Avocado vs Goji Berries – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing avocado to goji berries, we picked the avocado.
Why?
It takes a special non-dried food to beat a dried food for nutritional density, but avocado manages it!
In terms of macros, avocados have more (famously health) fat; mostly monounsaturated with some polyunsaturated and a little bit of saturated, with some omega-3 and omega-6, in a healthy ratio. Meanwhile, goji berries have more fiber, carbs, and protein. As for glycemic indices, avocados are low GI (40), but goji berries are zero-GI, or, functionally, a negative glycemic index as (notwithstanding their sugar content!) they have an overall lowering effect on blood sugars. In short, both of these fruits have very different things to offer in the macros category, so we’re declaring this round a tie.
In the category of vitamins, avocados have more of vitamins A, B1, B2, B3, B5, B6, B7, B9, E, K, and choline, while goji berries have more vitamin C. A clear win for avocados!
When it comes to minerals, avocados have more copper, magnesium, manganese, phosphorus, potassium, selenium, and zinc, while goji berries have more calcium and iron. Another win for avocados!
In short, enjoy either or both (diversity is good), but for overall nutritional density, avocados win this superfood showdown today.
Want to learn more?
You might like to read:
What’s Your Plant Diversity Score?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

End Your Carb Confusion – by Dr. Eric Westman & Amy Berger

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Carbs can indeed be confusing! We’ve written about it ourselves before, but there’s more to be said than fits in a single article, and sometimes a book is in order. This one is such a book.
The authors (an MD and a nutritionist) explain the ins and outs of carbohydrates of various kinds, insulin responses, and what that means for the body. They also then look at the partly-similar, partly-different processes that occur with the metabolism of fats of various kinds, and what that means for the body, too.
Ultimately they advocate for a simple and clear low-carb approach broadly consistent with keto diet macro principles, without getting too overly focused on “is this fruit/vegetable ok?” minutiae. This has the benefit of putting it well aside from the paleo diet, for example (which focuses more on pseudo-historical foods than it does on macros), and also makes it a lot easier on a practical level.
The style is very textbook-like, which makes for an easy read with plenty of information that should stick easily in most reader’s minds, rather than details getting lost in wall-of-text formatting. So, we approve of this.
There is not, by the way, a recipes section. It’s “here’s the information, now go forth and enjoy” and leaves us all to find/make our own recipes, rather than trying to guess our culinary preferences.
Bottom line: if you’d like an easy-to-read primer on understanding how carbs work, what it means for you, and what to do about it, then this is a fine book.
Click here to check out End Your Carb Confusion, and end your carb confusion!
Share This Post
-

How To Stay Alive (When You Really Don’t Want To)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Stay Alive (When You Really Don’t Want To)
A subscriber recently requested:
❝Request: more people need to be aware of suicidal tendencies and what they can do to ward them off❞
…and we said we’d do that one of these Psychology Sundays, so here we are, doing it!
First of all, we’ll mention that we did previously do a main feature on managing depression (in oneself or a loved one); here it is:
The Mental Health First Aid That You’ll Hopefully Never Need
Now, not all depression leads to suicidality, and not all suicide is pre-empted by depression, but there’s a large enough crossover that it seems sensible to put that article here, for anyone who might find it of use, or even just of interest.
Now, onwards, to the specific, and very important, topic of suicide.
This should go without saying, but some of today’s content may be a little heavy.
We invite you to read it anyway if you’re able, because it’s important stuff that we all should know, and not talking about it is part of what allows it to kill people.
So, let’s take a deep breath, and read on…
The risk factors
Top risk factors for suicide include:
- Not talking about it
- Having access to a firearm
- Having a plan of specifically how to commit suicide
- A lack of social support
- Being male
- Being over 40
Now, some of these are interesting sociologically, but aren’t very useful practically; what a convenient world it’d be if we could all simply choose to be under 40, for instance.
Some serve as alarm bells, such as “having a plan of specifically how to commit suicide”.
If someone has a plan, that plan’s never going to disappear entirely, even if it’s set aside!
(this writer is deeply aware of the specifics of how she has wanted to end things before, and has used the advice she gives in this article herself numerous times. So far so good, still alive to write about it!)
Specific advices, therefore, include:
Talk about it / Listen
Depending on whether it’s you or someone else at risk:
- Talk about it, if it’s you
- Listen attentively, if it’s someone else
There are two main objections that you might have at this point, so let’s look at those:
“I have nobody to talk to”—it can certainly feel that way, sometimes, but you may be surprised who would listen if you gave them the chance. If you really can’t trust anyone around you, there are of course suicide hotlines (usually per area, so we’ll not try to list them here; a quick Internet search will get you what you need).
If you’re worried it’ll result in bad legal/social consequences, check their confidentiality policy first:
- Some hotlines can and will call the police, for instance.
- Others deliberately have a set-up whereby they couldn’t even trace the call if they wanted to.
- On the one hand, that means they can’t intervene
- On the other hand, that means they’re a resource for anyone who will only trust a listener who can’t intervene.
“But it is just a cry for help”—then that person deserves help. What some may call “attention-seeking” is, in effect, care-seeking. Listen, without judgement.
Remove access to firearms, if applicable and possible
Ideally, get rid of them (safely and responsibly, please).
If you can’t bring yourself to do that, make them as inconvenient to get at as possible. Stored securely at your local gun club is better than at home, for example.
If your/their plan isn’t firearm-related, but the thing in question can be similarly removed, remove it. You/they do not need that stockpile of pills, for instance.
And of course you/they could get more, but the point is to make it less frictionless. The more necessary stopping points between thinking “I should just kill myself” and being able to actually do it, the better.
Have/give social support
What do the following people have in common?
- A bullied teenager
- A divorced 40-something who just lost a job
- A lonely 70-something with no surviving family, and friends that are hard to visit
Often, at least, the answer is: the absence of a good social support network
So, it’s good to get one, and be part of some sort of community that’s meaningful to us. That could look different to a lot of people, for example:
- A church, or other religious community, if we be religious
- The LGBT+ community, or even just a part of it, if that fits for us
- Any mutual-support oriented, we-have-this-shared-experience community, could be anything from AA to the VA.
Some bonus ideas…
If you can’t live for love, living for spite might suffice. Outlive your enemies; don’t give them the satisfaction.
If you’re going to do it anyway, you might as well take the time to do some “bucket list” items first. After all, what do you have to lose? Feel free to add further bucket list items as they occur to you, of course. Because, why not? Before you know it, you’ve postponed your way into a rich and fulfilling life.
Finally, some gems from Matt Haig’s “The Comfort Book”:
- “The hardest question I have been asked is: “How do I stay alive for other people if I have no one?” The answer is that you stay alive for other versions of you. For the people you will meet, yes, but also the people you will be.”
- “Stay for the person you will become”
- “You are more than a bad day, or week, or month, or year, or even decade”
- “It is better to let people down than to blow yourself up”
- “Nothing is stronger than a small hope that doesn’t give up”
- “You are here. And that is enough.”
You can find Matt Haig’s excellent “The Comfort Book” on Amazon, as well as his more well-known book more specifically on the topic we’ve covered today, “Reasons To Stay Alive“.
Share This Post
-

Fermenting Everything – by Andy Hamilton
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This is not justanother pickling book! This is, instead, what it says on the front cover, “fermenting everything”.
Ok, maybe not literally everything, but every kind of thing that can reasonably be fermented, and it’s probably a lot more things than you might think.
From habanero chutney to lacto-lemonade, aioli to kombucha, Ukrainian fermented tomatoes to kvass. We could go on, but we’d soon run out of space. You get the idea. If it’s a fermented product (food, drink, condiment) and you’ve heard of it, there’s probably a recipe in here.
All in all, this is a great way to get in your gut-healthy daily dose of fermented products!
He does also talk safety, and troubleshooting too. And so long as you have a collection of big jars and a fairly normally-furnished kitchen, you shouldn’t need any more special equipment than that, unless you decide to you your fermentation skills for making beer (which does need some extra equipment, and he offers advice on that—our advice as a health science publication is “don’t drink beer”, though).
Bottom line: with this in hand, you can create a lot of amazing foods/drinks/condiments that are not only delicious, but also great for gut health.
Click here to check out Fermenting Everything, and widen your culinary horizons!
Share This Post
Related Posts
-

Why it’s a bad idea to mix alcohol with some medications
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Anyone who has drunk alcohol will be familiar with how easily it can lower your social inhibitions and let you do things you wouldn’t normally do.
But you may not be aware that mixing certain medicines with alcohol can increase the effects and put you at risk.
When you mix alcohol with medicines, whether prescription or over-the-counter, the medicines can increase the effects of the alcohol or the alcohol can increase the side-effects of the drug. Sometimes it can also result in all new side-effects.
How alcohol and medicines interact
The chemicals in your brain maintain a delicate balance between excitation and inhibition. Too much excitation can lead to convulsions. Too much inhibition and you will experience effects like sedation and depression.
Alcohol works by increasing the amount of inhibition in the brain. You might recognise this as a sense of relaxation and a lowering of social inhibitions when you’ve had a couple of alcoholic drinks.
With even more alcohol, you will notice you can’t coordinate your muscles as well, you might slur your speech, become dizzy, forget things that have happened, and even fall asleep.

Alcohol can affect the way a medicine works.
Jonathan Kemper/UnsplashMedications can interact with alcohol to produce different or increased effects. Alcohol can interfere with the way a medicine works in the body, or it can interfere with the way a medicine is absorbed from the stomach. If your medicine has similar side-effects as being drunk, those effects can be compounded.
Not all the side-effects need to be alcohol-like. Mixing alcohol with the ADHD medicine ritalin, for example, can increase the drug’s effect on the heart, increasing your heart rate and the risk of a heart attack.
Combining alcohol with ibuprofen can lead to a higher risk of stomach upsets and stomach bleeds.
Alcohol can increase the break-down of certain medicines, such as opioids, cannabis, seizures, and even ritalin. This can make the medicine less effective. Alcohol can also alter the pathway of how a medicine is broken down, potentially creating toxic chemicals that can cause serious liver complications. This is a particular problem with paracetamol.
At its worst, the consequences of mixing alcohol and medicines can be fatal. Combining a medicine that acts on the brain with alcohol may make driving a car or operating heavy machinery difficult and lead to a serious accident.
Who is at most risk?
The effects of mixing alcohol and medicine are not the same for everyone. Those most at risk of an interaction are older people, women and people with a smaller body size.
Older people do not break down medicines as quickly as younger people, and are often on more than one medication.
Older people also are more sensitive to the effects of medications acting on the brain and will experience more side-effects, such as dizziness and falls.
Smaller and older people are often more affected.
Alfonso Scarpa/UnsplashWomen and people with smaller body size tend to have a higher blood alcohol concentration when they consume the same amount of alcohol as someone larger. This is because there is less water in their bodies that can mix with the alcohol.
What drugs can’t you mix with alcohol?
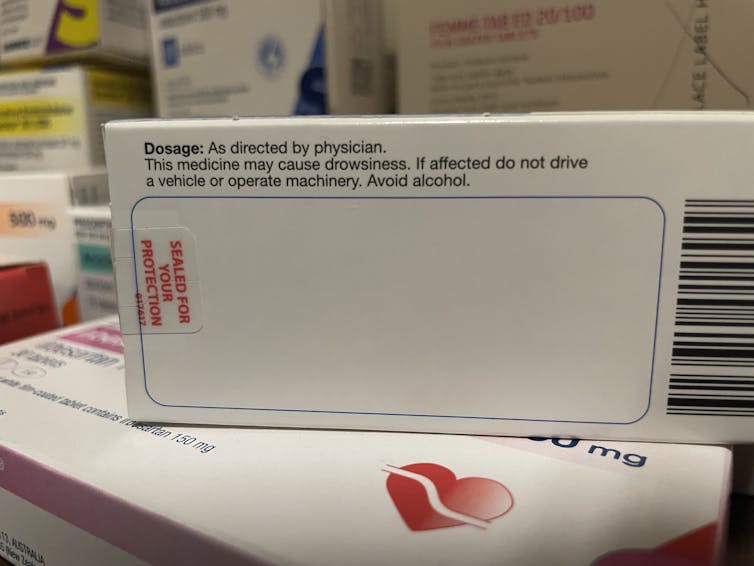
You’ll know if you can’t take alcohol because there will be a prominent warning on the box. Your pharmacist should also counsel you on your medicine when you pick up your script.
The most common alcohol-interacting prescription medicines are benzodiazepines (for anxiety, insomnia, or seizures), opioids for pain, antidepressants, antipsychotics, and some antibiotics, like metronidazole and tinidazole.
Medicines will carry a warning if you shouldn’t take them with alcohol.
Nial WheateIt’s not just prescription medicines that shouldn’t be mixed with alcohol. Some over-the-counter medicines that you shouldn’t combine with alcohol include medicines for sleeping, travel sickness, cold and flu, allergy, and pain.
Next time you pick up a medicine from your pharmacist or buy one from the local supermarket, check the packaging and ask for advice about whether you can consume alcohol while taking it.
If you do want to drink alcohol while being on medication, discuss it with your doctor or pharmacist first.

Nial Wheate, Associate Professor of the School of Pharmacy, University of Sydney; Jasmine Lee, Pharmacist and PhD Candidate, University of Sydney; Kellie Charles, Associate Professor in Pharmacology, University of Sydney, and Tina Hinton, Associate Professor of Pharmacology, University of Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

I’m iron deficient. Which supplements will work best for me and how should I take them?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Iron deficiency is common and can be debilitating. It mainly affects women. One in three premenopausal women are low in iron compared to just 5% of Australian men. Iron deficiency particularly affects teenage girls, women who do a lot of exercise and those who are pregnant.
The body needs iron to make new red blood cells, and to support energy production, the immune system and cognitive function. If you’re low, you may experience a range of symptoms including fatigue, weakness, shortness of breath, headache, irregular heartbeat and reduced concentration.
If a blood test shows you’re iron deficient, your doctor may recommend you start taking an oral iron supplement. But should you take a tablet or a liquid? With food or not? And when is the best time of day?
Here are some tips to help you work out how, when and what iron supplement to take.
LittlePigPower/Shutterstock How do I pick the right iron supplement?
The iron in your body is called “elemental iron”. Choosing the right oral supplement and dose will depend on how much elemental iron it has – your doctor will advise exactly how much you need.
The sweet spot is between 60-120 mg of elemental iron. Any less and the supplement won’t be effective in topping up your iron levels. Any higher and you risk gastrointestinal symptoms such as diarrhoea, cramping and stomach pain.
Low iron can especially affect people during pregnancy and women who do a lot of sport. Kamil Macniak/Shutterstock In Australia, iron salts are the most common oral supplements because they are cheap, effective and come in different delivery methods (tablets, capsules, liquid formulas). The iron salts you are most likely to find in your local chemist are ferrous sulfate (~20% elemental iron), ferrous gluconate (~12%) and ferrous fumarate (~33%).
These formulations all work similarly, so your choice should come down to dose and cost.
Many multivitamins may look like an iron supplement, but it’s important to note they usually have too little iron – usually less than 20 mg – to correct an iron deficiency.
Should I take tablets or liquid formulas?
Iron contained within a tablet is just as well absorbed as iron found in a liquid supplement. Choosing the right one usually comes down to personal preference.
The main difference is that liquid formulas tend to contain less iron than tablets. That means you might need to take more of the product to get the right dose, so using a liquid supplement could work out to be more expensive in the long term.
What should I eat with my iron supplement?
Research has shown you will absorb more of the iron in your supplement if you take it on an empty stomach. But this can cause more gastrointestinal issues, so might not be practical for everyone.
If you do take your supplement with meals, it’s important to think about what types of food will boost – rather than limit – iron absorption. For example, taking the supplement alongside vitamin C improves your body’s ability to absorb it.
Some supplements already contain vitamin C. Otherwise you could take the supplement along with a glass of orange juice, or other vitamin C-rich foods.
Taking your supplement alongside foods rich in vitamin C, like orange juice or kiwifruit, can help your body absorb the iron. Anete Lusina/Pexels On the other hand, tea, coffee and calcium all decrease the body’s ability to absorb iron. So you should try to limit these close to the time you take your supplement.
Should I take my supplement in the morning or evening?
The best time of day to take your supplement is in the morning. The body can absorb significantly more iron earlier in the day, when concentrations of hepcidin (the main hormone that regulates iron) are at their lowest.
Exercise also affects the hormone that regulates iron. That means taking your iron supplement after exercising can limit your ability to absorb it. Taking your supplement in the hours following exercise will mean significantly poorer absorption, especially if you take it between two and five hours after you stop.
Our research has shown if you exercise every day, the best time to take your supplement is in the morning before training, or immediately after (within 30 minutes).
My supplements are upsetting my stomach. What should I do?
If you experience gastrointestinal side effects such as diarrhoea or cramps when you take iron supplements, you may want to consider taking your supplement every second day, rather than daily.
Taking a supplement every day is still the fastest way to restore your iron levels. But a recent study has shown taking the same total dose can be just as effective when it’s taken on alternate days. For example, taking a supplement every day for three months works as well as every second day for six months. This results in fewer side effects.
Oral iron supplements can be a cheap and easy way to correct an iron deficiency. But ensuring you are taking the right product, under the right conditions, is crucial for their success.
It’s also important to check your iron levels prior to commencing iron supplementation and do so only under medical advice. In large amounts, iron can be toxic, so you don’t want to be consuming additional iron if your body doesn’t need it.
If you think you may be low on iron, talk to your GP to find out your best options.
Alannah McKay, Postdoctoral Research Fellow, Sports Nutrition, Australian Catholic University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What is AuDHD? 5 important things to know when someone has both autism and ADHD
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
You may have seen some new ways to describe when someone is autistic and also has attention-deficit hyperactivity disorder (ADHD). The terms “AuDHD” or sometimes “AutiADHD” are being used on social media, with people describing what they experience or have seen as clinicians.
It might seem surprising these two conditions can co-occur, as some traits appear to be almost opposite. For example, autistic folks usually have fixed routines and prefer things to stay the same, whereas people with ADHD usually get bored with routines and like spontaneity and novelty.
But these two conditions frequently overlap and the combination of diagnoses can result in some unique needs. Here are five important things to know about AuDHD.
Kosro/Shutterstock 1. Having both wasn’t possible a decade ago
Only in the past decade have autism and ADHD been able to be diagnosed together. Until 2013, the Diagnostic and Statistical Manual of Mental Disorders (DSM) – the reference used by health workers around the world for definitions of psychological diagnoses – did not allow for ADHD to be diagnosed in an autistic person.
The manual’s fifth edition was the first to allow for both diagnoses in the same person. So, folks diagnosed and treated prior to 2013, as well as much of the research, usually did not consider AuDHD. Instead, children and adults may have been “assigned” to whichever condition seemed most prominent or to be having the greater impact on everyday life.
2. AuDHD is more common than you might think
Around 1% to 4% of the population are autistic.
They can find it difficult to navigate social situations and relationships, prefer consistent routines, find changes overwhelming and repetition soothing. They may have particular sensory sensitivities.
ADHD occurs in around 5–8% of children and adolescents and 2–6% of adults. Characteristics can include difficulties with focusing attention in a flexible way, resulting in procrastination, distraction and disorganisation. People with ADHD can have high levels of activity and impulsivity.
Studies suggest around 40% of those with ADHD also meet diagnostic criteria for autism and vice versa. The co-occurrence of having features or traits of one condition (but not meeting the full diagnostic criteria) when you have the other, is even more common and may be closer to around 80%. So a substantial proportion of those with autism or ADHD who don’t meet full criteria for the other condition, will likely have some traits.
3. Opposing traits can be distressing
Autistic people generally prefer order, while ADHDers often struggle to keep things organised. Autistic people usually prefer to do one thing at a time; people with ADHD are often multitasking and have many things on the go. When someone has both conditions, the conflicting traits can result in an internal struggle.
For example, it can be upsetting when you need your things organised in a particular way but ADHD traits result in difficulty consistently doing this. There can be periods of being organised (when autistic traits lead) followed by periods of disorganisation (when ADHD traits dominate) and feelings of distress at not being able to maintain organisation.
There can be eventual boredom with the same routines or activities, but upset and anxiety when attempting to transition to something new.
Autistic special interests (which are often all-consuming, longstanding and prioritised over social contact), may not last as long in AuDHD, or be more like those seen in ADHD (an intense deep dive into a new interest that can quickly burn out).
Autism can result in quickly being overstimulated by sensory input from the environment such as noises, lighting and smells. ADHD is linked with an understimulated brain, where intense pressure, novelty and excitement can be needed to function optimally.
For some people the conflicting traits may result in a balance where people can find a middle ground (for example, their house appears tidy but the cupboards are a little bit messy).
There isn’t much research yet into the lived experience of this “trait conflict” in AuDHD, but there are clinical observations.
4. Mental health and other difficulties are more frequent
Our research on mental health in children with autism, ADHD or AuDHD shows children with AuDHD have higher levels of mental health difficulites than autism or ADHD alone.
This is a consistent finding with studies showing higher mental health difficulties such as depression and anxiety in AuDHD. There are also more difficulties with day-to-day functioning in AuDHD than either condition alone.
So there is an additive effect in AuDHD of having the executive foundation difficulties found in both autism and ADHD. These difficulties relate to how we plan and organise, pay attention and control impulses. When we struggle with these it can greatly impact daily life.
5. Getting the right treatment is important
ADHD medication treatments are evidence-based and effective. Studies suggest medication treatment for ADHD in autistic people similarly helps improve ADHD symptoms. But ADHD medications won’t reduce autistic traits and other support may be needed.
Non-pharmacological treatments such as psychological or occupational therapy are less researched in AuDHD but likely to be helpful. Evidence-based treatments include psychoeducation and psychological therapy. This might include understanding one’s strengths, how traits can impact the person, and learning what support and adjustments are needed to help them function at their best. Parents and carers also need support.
The combination and order of support will likely depend on the person’s current functioning and particular needs. https://www.youtube.com/embed/pMx1DnSn-eg?wmode=transparent&start=0 ‘Up until recently … if you had one, you couldn’t have the other.’
Do you relate?
Studies suggest people may still not be identified with both conditions when they co-occur. A person in that situation might feel misunderstood or that they can’t fully relate to others with a singular autism and ADHD diagnosis and something else is going on for them.
It is important if you have autism or ADHD that the other is considered, so the right support can be provided.
If only one piece of the puzzle is known, the person will likely have unexplained difficulties despite treatment. If you have autism or ADHD and are unsure if you might have AuDHD consider discussing this with your health professional.
Tamara May, Psychologist and Research Associate in the Department of Paediatrics, Monash University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: