The Best Kind Of Fiber For Overall Health?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Fiber Of Good Health
We’ve written before about how most people in industrialized nations in general, and N. America in particular, do not get nearly enough fiber:
Why You’re Probably Not Getting Enough Fiber (And How To Fix It)
Fiber’s important for many aspects of health, not least of all the heart:
What Matters Most For Your Heart? Eat More (Of This) For Lower Blood Pressure
As well, of course, as being critical for gut health:
Gut Health 101: Making Friends With Your Gut (You Can Thank Us Later)
But is all fiber “prebiotic fiber”, and/or are some better than others?
Beta-glucan
A recent study (it’s a mouse study, but promising in its applicability for humans) examined the health impacts of 5 different fiber types:
- pectin
- β-glucan
- wheat dextrin
- resistant starch
- cellulose (control)
As for health metrics, they measured:
- body weight
- adiposity
- indirect calorimetry
- glucose tolerance
- gut microbiota
- metabolites thereof
What they found was…
❝Only β-glucan supplementation during HFD-feeding decreased adiposity and body weight gain and improved glucose tolerance compared with HFD-cellulose, whereas all other fibers had no effect. This was associated with increased energy expenditure and locomotor activity in mice compared with HFD-cellulose.
All fibers supplemented into an HFD uniquely shifted the intestinal microbiota and cecal short-chain fatty acids; however, only β-glucan supplementation increased cecal butyrate concentrations. Lastly, all fibers altered the small-intestinal microbiota and portal bile acid composition. ❞
If you’d like to read more, the study itself is here:
If you’d like to read less, the short version is that they are all good but β-glucan scored best in several metrics.
It also acts indirectly as a GLP-1 agonist, by the way:
The right fiber may help you lose weight
You may be wondering: what is β-glucan found in?
It’s found in many (non-animal product) foods, but oats, barley, mushrooms, and yeasts are all good sources.
Is it available as a supplement?
More or less; there are supplements that contain it generously, here’s an example product on Amazon, a cordyceps extract, of which >30% is β-glucan.
As an aside, cordyceps itself has many other healthful properties too:
Cordyceps: Friend Or Foe? ← the answer is, it depends! If you’re human, it’s a friend.
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What the Health – by Kip Andersen, Keegan Kuhn, & Eunice Wong

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is a book from the makers of the famous documentary of the same name. Which means that yes, they are journalists not scientists, but they got input from very many scientists, doctors, nutritionists, and so forth, for a very reliable result.
It’s worth noting however that while a lot of the book is about the health hazards of a lot of the “Standard American Diet”, or “SAD” as it is appropriately abbreviated, a lot is also about how various industries
bribelobby the government to either push, or give them leeway to push, their products over healthier ones. So, there’s a lot about what would amount to corruption if it weren’t tied up in legalese that makes it just “lobbying” rather than bribery.The style is mostly narrative, albeit with very many citations adding up to 50 pages of references. There’s also a recipe section, which is… fairly basic, and despite getting a shoutout in the subtitle, the recipes are certainly not the real meat of the book.
The recipes themselves are entirely plant-based, and de facto vegan.
Bottom line: this one’s more of a polemic against industry malfeasance than it is a textbook of nutrition science, but there is enough information in here that it could have been the textbook if it wanted to, changing only the style and not the content.
Click here to check out What The Health, and make informed choices about yours!
Share This Post
-

Hair Growth: Caffeine and Minoxidil Strategies
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Questions and Answers at 10almonds
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
This newsletter has been growing a lot lately, and so have the questions/requests, and we love that! In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
Hair growth strategies for men combing caffeine and minoxidil?
Well, the strategy for that is to use caffeine and minoxidil! Some more specific tips, though:
- Both of those things need to be massaged (gently!) into your scalp especially around your hairline.
- In the case of caffeine, that boosts hair growth. No extra thought or care needed for that one.
- In the case of minoxidil, it reboots the hair growth cycle, so if you’ve only recently started, don’t be surprised (or worried) if you see more shedding in the first three months. It’s jettisoning your old hairs because new ones were just prompted (by the minoxidil) to start growing behind them. So: it will get briefly worse before it gets better, but then it’ll stay better… provided you keep using it.
- If you’d like other options besides minoxidil, finasteride is a commonly prescribed oral drug that blocks the conversion of testosterone to DHT, which latter is what tells your hairline to recede.
- If you’d like other options besides prescription drugs, saw palmetto performs comparably to finasteride (and works the same way).
- You may also want to consider biotin supplementation if you don’t already enjoy that
- Consider also using a dermaroller on your scalp. If you’re unfamiliar, this is a device that looks like a tiny lawn aerator, with many tiny needles, and you roll it gently across your skin.
- It can be used for promoting hair growth, as well as for reducing wrinkles and (more slowly) healing scars.
- It works by breaking up the sebum that may be blocking new hair growth, and also makes the skin healthier by stimulating production of collagen and elastin (in response to the thousands of microscopic wounds that the needles make).
- Sounds drastic, but it doesn’t hurt and doesn’t leave any visible marks—the needles are that tiny. Still, practise good sterilization and ensure your skin is clean when using it.
See: How To Use A Dermaroller ← also explains more of the science of it
PS: this question was asked in the context of men, but the information goes the same for women suffering from androgenic alepoceia—which is a lot more common than most people think!
Share This Post
- Both of those things need to be massaged (gently!) into your scalp especially around your hairline.
-

Their First Baby Came With Medical Debt. These Illinois Parents Won’t Have Another.
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
JACKSONVILLE, Ill. — Heather Crivilare was a month from her due date when she was rushed to an operating room for an emergency cesarean section.
The first-time mother, a high school teacher in rural Illinois, had developed high blood pressure, a sometimes life-threatening condition in pregnancy that prompted doctors to hospitalize her. Then Crivilare’s blood pressure spiked, and the baby’s heart rate dropped. “It was terrifying,” Crivilare said.
She gave birth to a healthy daughter. What followed, though, was another ordeal: thousands of dollars in medical debt that sent Crivilare and her husband scrambling for nearly a year to keep collectors at bay.
The Crivilares would eventually get on nine payment plans as they juggled close to $5,000 in bills.
“It really felt like a full-time job some days,” Crivilare recalled. “Getting the baby down to sleep and then getting on the phone. I’d set up one payment plan, and then a new bill would come that afternoon. And I’d have to set up another one.”
Crivilare’s pregnancy may have been more dramatic than most. But for millions of new parents, medical debt is now as much a hallmark of having children as long nights and dirty diapers.
About 12% of the 100 million U.S. adults with health care debt attribute at least some of it to pregnancy or childbirth, according to a KFF poll.
These people are more likely to report they’ve had to take on extra work, change their living situation, or make other sacrifices.
Overall, women between 18 and 35 who have had a baby in the past year and a half are twice as likely to have medical debt as women of the same age who haven’t given birth recently, other KFF research conducted for this project found.
“You feel bad for the patient because you know that they want the best for their pregnancy,” said Eilean Attwood, a Rhode Island OB-GYN who said she routinely sees pregnant women anxious about going into debt.
“So often, they may be coming to the office or the hospital with preexisting debt from school, from other financial pressures of starting adult life,” Attwood said. “They are having to make real choices, and what those real choices may entail can include the choice to not get certain services or medications or what may be needed for the care of themselves or their fetus.”
Best-Laid Plans
Crivilare and her husband, Andrew, also a teacher, anticipated some of the costs.
The young couple settled in Jacksonville, in part because the farming community less than two hours north of St. Louis was the kind of place two public school teachers could afford a house. They saved aggressively. They bought life insurance.
And before Crivilare got pregnant in 2021, they enrolled in the most robust health insurance plan they could, paying higher premiums to minimize their deductible and out-of-pocket costs.
Then, two months before their baby was due, Crivilare learned she had developed preeclampsia. Her pregnancy would no longer be routine. Crivilare was put on blood pressure medication, and doctors at the local hospital recommended bed rest at a larger medical center in Springfield, about 35 miles away.
“I remember thinking when they insisted that I ride an ambulance from Jacksonville to Springfield … ‘I’m never going to financially recover from this,’” she said. “‘But I want my baby to be OK.’”
For weeks, Crivilare remained in the hospital alone as covid protocols limited visitors. Meanwhile, doctors steadily upped her medications while monitoring the fetus. It was, she said, “the scariest month of my life.”
Fear turned to relief after her daughter, Rita, was born. The baby was small and had to spend nearly two weeks in the neonatal intensive care unit. But there were no complications. “We were incredibly lucky,” Crivilare said.
When she and Rita finally came home, a stack of medical bills awaited. One was already past due.
Crivilare rushed to set up payment plans with the hospitals in Jacksonville and Springfield, as well as the anesthesiologist, the surgeon, and the labs. Some providers demanded hundreds of dollars a month. Some settled for monthly payments of $20 or $25. Some pushed Crivilare to apply for new credit cards to pay the bills.
“It was a blur of just being on the phone constantly with all the different people collecting money,” she recalled. “That was a nightmare.”
Big Bills, Big Consequences
The Crivilares’ bills weren’t unusual. Parents with private health coverage now face on average more than $3,000 in medical bills related to a pregnancy and childbirth that aren’t covered by insurance, researchers at the University of Michigan found.
Out-of-pocket costs are even higher for families with a newborn who needs to stay in a neonatal ICU, averaging $5,000. And for 1 in 11 of these families, medical bills related to pregnancy and childbirth exceed $10,000, the researchers found.
“This forces very difficult trade-offs for families,” said Michelle Moniz, a University of Michigan OB-GYN who worked on the study. “Even though they have insurance, they still have these very high bills.”
Nationwide polls suggest millions of these families end up in debt, with sometimes devastating consequences.
About three-quarters of U.S. adults with debt related to pregnancy or childbirth have cut spending on food, clothing, or other essentials, KFF polling found.
About half have put off buying a home or delayed their own or their children’s education.
These burdens have spurred calls to limit what families must pay out-of-pocket for medical care related to pregnancy and childbirth.
In Massachusetts, state Sen. Cindy Friedman has proposed legislation to exempt all these bills from copays, deductibles, and other cost sharing. This would parallel federal rules that require health plans to cover recommended preventive services like annual physicals without cost sharing for patients. “We want … healthy children, and that starts with healthy mothers,” Friedman said. Massachusetts health insurers have warned the proposal will raise costs, but an independent state analysis estimated the bill would add only $1.24 to monthly insurance premiums.
Tough Lessons
For her part, Crivilare said she wishes new parents could catch their breath before paying down medical debt.
“No one is in the right frame of mind to deal with that when they have a new baby,” she said, noting that college graduates get such a break. “When I graduated with my college degree, it was like: ‘Hey, new adult, it’s going to take you six months to kind of figure out your life, so we’ll give you this six-month grace period before your student loans kick in and you can get a job.’”
Rita is now 2. The family scraped by on their payment plans, retiring the medical debt within a year, with help from Crivilare’s side job selling resources for teachers online.
But they are now back in debt, after Rita’s recurrent ear infections required surgery last year, leaving the family with thousands of dollars in new medical bills.
Crivilare said the stress has made her think twice about seeing a doctor, even for Rita. And, she added, she and her husband have decided their family is complete.
“It’s not for us to have another child,” she said. “I just hope that we can put some of these big bills behind us and give [Rita] the life that we want to give her.”
About This Project
“Diagnosis: Debt” is a reporting partnership between KFF Health News and NPR exploring the scale, impact, and causes of medical debt in America.
The series draws on original polling by KFF, court records, federal data on hospital finances, contracts obtained through public records requests, data on international health systems, and a yearlong investigation into the financial assistance and collection policies of more than 500 hospitals across the country.
Additional research was conducted by the Urban Institute, which analyzed credit bureau and other demographic data on poverty, race, and health status for KFF Health News to explore where medical debt is concentrated in the U.S. and what factors are associated with high debt levels.
The JPMorgan Chase Institute analyzed records from a sampling of Chase credit card holders to look at how customers’ balances may be affected by major medical expenses. And the CED Project, a Denver nonprofit, worked with KFF Health News on a survey of its clients to explore links between medical debt and housing instability.
KFF Health News journalists worked with KFF public opinion researchers to design and analyze the “KFF Health Care Debt Survey.” The survey was conducted Feb. 25 through March 20, 2022, online and via telephone, in English and Spanish, among a nationally representative sample of 2,375 U.S. adults, including 1,292 adults with current health care debt and 382 adults who had health care debt in the past five years. The margin of sampling error is plus or minus 3 percentage points for the full sample and 3 percentage points for those with current debt. For results based on subgroups, the margin of sampling error may be higher.
Reporters from KFF Health News and NPR also conducted hundreds of interviews with patients across the country; spoke with physicians, health industry leaders, consumer advocates, debt lawyers, and researchers; and reviewed scores of studies and surveys about medical debt.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Share This Post
-

Fruit Is Healthy; Juice Isn’t (Here’s Why)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Biochemist and “Glucose Goddess” Jessie Inchauspé wants us to understand the difference:
Stripped!
A glass of orange juice contains 22 grams of sugar (about six sugar cubes), nearly as much as a can of soda (27 grams).
Orange juice is widely perceived as healthy due to vitamin content—but if you add vitamins to soda, it won’t make it healthy, because the main health effect is still the sugar, leading to glucose spikes and many resultant health risks. The positive image of fruit juice is mainly from industry marketing.
In reality, Inchauspé advises, fruit juice should be treated like a dessert—consumed for pleasure, not health benefits.
But why, then, is fruit healthy if fruit juice is unhealthy? Isn’t the sugar there too?
Whole fruit contains plenty of fiber, which slows sugar absorption and prevents glucose spikes. Juicing strips it of its fiber, leaving water and sugar.
The American Heart Association suggests a sugar limit: 25g/day for women, 36g/day for men. One glass of orange juice nearly meets the daily limit for women. If that’s how you want to “spend” your daily sugar allowance, go for it, but do so consciously, by choice, knowing that the allowance is now “spent”.
In contrast, if you eat whole fruit, that basically “doesn’t count” for sugar purposes. The sugar is there, but the fiber more than offsets it, making whole fruit very good for blood sugars.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Which Sugars Are Healthier, And Which Are Just The Same?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What happens in my brain when I get a migraine? And what medications can I use to treat it?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Migraine is many things, but one thing it’s not is “just a headache”.
“Migraine” comes from the Greek word “hemicrania”, referring to the common experience of migraine being predominantly one-sided.
Some people experience an “aura” preceding the headache phase – usually a visual or sensory experience that evolves over five to 60 minutes. Auras can also involve other domains such as language, smell and limb function.
Migraine is a disease with a huge personal and societal impact. Most people cannot function at their usual level during a migraine, and anticipation of the next attack can affect productivity, relationships and a person’s mental health.

Francisco Gonzelez/Unsplash What’s happening in my brain?
The biological basis of migraine is complex, and varies according to the phase of the migraine. Put simply:
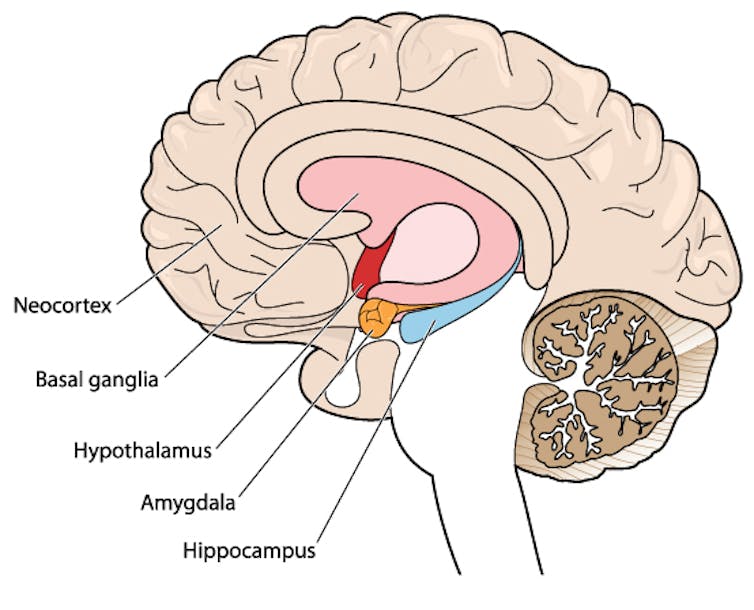
The earliest phase is called the prodrome. This is associated with activation of a part of the brain called the hypothalamus which is thought to contribute to many symptoms such as nausea, changes in appetite and blurred vision.
The hypothalamus is shown here in red. Blamb/Shutterstock Next is the aura phase, when a wave of neurochemical changes occur across the surface of the brain (the cortex) at a rate of 3–4 millimetres per minute. This explains how usually a person’s aura progresses over time. People often experience sensory disturbances such as flashes of light or tingling in their face or hands.
In the headache phase, the trigeminal nerve system is activated. This gives sensation to one side of the face, head and upper neck, leading to release of proteins such as CGRP (calcitonin gene-related peptide). This causes inflammation and dilation of blood vessels, which is the basis for the severe throbbing pain associated with the headache.
Finally, the postdromal phase occurs after the headache resolves and commonly involves changes in mood and energy.
What can you do about the acute attack?
A useful way to conceive of migraine treatment is to compare putting out campfires with bushfires. Medications are much more successful when applied at the earliest opportunity (the campfire). When the attack is fully evolved (into a bushfire), medications have a much more modest effect.
Aspirin
For people with mild migraine, non-specific anti-inflammatory medications such as high-dose aspirin, or standard dose non-steroidal medications (NSAIDS) can be very helpful. Their effectiveness is often enhanced with the use of an anti-nausea medication.
Triptans
For moderate to severe attacks, the mainstay of treatment is a class of medications called “triptans”. These act by reducing blood vessel dilation and reducing the release of inflammatory chemicals.
Triptans vary by their route of administration (tablets, wafers, injections, nasal sprays) and by their time to onset and duration of action.
The choice of a triptan depends on many factors including whether nausea and vomiting is prominent (consider a dissolving wafer or an injection) or patient tolerability (consider choosing one with a slower onset and offset of action).
As triptans constrict blood vessels, they should be used with caution (or not used) in patients with known heart disease or previous stroke.
Triptans should be used cautiously in patients with heart disease. CDC/Unsplash Gepants
Some medications that block or modulate the release of CGRP, which are used for migraine prevention (which we’ll discuss in more detail below), also have evidence of benefit in treating the acute attack. This class of medication is known as the “gepants”.
Gepants come in the form of injectable proteins (monoclonal antibodies, used for migraine prevention) or as oral medication (for example, rimegepant) for the acute attack when a person has not responded adequately to previous trials of several triptans or is intolerant of them.
They do not cause blood vessel constriction and can be used in patients with heart disease or previous stroke.
Ditans
Another class of medication, the “ditans” (for example, lasmiditan) have been approved overseas for the acute treatment of migraine. Ditans work through changing a form of serotonin receptor involved in the brain chemical changes associated with the acute attack.
However, neither the gepants nor the ditans are available through the Pharmaceutical Benefits Scheme (PBS) for the acute attack, so users must pay out-of-pocket, at a cost of approximately A$300 for eight wafers.
What about preventing migraines?
The first step is to see if lifestyle changes can reduce migraine frequency. This can include improving sleep habits, routine meal schedules, regular exercise, limiting caffeine intake and avoiding triggers such as stress or alcohol.
Despite these efforts, many people continue to have frequent migraines that can’t be managed by acute therapies alone. The choice of when to start preventive treatment varies for each person and how inclined they are to taking regular medication. Those who suffer disabling symptoms or experience more than a few migraines a month benefit the most from starting preventives.
Some people will take medicines to prevent migraines. Tbel Abuseridze/Unsplash Almost all migraine preventives have existing roles in treating other medical conditions, and the physician would commonly recommend drugs that can also help manage any pre-existing conditions. First-line preventives include:
- tablets that lower blood pressure (candesartan, metoprolol, propranolol)
- antidepressants (amitriptyline, venlafaxine)
- anticonvulsants (sodium valproate, topiramate).
Some people have none of these other conditions and can safely start medications for migraine prophylaxis alone.
For all migraine preventives, a key principle is starting at a low dose and increasing gradually. This approach makes them more tolerable and it’s often several weeks or months until an effective dose (usually 2- to 3-times the starting dose) is reached.
It is rare for noticeable benefits to be seen immediately, but with time these drugs typically reduce migraine frequency by 50% or more.
‘Nothing works for me!’
In people who didn’t see any effect of (or couldn’t tolerate) first-line preventives, new medications have been available on the PBS since 2020. These medications block the action of CGRP.
The most common PBS-listed anti-CGRP medications are injectable proteins called monoclonal antibodies (for example, galcanezumab and fremanezumab), and are self-administered by monthly injections.
These drugs have quickly become a game-changer for those with intractable migraines. The convenience of these injectables contrast with botulinum toxin injections (also effective and PBS-listed for chronic migraine) which must be administered by a trained specialist.
Up to half of adolescents and one-third of young adults are needle-phobic. If this includes you, tablet-form CGRP antagonists for migraine prevention are hopefully not far away.
Data over the past five years suggest anti-CGRP medications are safe, effective and at least as well tolerated as traditional preventives.
Nonetheless, these are used only after a number of cheaper and more readily available first-line treatments (all which have decades of safety data) have failed, and this also a criterion for their use under the PBS.
Mark Slee, Associate Professor, Clinical Academic Neurologist, Flinders University and Anthony Khoo, Lecturer, Flinders University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Who Screens The Sunscreens?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We Screen The Sunscreens!

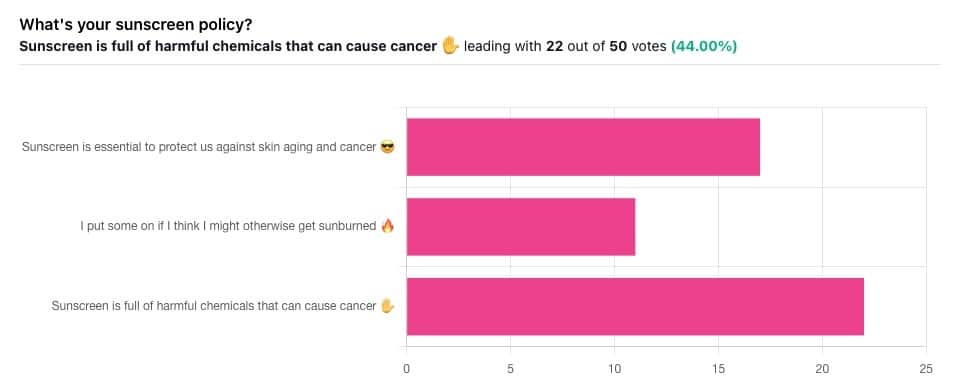
Yesterday, we asked you what your sunscreen policy was, and got a spread of answers. Apparently this one was quite polarizing!
One subscriber who voted for “Sunscreen is essential to protect us against skin aging and cancer” wrote:
❝My mom died of complications from melanoma, so we are vigilant about sun and sunscreen. We are a family of campers and hikers and gardeners—outdoors in all seasons—and we never burn❞
Our condolences with regard to your mom! Life is so precious, and when something like that happens, it tends to stick with us. We’re glad you and your family are taking care of yourselves.
Of the subscribers who voted for “I put some on if I think I might otherwise get sunburned”, about half wrote to express uncertainties:
- uncertainty about how safe it is, and
- uncertainty about how helpful it is
…so we’re going to tackle those questions in a moment. But what of those who voted for “Sunscreen is full of harmful chemicals that can cause cancer”?
Of those, only one wrote a message, which was to say one has to be very careful of what is in the formula.
Let’s take a look, then…
Sunscreen is full of harmful chemicals that can cause cancer: True or False?
False—according to current best science. Research is ongoing!
There are four main chemicals (found in most sunscreens) that people tend to worry about:
- Abobenzone
- Oxybenzone
- Octocrylene
- Ecamsule
Now, these two sound like four brands of rocket fuel, but then, dihydrogen monoxide (DHMO), which is also found in most sunscreens, sounds like a deadly toxin too. That’s water, by the way.
But what of these four chemicals? Well, as we say, research is ongoing, but we found a study that measured all four, to see how much got into the blood, and what adverse effects, if any, this caused.
We’ll skip to their conclusion:
❝In this preliminary study involving healthy volunteers, application of 4 commercially available sunscreens under maximal use conditions resulted in plasma concentrations that exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens. The systemic absorption of sunscreen ingredients supports the need for further studies to determine the clinical significance of these findings. These results do not indicate that individuals should refrain from the use of sunscreen.❞
Now, “exceeded the threshold established by the FDA for potentially waiving some nonclinical toxicology studies for sunscreens” sounds alarming, so why did they close with the words “These results do not indicate that individuals should refrain from the use of sunscreen”?
Let’s skip back up to a line from the results:
❝The most common adverse event was rash, which developed in 1 participant with each sunscreen.❞
This was most probably due to the oxybenzone, which can cause allergic skin reactions in some people.
Let us take a moment to remember the most common adverse event that occurs from not wearing sunscreen: sunburn!
You can read the full study here:
None of those ingredients have been found to be carcinogenic, even at the maximal blood plasma concentrations studied, from applications 4x/day to 75% of the body.
UVA rays, on the other hand, are absolutely very much known to cause cancer, and the effect is cumulative.
Sunscreen is essential to protect us against skin aging and cancer: True or False?
True, unequivocally, unless we live indoors and/or otherwise never go about under sunlight.
“But our ancestors—” lived under the same sun we do, and either used sunscreen or got advanced skin aging and cancer.
Sunscreen of times past ranged from mud to mineral lotions, but it’s pretty much always existed. Even non-human animals that have skin and don’t have fur or feathers, tend to take mud-baths in sunny parts of the world.
If you’d like to avoid oxybenzone and other chemicals, though, you might have your reasons. Maybe you’re allergic, or maybe you read that it’s a potential endocrine disruptor with estrogen-like and anti-androgenic properties that you don’t want.
There are other options, to include physical blockers containing zinc and titanium dioxide, which are generally recognized as safe and effective ingredients.
If you’re interested, you can even make your own sunscreen that blocks both UVA and UVB rays (UVA is what causes skin cancer; UVB is “milder” and is what causes sunburn):
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: