Down
About cancer risk
It sounds like you know this one, but for any who were unaware: indeed, there was an incredibly overblown and misrepresented study, and even that was about older forms of HRT (being conjugated equine estrogens, instead of bioidentical estradiol):
As for those who have previously had breast cancer or similar, there is also:
The Hormone Therapy That Reduces Breast Cancer Risk & More
Is it too late?
Fortunately, there is a quick and easy test to know whether you are too old to benefit:
First, find your pulse, by touching the first two fingers of one hand, against the wrist of the other. If you’re unfamiliar with where to find the pulse at the wrist, here’s a quick explainer.
Or if you prefer a video:
Click Here If The Embedded Video Doesn’t Load Automatically!
Did you find it?
Good; in that case, it’s not too late!
Scientists have tackled this question, looking at women of various ages, and finding that when comparing age groups taking HRT, disease risk changes do not generally vary much by age i.e., someone at 80 gets the same relative benefit from HRT as someone at 50, with no extra risks from the HRT. For example, if taking HRT at 50 reduces a risk by n% compared to an otherwise similar 50-year-old not on HRT, then doing so at 80 reduces the same risk by approximately the same percentage, compared to an otherwise similar 80-year-old not on HRT.
There are a couple of exceptions, such as in the case of already having advanced atherosclerotic lesions (in which specific case HRT could increase inflammation; not something it usually does), or in the case of using conjugated equine estrogens instead of modern bioidentical estradiol (as we talked about before).
Thus, for the most part, HRT is considered safe and effective regardless of age:
How old is too old for hormone therapy?
👆 that’s from 2015 though, so how about a new study, from 2024?
❝Compared with never use or discontinuation of menopausal hormone therapy after age 65 years, the use of estrogen monotherapy beyond age 65 years was associated with significant risk reductions in mortality (19% or adjusted hazards ratio, 0.81; 95% CI, 0.79-0.82), breast cancer (16%), lung cancer (13%), colorectal cancer (12%), congestive heart failure (CHF) (5%), venous thromboembolism (3%), atrial fibrillation (4%), acute myocardial infarction (11%), and dementia (2%).❞
❝Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with estradiol rather than conjugated estrogen.❞
Read in full: Use of menopausal hormone therapy beyond age 65 years and its effects on women’s health outcomes by types, routes, and doses
As for more immediately-enjoyable benefits (improved mood, healthier skin, better sexual function, etc), yes, those also are benefits that people enjoy at least into their eighth decade:
See: Use of hormone therapy in Swedish women aged 80 years or older
What about…
Statistically speaking, most people who take HRT have a great time with it and consider it life-changing in a good way. However, nothing is perfect; sometimes going on HRT can have a shaky start, and for those people, there may be some things that need addressing. So for that, check out:
HRT Side Effects & Troubleshooting
And also, while estrogen monotherapy is very common, it is absolutely worthwhile to consider also taking progesterone alongside it:
Progesterone Menopausal HRT: When, Why, And How To Benefit
Enjoy!
Share This Post

Related Posts
-

The Aesthetic Brain – by Dr. Anjan Chatterjee
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Dr. Anjan Chatterjee (not to be mistaken for Dr. Rangan Chatterjee, whose books we have also sometimes reviewed before) is a neurologist.
A lot about aesthetics is easy enough to understand. We like physical features in humans that suggest a healthy mate, and we like lush and/or colorful plants that reassure us that we will have plenty to eat.
But what about a beautiful building, or a charcoal drawing of some captivatingly eldritch horror? And what, neurologically speaking, is the difference between a bowl of fruit and a painting of a bowl of fruit? And what, if anything, does appreciation of such do for us?
In this very readable pop-science book, we learn about these things and many more, from the perspective of an experienced neurologist who explains things simply but with plenty of science.
Bottom line: if you’d like to understand how and why your brain does more things than just process tasks necessary for survival, this book will give you plenty of insight.
Click here to check out The Aesthetic Brain, and learn more about yours!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Severe irritability in teens can be reduced by daily doses of vitamins and minerals, new research
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Irritability is one of the most common and distressing problems teenagers and their families face.
Its main symptom is an excessive reaction to negative emotional stimuli, resulting in temper outbursts and severe irritable mood.
While current treatment options such as psychotherapy and medications are helpful for some, they can be inaccessible or poorly tolerated.
Our new research, based on a double-blinded, placebo-controlled clinical trial, shows broad-spectrum micronutrients (vitamins and minerals) can significantly reduce severe irritability in teenagers. Teens with severely disruptive behaviour experienced especially large improvements.
This offers a safe, scalable and biologically grounded alternative to conventional psychiatric treatments.

Getty Images Urgent need for more effective treatments
Irritability cuts across many psychiatric presentations, including anxiety, depression, attention deficit/hyperactivity disorder (ADHD) and other disruptive behaviour disorders.
The need for interventions that directly target irritability, have fewer side effects and are available to all communities is urgent.
Statistics on mental health in young people are especially concerning. Youth mental health has been declining globally over the past two decades and has now reached a “dangerous phase”, according to a Lancet commission.
Despite this, research consistently highlights a lack of effective and accessible treatments for severely irritable youth. This suggests a significant unmet public health need.
Our research findings are based on the Balancing Emotions of Adolescents with Micronutrients (BEAM) trial, in which 132 unmedicated teenagers (aged 12 to 17) with moderate to severe irritability were randomly assigned to micronutrients (taken as four pills three times a day) or an active placebo for eight weeks. They were monitored monthly online by a clinical psychologist.
The placebo response was high, suggesting that simply participating in the study helped many teens feel able to improve their behaviour. But micronutrients still outperformed the placebo across key clinical measures such as irritability, emotional reactivity and overall improvement.
We saw the strongest effects in teenagers with disruptive mood dysregulation disorder (DMDD), with 64% responding to micronutrients compared to 12.5% on placebo. This demonstrates an unusually large effect for a psychiatric intervention.
Parents of participants receiving micronutrients rated the teens’ conduct and prosocial behaviour much higher compared with those of teens on placebo.
Micronutrient treatment was also associated with more rapid improvements in clinician‑rated irritability, parent‑reported dysphoria and teen‑reported quality of life, stress and prosocial behaviours.
One of the most notable and reassuring findings was that suicidal ideation, which about a quarter of study participants reported at the start of the trial, improved over time for both groups, but with a greater change for teens on micronutrients. Self-harm behaviour also decreased for both groups.
Only one side effect differed significantly between groups: diarrhoea was more common on micronutrients (20.9%) than placebo (6.2%). But this side effect was typically temporary and resolved by taking the nutrients with food and water.
A minority (fewer than 10%) found swallowing pills a challenge. Other side effects reported equally in both groups included occasional headaches, stomach aches or a dry mouth. These tended to dissipate within the first few weeks.
Socioeconomic background matters
The response to treatment was moderated by the teens’ socioeconomic status.
Participants from lower socioeconomic backgrounds were more likely to benefit from micronutrients. This is particularly meaningful for both clinical practice and public health.
Lower socioeconomic status is typically associated with greater exposure to nutritional insufficiencies, chronic stress, reduced access to health services and higher rates of mental health difficulties.
Our findings suggest micronutrients may help address underlying nutritional vulnerabilities that may be more prevalent or more severe in disadvantaged groups.
This pattern also indicates that micronutrient supplementation, if publicly funded, could function as a low‑cost, scalable intervention, with the potential to reduce health inequities.
Many evidence‑based psychosocial or pharmacological treatments require resources – time, transportation, specialist access – that disproportionately disadvantage lower‑income families.
In our trial, all meetings between the psychologist and the teen with their family were conducted online and the micronutrients were couriered across the country, making this intervention accessible, particularly to rural communities.
Micronutrients may represent an intervention that is both accessible and responsive to the specific needs of youth who are most at risk yet often least well served by traditional care pathways.
This study was developed alongside Māori health providers and fits within a tikanga (traditional) Māori framework. It had a high percentage of Māori participants (27%) and worked closely with them, their families and health providers to assist in improving mental health outcomes.
The BEAM trial provides robust evidence that a simple nutritional approach can meaningfully improve symptoms, including emotional reactivity, conduct difficulties and even suicidal ideation.
These results are relevant for parents, clinicians, teachers and policymakers seeking safe and practical interventions, especially for young people who cannot access or do not respond well to existing treatments. The results also highlight important equity implications, as teens from lower income families showed stronger responses.
Our results cast a new lens on the cause of some psychiatric problems, often conceptualised as chemical imbalances or family dysfunction. They reframe some cases of irritability as a possible nutritional and metabolic vulnerability, one that might be addressed with greater attention to the quality of our food alongside some supplementation with broad-spectrum micronutrients.
Julia J Rucklidge, Professor of Psychology, University of Canterbury; Angela Sherwin, PhD Candidate in Psychology, University of Canterbury; Joseph Boden, Professor of Psychology, Director of the Christchurch Health and Development Study, University of Otago, and Roger Mulder, Professor of Psychiatry, University of Otago
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between miscarriage and stillbirth?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What’s the difference? is a new editorial product that explains the similarities and differences between commonly confused health and medical terms, and why they matter.
Former US First Lady Michelle Obama revealed in her memoir she had a miscarriage. UK singer-songwriter and actor Lily Allen has gone on the record about her stillbirth.
Both miscarriage and stillbirth are sadly familiar terms for pregnancy loss. They can be traumatic life events for the prospective parents and family, and their impacts can be long-lasting. But the terms can be confused.
Here are some similarities and differences between miscarriage and stillbirth, and why they matter.
christinarosepix/Shutterstock Let’s start with some definitions
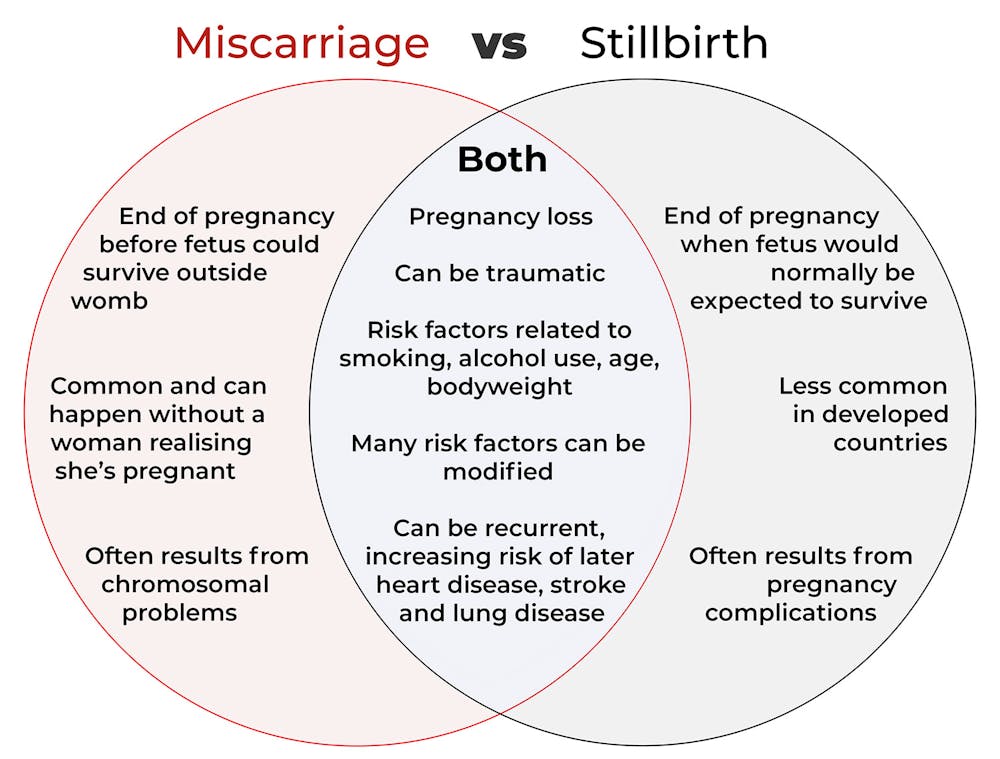
In broad terms, a miscarriage is when a pregnancy ends while the fetus is not yet viable (before it could survive outside the womb).
This is the loss of an “intra-uterine” pregnancy, when an embryo is implanted in the womb to then develop into a fetus. The term miscarriage excludes ectopic pregnancies, where the embryo is implanted outside the womb.
However, stillbirth refers to the end of a pregnancy when the fetus is normally viable. There may have been sufficient time into the pregnancy. Alternatively, the fetus may have grown large enough to be normally expected to survive, but it dies in the womb or during delivery.
The Australian Institute of Health and Welfare defines stillbirth as a fetal death of at least 20 completed weeks of gestation or with a birthweight of at least 400 grams.
Internationally, definitions of stillbirth vary depending on the jurisdiction.
How common are they?
It is difficult to know how common miscarriages are as they can happen when a woman doesn’t know she is pregnant. There may be no obvious symptoms or something that looks like a heavier-than-normal period. So miscarriages are likely to be more common than reported.
Studies from Europe and North America suggest a miscarriage occurs in about one in seven pregnancies (15%). More than one in eight women (13%) will have a miscarriage at some time in her life.
Around 1–2% of women have recurrent miscarriages. In Australia this is when someone has three or more miscarriages with no pregnancy in between.
Australia has one of the lowest rates of stillbirth in the world. The rate has been relatively steady over the past 20 years at 0.7% or around seven per 1,000 pregnancies.
Who’s at risk?
Someone who has already had a miscarriage or stillbirth has an increased risk of that outcome again in a subsequent pregnancy.
Compared with women who have had a live birth, those who have had a stillbirth have double the risk of another. For those who have had recurrent miscarriages, the risk of another miscarriage is four-fold higher.
Some factors have a u-shaped relationship, with the risk of miscarriage and stillbirth lowest in the middle.
For instance, maternal age is a risk factor for both miscarriage and stillbirth, especially if under 20 years old or older than 35. Increasing age of the male is only a risk factor for stillbirth, especially for fathers over 40.
An older dad can be a risk factor for stillbirth, but not miscarriage. Elizaveta Galitckaia/Shutterstock Similarly for maternal bodyweight, women with a body mass index or BMI in the normal range have the lowest risk of miscarriage and stillbirth compared with those in the obese or underweight categories.
Lifestyle factors such as smoking and heavy alcohol drinking while pregnant are also risk factors for both miscarriage and stillbirth.
So it’s important to not only avoid smoking and alcohol while pregnant, but before getting pregnant. This is because early in the pregnancy, women may not know they have conceived and could unwittingly expose the developing fetus.
Why do they happen?
Miscarriage often results from chromosomal problems in the developing fetus. However, genetic conditions or birth defects account for only 7-14% of stillbirths.
Instead, stillbirths often relate directly to pregnancy complications, such as a prolonged pregnancy or problems with the umbilical cord.
Maternal health at the time of pregnancy is another contributing factor in the risk of both miscarriage and stillbirths.
Chronic diseases, such as high blood pressure, diabetes, hypothyroidism (underactive thyroid), polycystic ovary syndrome, problems with the immune system (such as an autoimmune disorder), and some bacterial and viral infections are among factors that can increase the risk of miscarriage.
Similarly mothers with diabetes, high blood pressure, and untreated infections, such as malaria or syphilis, face an increased risk of stillbirth.
In many cases, however, the specific cause of pregnancy loss is not known.
How about the long-term health risks?
Miscarriage and stillbirth can be early indicators of health issues later in life.
For instance, women who have had recurrent miscarriages or recurrent stillbirths are at higher risk of cardiovascular disease (such as heart disease or stroke).
Our research has also looked at the increased risk of stroke. Compared with women who had never miscarried, we found women with a history of three or more miscarriages had a 35% higher risk of non-fatal stroke and 82% higher risk of fatal stroke.
Women who had a stillbirth had a 31% higher risk of a non-fatal stroke, and those who had had two or more stillbirths were at a 26% higher risk of a fatal stroke.
We saw similar patterns in chronic obstructive pulmonary disease or COPD, a progressive lung disease with respiratory symptoms such as breathlessness and coughing.
Our data showed women with a history of recurrent miscarriages or stillbirths were at a 36% or 67% higher risk of COPD, respectively, even after accounting for a history of asthma.
Long-term health risks of recurrent miscarriages or stillbirths include developing lung disease later in life. PRPicturesProduction/Shutterstock Why is all this important?
Being well-informed about the similarities and differences between these two traumatic life events may help explain what has happened to you or a loved one.
Where risk factors can be modified, such as smoking and obesity, this information can be empowering for individuals who wish to reduce their risk of miscarriage and stillbirth and make lifestyle changes before they become pregnant.
More information and support about miscarriage and stillbirth is available from SANDS and Pink Elephants.
Gita Mishra, Professor of Life Course Epidemiology, Faculty of Medicine, The University of Queensland; Chen Liang, PhD student, reproductive history and non-communicable diseases in women, The University of Queensland, and Jenny Doust, Clinical Professorial Research Fellow, School of Public Health, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: