Bright Line Eating – by Dr. Susan Peirce Thompson
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a great title! It’s a great book too, but let’s talk about the title for a moment:
The “Bright Line” referenced (often used in the plural within the book) is the line one draws between what one will and will not do. It’s a line one doesn’t cross, and it’s a bright line, because it’s not a case of “oh woe is me I cannot have the thing”, but rather “oh yay is me for I being joyously healthy”.
And as for living happy, thin, and free? The author makes clear that “thin” is only a laudable goal if it’s bookended by “happy” and “free”. Eating things because we want to, and being happy about our choices.
To this end, while some of the book is about nutrition (and for example the strong recommendation to make the first “bright lines” one draws cutting out sugar and flour), the majority of it is about the psychology of eating.
This includes, hunger and satiety, willpower and lack thereof, disordered eating and addictions, body image issues and social considerations, the works. She realizes and explains, that if being healthy were just a matter of the right diet plan, everyone would be healthy. But it’s not; our eating behaviors don’t exist in a vacuum, and there’s a lot more to consider.
Despite all the odds, however, this is a cheerful and uplifting book throughout, while dispensing very practical, well-evidenced methods for getting your brain to get your body to do what you want it to.
Bottom line: this isn’t your average diet book, and it’s not just a motivational pep talk either. It’s an enjoyable read that’s also full of science and can make a huge difference to how you see food.
Click here to check out Bright Line Eating, and enjoy life, healthily!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Why it’s a bad idea to mix alcohol with some medications

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anyone who has drunk alcohol will be familiar with how easily it can lower your social inhibitions and let you do things you wouldn’t normally do.
But you may not be aware that mixing certain medicines with alcohol can increase the effects and put you at risk.
When you mix alcohol with medicines, whether prescription or over-the-counter, the medicines can increase the effects of the alcohol or the alcohol can increase the side-effects of the drug. Sometimes it can also result in all new side-effects.
How alcohol and medicines interact
The chemicals in your brain maintain a delicate balance between excitation and inhibition. Too much excitation can lead to convulsions. Too much inhibition and you will experience effects like sedation and depression.
Alcohol works by increasing the amount of inhibition in the brain. You might recognise this as a sense of relaxation and a lowering of social inhibitions when you’ve had a couple of alcoholic drinks.
With even more alcohol, you will notice you can’t coordinate your muscles as well, you might slur your speech, become dizzy, forget things that have happened, and even fall asleep.

Alcohol can affect the way a medicine works.
Jonathan Kemper/UnsplashMedications can interact with alcohol to produce different or increased effects. Alcohol can interfere with the way a medicine works in the body, or it can interfere with the way a medicine is absorbed from the stomach. If your medicine has similar side-effects as being drunk, those effects can be compounded.
Not all the side-effects need to be alcohol-like. Mixing alcohol with the ADHD medicine ritalin, for example, can increase the drug’s effect on the heart, increasing your heart rate and the risk of a heart attack.
Combining alcohol with ibuprofen can lead to a higher risk of stomach upsets and stomach bleeds.
Alcohol can increase the break-down of certain medicines, such as opioids, cannabis, seizures, and even ritalin. This can make the medicine less effective. Alcohol can also alter the pathway of how a medicine is broken down, potentially creating toxic chemicals that can cause serious liver complications. This is a particular problem with paracetamol.
At its worst, the consequences of mixing alcohol and medicines can be fatal. Combining a medicine that acts on the brain with alcohol may make driving a car or operating heavy machinery difficult and lead to a serious accident.
Who is at most risk?
The effects of mixing alcohol and medicine are not the same for everyone. Those most at risk of an interaction are older people, women and people with a smaller body size.
Older people do not break down medicines as quickly as younger people, and are often on more than one medication.
Older people also are more sensitive to the effects of medications acting on the brain and will experience more side-effects, such as dizziness and falls.
Smaller and older people are often more affected.
Alfonso Scarpa/UnsplashWomen and people with smaller body size tend to have a higher blood alcohol concentration when they consume the same amount of alcohol as someone larger. This is because there is less water in their bodies that can mix with the alcohol.
What drugs can’t you mix with alcohol?
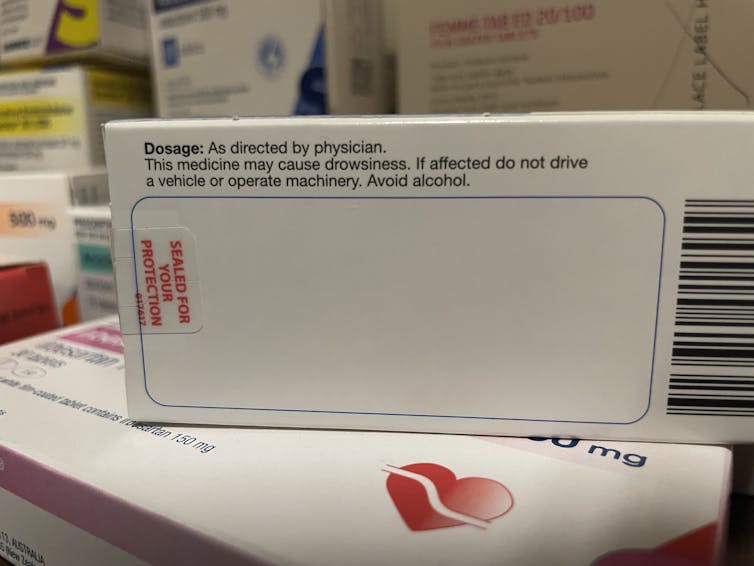
You’ll know if you can’t take alcohol because there will be a prominent warning on the box. Your pharmacist should also counsel you on your medicine when you pick up your script.
The most common alcohol-interacting prescription medicines are benzodiazepines (for anxiety, insomnia, or seizures), opioids for pain, antidepressants, antipsychotics, and some antibiotics, like metronidazole and tinidazole.
Medicines will carry a warning if you shouldn’t take them with alcohol.
Nial WheateIt’s not just prescription medicines that shouldn’t be mixed with alcohol. Some over-the-counter medicines that you shouldn’t combine with alcohol include medicines for sleeping, travel sickness, cold and flu, allergy, and pain.
Next time you pick up a medicine from your pharmacist or buy one from the local supermarket, check the packaging and ask for advice about whether you can consume alcohol while taking it.
If you do want to drink alcohol while being on medication, discuss it with your doctor or pharmacist first.

Nial Wheate, Associate Professor of the School of Pharmacy, University of Sydney; Jasmine Lee, Pharmacist and PhD Candidate, University of Sydney; Kellie Charles, Associate Professor in Pharmacology, University of Sydney, and Tina Hinton, Associate Professor of Pharmacology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

10 Unsexy (But Lifechanging) Tips
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you don’t want your efforts to go to waste, these tips will help you make sure everything’s at least a slight improvement—and then the same again the next day!
Bit by bit
If you have the right approach to these things, the rest will fall into place by itself:
- Like vs want/need: what feels good isn’t always what you want or need; progress often requires uncomfortable new habits that align with your goals/desires rather than your immediate inclinations. You may not enjoy every action, but you’ll like the results that come from them.
- Train hard if you want, but rest well: you can only train as hard as you can recover; burnout usually comes from under-recovering, not from overtraining. So, prioritize sleep, nutrition, and mobility work before changing your workouts.
- Eat more: sustainable fat loss comes from small calorie deficits at most, not starvation. Extreme or long-term restriction slows your metabolism, minimizes fat loss, and leads to rebound weight gain. Fuel your body properly so you can look leaner, feel energized, and maintain your results.
- Fearing carbs/fat: don’t demonize any macronutrient; both carbs and fats are essential for energy, hormones, and metabolism. Your ideal balance will change with your goals, activity, and life stage, so stay adaptable. If in doubt, follow your gut, and just make sure to get plenty of fiber either way.
- Don’t “set and forget”: there’s no one perfect “lifestyle”; our goals, body, and routines will evolve, so your nutrition and workouts must too. True progress comes from constant small adjustments and long-term consistency.
- Daily mobility: do the boring mobility work—foam roll, stretch, and activate—every day. A few minutes of “prehab” prevents injuries, improves performance, and keeps you training pain-free as you age.
- Don’t blame circumstances: even if it’s true! You can’t control everything, but you can always control your response. Focus on solutions, not the negatives, to keep moving forwards.
- Don’t define yourself by specific routines or labels: as you grow and your goals change, your habits should too. Evolving your approach is a sign of progress, not failure.
- Slow down to speed up: when life gets busy, doing something is better than doing nothing. A few workouts or partial effort still move you forwards; perfectionism only keeps you stuck.
- Track things the easy way: measure what you do so you can manage it. Using apps for this gives you clarity, direction, and the ability to adjust intelligently instead of guessing.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
How To Actually Get Abs (10 Annoying Tips That Work!)
Take care!
Share This Post
-

Stop Cancer 20 Years Ago
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Get Abreast And Keep Abreast

This is Dr. Jenn Simmons. Her specialization is integrative oncology, as she—then a breast cancer surgeon—got breast cancer, decided the system wasn’t nearly as good from the patients’ side of things as from the doctors’ side, and took to educate herself, and now others, on how things can be better.
What does she want us to know?
Start now
If you have breast cancer, the best time to start adjusting your lifestyle might be 20 years ago, but the second-best time is now. We realize our readers with breast cancer (or a history thereof) probably have indeed started already—all strength to you.
What this means for those of us without breast cancer (or a history therof) is: start now
Even if you don’t have a genetic risk factor, even if there’s no history of it in your family, there’s just no reason not to start now.
Start what, you ask? Taking away its roots. And how?
Inflammation as the root of cancer
To oversimplify: cancer occurs because an accidentally immortal cell replicates and replicates and replicates and takes any nearby resources to keep on going. While science doesn’t know all the details of how this happens, it is a factor of genetic mutation (itself a normal process, without which evolution would be impossible), something which in turn is accelerated by damage to the DNA. The damage to the DNA? That occurs (often as not) as a result of cellular oxidation. Cellular oxidation is far from the only genotoxic thing out there, and a lot of non-food “this thing causes cancer” warnings are usually about other kinds of genotoxicity. But cellular oxidation is a big one, and it’s one that we can fight vigorously with our lifestyle.
Because cellular oxidation and inflammation go hand-in-hand, reducing one tends to reduce the other. That’s why so often you’ll see in our Research Review Monday features, a line that goes something like:
“and now for those things that usually come together: antioxidant, anti-inflammatory, anticancer, and anti-aging”
So, fight inflammation now, and have a reduced risk of a lot of other woes later.
See: How to Prevent (or Reduce) Inflammation
Don’t settle for “normal”
People are told, correctly but not always helpfully, such things as:
- It’s normal to have less energy at your age
- It’s normal to have a weaker immune system at your age
- It’s normal to be at a higher risk of diabetes, heart disease, etc
…and many more. And these things are true! But that doesn’t mean we have to settle for them.
We can be all the way over on the healthy end of the distribution curve. We can do that!
(so can everyone else, given sufficient opportunity and resources, because health is not a zero-sum game)
If we’re going to get a cancer diagnosis, then our 60s are the decade where we’re most likely to get it. Earlier than that and the risk is extant but lower; later than that and technically the risk increases, but we probably got it already in our 60s.
So, if we be younger than 60, then now’s a good time to prepare to hit the ground running when we get there. And if we missed that chance, then again, the second-best time is now:
See: Focusing On Health In Our Sixties
Fast to live
Of course, anything can happen to anyone at any age (alas), but this is about the benefits of living a fasting lifestyle—that is to say, not just fasting for a 4-week health kick or something, but making it one’s “new normal” and just continuing it for life.
This doesn’t mean “never eat”, of course, but it does mean “practice intermittent fasting, if you can”—something that Dr. Simmons strongly advocates.
See: Intermittent Fasting: We Sort The Science From The Hype
While this calls back to the previous “fight inflammation”, it deserves its own mention here as a very specific way of fighting it.
It’s never too late
All of the advices that go before a cancer diagnosis, continue to stand afterwards too. There is no point of “well, I already have cancer, so what’s the harm in…?”
The harm in it after a diagnosis will be the same as the harm before. When it comes to lifestyle, preventing a cancer and preventing it from spreading are very much the same thing, which is also the same as shrinking it. Basically, if it’s anticancer, it’s anticancer, no matter whether it’s before, during, or after.
Dr. Simmons has seen too many patients get a diagnosis, and place their lives squarely in the hands of doctors, when doctors can only do so much.
Instead, Dr. Simmons recommends taking charge of your health as best you are able, today and onwards, no matter what. And that means two things:
- Knowing stuff
- Doing stuff
So it becomes our responsibility (and our lifeline) to educate ourselves, and take action accordingly.
Want to know more?
We recently reviewed her book, and heartily recommend it:
The Smart Woman’s Guide to Breast Cancer – by Dr. Jenn Simmons
Enjoy!
Share This Post




Related Posts
-
Unsafe and unethical: bed shortages mean dementia patients with psychiatric symptoms are admitted to medical wards
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
New Zealand’s mental health crisis is well documented in the government’s 2018 inquiry, He Ara Oranga, which shows one in five people experience mental illness or significant mental distress.
However, an almost singular focus on care of young people obscures the psychiatric needs of older adults.
Failure to account for these needs has resulted in physicians facing pressure to admit psychiatric patients to medical wards that are not designed or resourced to care for them. This compromises patient safety and rights as well as fundamental standards of care.
Our new research highlights the clinical, ethical and legal consequences of this practice and calls for urgent action.
Getty Images Dementia includes psychiatric features
The memory deficits of dementia are well known but the condition also includes psychiatric presentations. These are known collectively as the “behavioural and psychiatric symptoms of dementia” (BPSD). When severe, they can include intrusive behaviour, violence and inappropriate sexual conduct. Such patients require admission and specialist treatment.
However, New Zealand has a severe shortage of psychiatric beds for older adults. Even more concerning is that despite well recognised demographic trends and clinical concerns, bed numbers have decreased over time rather than increased.
Reports that Dunedin plans to slash the number of psycho-geriatric beds by 50% reflect a lack of government insight into the risks this large and growing patient cohort poses.
Hospitals routinely expect medical wards to admit dementia patients presenting with BPSD when no psycho-geriatric bed is available. Yet it is impossible for staff on medical wards to adhere to even basic standards of care.
Poor design
A lack of single rooms means medical teams cannot provide the security and minimisation of light and noise people with dementia require. Single rooms need to be prioritised for transmissible infections, delirium and terminal care.
Medical wards are also not designed for aggressive patients. People can enter and exit freely, potential weapons (scissors, for example) are accessible, there are no seclusion rooms or low-stimulus areas, and nursing stations are not secure.
Medical staff are not trained in de-escalation or restraint and ward pharmacists are not specialised in the medications required to treat BPSD.
Those presenting with physical or sexual violence also need dedicated security, well beyond what healthcare assistants on “patient watches” can provide. Most healthcare assistants are women, which creates a grossly inadequate level of safety when managing violent male patients.
The experience of Wellington general medicine staff documents numerous assaults on nurses and intrusive and frightening behaviour. Staff have been punched, hit, bitten and threatened. One nurse was stabbed while attending to another patient in a multi-bed room.
Admissions have included physically robust patients who have seriously assaulted family or carers. This includes one man who committed a fatal assault and another who was sexually aggressive and stabbed a family member.
High rates of mixed-gender bedding in hospital wards raise the risk of harm. The United Kingdom banned hospitals from placing men and women in the same room in 2010. Yet despite concerns for patient safety, New Zealand has no prohibition on this practice.
Poor policy
By comparison, Australia proposed a risk stratification approach more than 20 years ago whereby severe dementia patients would be managed in secure units with dedicated security staff and specialist psycho-geriatric care.
This model is used throughout Australia in policy and planning. In New Zealand, severe dementia is defaulted to medical wards even in cases where patients are presenting solely due to extreme violence.
According to the Code of Health and Disability Services Consumers’ Rights, patients are entitled to an appropriate standard of care. Admitting someone with dementia to medical wards that cannot meet basic standards of care clearly breaches this right.
BPSD admissions also significantly compromise the rights of other patients. The risks are again demonstrable rather than potential. International media reports have documented male dementia patients assaulting female patients in medical wards without the necessary security measures.
Medical staff in New Zealand hospitals have also witnessed numerous incidents of intrusion and harassment as well as assaults of other patients by dementia patients inappropriately admitted to medical wards with BPSD.
We should also recognise indirect impacts of people with severe dementia being admitted on medical wards. Many patients wait overnight for admission, increasing their risk for complications, and breaching rights to privacy and dignity.
When psychiatric patients occupy medical beds, they contribute to admission delays, complications and rights breaches for medical patients awaiting beds.
Urgent need for more psycho-geriatric beds
Wellington general medicine teams have raised serious concerns about dementia admissions for many years. Yet there are no secure areas and no additional psycho-geriatric beds.
We need to ask why the practice continues when harm is so obvious. The answer appears to be about cost. When physicians relent and admit psychiatric patients, the risks are high but the financial cost is low. The consequences are born by elderly and frail patients seldom able to advocate for themselves.
Change relies on health leaders and funders caring about safety, rights and basic standards of care. Unfortunately, the Wellington experience and the decision to cut beds in Dunedin suggest change will not happen unless physicians consistently refuse the admission of psychiatric patients. But this is a morally distressing position to be put in.
New Zealand must urgently address the shortage of psycho-geriatric beds. Until these are in place, temporary secure accommodation must be made available under the care of mental health specialists.
Medical teams can no longer be expected to manage the mental health crisis as well as their own medical workloads. It is unsafe, unethical and untenable for all involved.
Cindy Towns, Senior Lecturer in Geriatrics and Clinical Ethics, University of Otago
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Power Plates – by Gena Hamshaw
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Superfoods are all well and good, but there are only so many ways one can reasonably include watercress before it starts becoming a chore.
Happily, Gena Hamshaw is here with a hundred single-dish vegan meals, that are not only nutritionally balanced as the subtitle promises, but also, as the title suggests, are nutritional powerhouses too.
In the category of criticism, some ingredients are not so universally available as others. For example, depending on where you live, your local supermarket might not have freekeh, gochujang, or pomegranate molasses.
However, most of the recipes have ingredients that are easy enough to source in any medium-sized supermarket, and for the ones that aren’t, we do recommend ordering the ingredient online and trying something you might not otherwise have experienced—that’s an important thing in life, after all!
Bottom line: if you’d like plant-based meals that are packed full of nutrients and are delicious too, this is a top-tier recipe book.
Click here to check out Power Plates, and enjoy a wide variety of plant-based cuisine!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

If I’m diagnosed with one cancer, am I likely to get another?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Receiving a cancer diagnosis is life-changing and can cause a range of concerns about ongoing health.
Fear of cancer returning is one of the top health concerns. And managing this fear is an important part of cancer treatment.
But how likely is it to get cancer for a second time?
Why can cancer return?
While initial cancer treatment may seem successful, sometimes a few cancer cells remain dormant. Over time, these cancer cells can grow again and may start to cause symptoms.
This is known as cancer recurrence: when a cancer returns after a period of remission. This period could be days, months or even years. The new cancer is the same type as the original cancer, but can sometimes grow in a new location through a process called metastasis.
Actor Hugh Jackman has gone public about his multiple diagnoses of basal cell carcinoma (a type of skin cancer) over the past decade.
The exact reason why cancer returns differs depending on the cancer type and the treatment received. Research is ongoing to identify genes associated with cancers returning. This may eventually allow doctors to tailor treatments for high-risk people.
What are the chances of cancer returning?
The risk of cancer returning differs between cancers, and between sub-types of the same cancer.
New screening and treatment options have seen reductions in recurrence rates for many types of cancer. For example, between 2004 and 2019, the risk of colon cancer recurring dropped by 31-68%. It is important to remember that only someone’s treatment team can assess an individual’s personal risk of cancer returning.
For most types of cancer, the highest risk of cancer returning is within the first three years after entering remission. This is because any leftover cancer cells not killed by treatment are likely to start growing again sooner rather than later. Three years after entering remission, recurrence rates for most cancers decrease, meaning that every day that passes lowers the risk of the cancer returning.
Every day that passes also increases the numbers of new discoveries, and cancer drugs being developed.
What about second, unrelated cancers?
Earlier this year, we learned Sarah Ferguson, Duchess of York, had been diagnosed with malignant melanoma (a type of skin cancer) shortly after being treated for breast cancer.
Although details have not been confirmed, this is likely a new cancer that isn’t a recurrence or metastasis of the first one.
Australian research from Queensland and Tasmania shows adults who have had cancer have around a 6-36% higher risk of developing a second primary cancer compared to the risk of cancer in the general population.
Who’s at risk of another, unrelated cancer?
With improvements in cancer diagnosis and treatment, people diagnosed with cancer are living longer than ever. This means they need to consider their long-term health, including their risk of developing another unrelated cancer.
Reasons for such cancers include different types of cancers sharing the same kind of lifestyle, environmental and genetic risk factors.
The increased risk is also likely partly due to the effects that some cancer treatments and imaging procedures have on the body. However, this increased risk is relatively small when compared with the (sometimes lifesaving) benefits of these treatment and procedures.
While a 6-36% greater chance of getting a second, unrelated cancer may seem large, only around 10-12% of participants developed a second cancer in the Australian studies we mentioned. Both had a median follow-up time of around five years.
Similarly, in a large US study only about one in 12 adult cancer patients developed a second type of cancer in the follow-up period (an average of seven years).
The kind of first cancer you had also affects your risk of a second, unrelated cancer, as well as the type of second cancer you are at risk of. For example, in the two Australian studies we mentioned, the risk of a second cancer was greater for people with an initial diagnosis of head and neck cancer, or a haematological (blood) cancer.
People diagnosed with cancer as a child, adolescent or young adult also have a greater risk of a second, unrelated cancer.
What can I do to lower my risk?
Regular follow-up examinations can give peace of mind, and ensure any subsequent cancer is caught early, when there’s the best chance of successful treatment.
Maintenance therapy may be used to reduce the risk of some types of cancer returning. However, despite ongoing research, there are no specific treatments against cancer recurrence or developing a second, unrelated cancer.
But there are things you can do to help lower your general risk of cancer – not smoking, being physically active, eating well, maintaining a healthy body weight, limiting alcohol intake and being sun safe. These all reduce the chance of cancer returning and getting a second cancer.
Sarah Diepstraten, Senior Research Officer, Blood Cells and Blood Cancer Division, Walter and Eliza Hall Institute and Terry Boyle, Senior Lecturer in Cancer Epidemiology, University of South Australia
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: