Over 50? Do These 3 Stretches Every Morning To Avoid Pain
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Will Harlow, over-50s specialist physiotherapist, recommends these three stretches be done daily for cumulative benefits over time, especially if you have arthritis, stiff joints, or similar morning pain:
The good-morning routine
These stretches are designed for people with arthritis and stiff joints, but if you experience any extra pain, or are aware of having some musculoskeletal irregularity, do seek professional advice (such as from a local physiotherapist). Otherwise, the three stretches he recommends are:
Quad hip flexor stretch
This one is performed while lying on your side in bed:
- Bring the top leg up toward your body, grab the shin, and pull the leg backward to stretch.
- Feel the stretch in the front of the leg (quadriceps and hip flexor).
- Hold for 30 seconds and repeat on both sides.
- Use a towel or band if you can’t reach your shin.
Book-opener
This one helps improve mobility in the lower and mid-back:
- Lie on your side with arms at a 90-degree angle in front of your body.
- Roll backward, opening the top arm while keeping legs in place.
- Hold for 20–30 seconds or repeat the movement several times.
- Optionally, allow your head to rotate for a neck stretch.
Calf stretch with chest-opener
This one combines a calf and chest stretch:
- Stand in a lunged position, keeping the back leg straight and heel down for the calf stretch.
- Place hands behind your head, open elbows, and lift your head slightly for a chest stretch.
- Hold for 20–30 seconds, then switch legs.
For more on all the above plus visual demonstrations, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

How To Recover Quickly From A Stomach Bug

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
How To Recover Quickly From A Stomach Bug
Is it norovirus, or did you just eat something questionable? We’re not doctors, let alone your doctors, and certainly will not try to diagnose from afar. And as ever, if unsure and/or symptoms don’t go away or do get worse, seek professional medical advice.
That out of the way, we can give some very good general-purpose tips for this one…
Help your immune system to help you
So far as you can, you want a happy healthy immune system. For the most part, we’d recommend the following things:
Beyond Supplements: The Real Immune-Boosters!
…but you probably don’t want to be exercising with a stomach bug, so perhaps sit that one out. Exercise is the preventative; what you need right now is rest.
Hydrate—but watch out
Hydration is critical for recovery especially if you have diarrhea, but drinking too much water too quickly will just make things worse. Great options for getting good hydration more slowly are:
- Peppermint tea
- (peppermint also has digestion-settling properties)
- Ginger tea
- See also: Ginger Does A Lot More Than You Think
- Broths
- These will also help replenish your sodium and other nutrients, gently. Chicken soup for your stomach, and all that. A great plant-based option is sweetcorn soup.
- By broths, we mean clear(ish) water-based soups. This is definitely not the time for creamier soups.
❝Milk and dairy products should be avoided for 24 to 48 hours as they can make diarrhea worse.
Initial dietary choices when refeeding should begin with soups and broth.❞
Source: American College of Gastroenterology
Other things to avoid
Caffeine stimulates the digestion in a way that can make things worse.
Fat is more difficult to digest, and should also be avoided until feeling better.
To medicate or not to medicate?
Loperamide (also known by the brand name Imodium) is generally safe when used as directed.
Click here to see its uses, dosage, side effects, and contraindications
Antibiotics may be necessary for certain microbial infections, but should not be anyone’s first-choice treatment unless advised otherwise by your doctor/pharmacist.
Note that if your stomach bug is not something that requires antibiotics, then taking antibiotics can actually make it worse as the antibiotics wipe out your gut bacteria that were busy helping fight whatever’s going wrong in there:
- Facing a new challenge: the adverse effects of antibiotics on gut microbiota and host immunity
- Antibiotics as major disruptors of gut microbiota
- Microbiotoxicity: antibiotic usage and its unintended harm to the microbiome
A gentler helper
If you want to give your “good bacteria” a hand while giving pathogens a harder time of it, then a much safer home remedy is a little (seriously, do not over do it; we are talking 1–2 tablespoons, or around 20ml) apple cider vinegar, taken diluted in a glass of water.
❝Several studies indicate apple cider vinegar (ACV)’s usefulness in lowering postprandial glycemic response, specifically by slowing of gastric motility❞
(Slowing gastric motility is usually exactly what you want in the case of a stomach bug, and apple cider vinegar)
See also:
- Antimicrobial activity of apple cider vinegar against Escherichia coli, Staphylococcus aureus and Candida albicans
- Antibacterial apple cider vinegar eradicates methicillin resistant Staphylococcus aureus and resistant Escherichia coli
Take care!
Share This Post
- Peppermint tea
-

The Two-Second Advantage – by Vivek Ranadive and Kevin Maney
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The titular “two-second advantage” can in some cases be literal (imagine you got a two-second head-start in a boxing match!), in other cases can refer to being just a little ahead of things in a way that can confer a great advantage, often cumulatively—as anyone who’s played Monopoly can certainly attest.
Vivek Ranadivé and Kevin Maney give us lots of examples from business, sports, politics, economics, and more, in a way that seeks to cultivate a habit of asking the right questions in order to anticipate the future and not just be ahead of the competition—some areas of life don’t have competition for most people, like health, for example—but to generally have things “in hand”.
When it comes to personal finances, health, personal projects, and the like, those tiny initial advantages that lead to incremental further improvements, can be the difference between continually (and frantically) playing catch-up, or making the jump past breaking even to going from strength to strength.
Share This Post
-

Retrain Your Brain – by Dr. Seth Gillihan
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
15-Minute Arabic”, “Sharpen Your Chess Tactics in 24 Hours”, “Change Your Life in 7 Days”, “Cognitive Behavioral Therapy in 7 weeks”—all real books from this reviewer’s shelves.
The thing with books with these sorts of time periods in the titles is that the time period in the title often bears little relation to how long it takes to get through the book. So what’s the case here?
You’ll probably get through it in more like 7 days, but the pacing is more important than the pace. By that we mean:
Dr. Gillihan starts by assuming the reader is at best “in a rut”, and needs to first pick a direction to head in (the first “week”) and then start getting one’s life on track (the second “week”).
He then gives us, one by one, an array of tools and power-ups to do increasingly better. These tools aren’t just CBT, though of course that features prominently. There’s also mindfulness exercises, and holistic / somatic therapy too, for a real “bringing it all together” feel.
And that’s where this book excels—at no point is the reader left adrift with potential stumbling-blocks left unexamined. It’s a “whole course”.
Bottom line: whether it takes you 7 hours or 7 months, “Cognitive Behavioral Therapy in 7 Weeks” is a CBT-and-more course for people who like courses to work through. It’ll get you where you’re going… Wherever you want that to be for you!
Share This Post
-

The Vagus Nerve (And How You Can Make Use Of It)
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Vagus Nerve: The Brain-Gut Highway
The longest cranial nerve is the vagus nerve; it runs all the way from your brain to your colon. It’s very important, and (amongst other tasks) it largely regulates your parasympathetic nervous system, and autonomous functions like:
- Breathing
- Heart rate
- Vasodilation & vasoconstriction
- Blood pressure
- Reflex actions (e.g. coughing, sneezing, swallowing, vomiting, hiccuping)
That’s great, but how does knowing about it help us?
Because of vagal maneuvers! This means taking an action to stimulate the vagus nerve, and prompt it to calm down various bodily functions that need calming down. This can take the form of:
- Massage
- Electrostimulation
- Diaphragmatic breathing
Massage is perhaps the simplest; “vagus” means “wandering”, and the nerve is accessible in various places, including behind the ears. That’s the kind of thing that’ easier to show than tell, though, so we’ll include a video at the end.
Electrostimulation is the fanciest, and has been used to treat migraines and cluster headaches. Check out, for example:
Update on noninvasive neuromodulation for migraine treatment-Vagus nerve stimulation
Diaphragmatic breathing means breathing from the diaphragm—the big muscular tissue that sits under your lungs. You might know it as “abdominal breathing”, and refers to breathing “to the abdomen” rather than merely to the chest.
Even though your lungs are obviously in your chest not your abdomen, breathing with a focus on expanding the abdomen (rather than the chest) when breathing in, will result in much deeper breathing as the diaphragm allows the lungs to fill downwards as well as outwards.
Why this helps when it comes to the vagus nerve is simply that the vagus nerve passes by the diaphragm, such that diaphragmatic breathing will massage the vagus nerve deep inside your body.
More than just treating migraines
Vagus nerve stimulation has also been researched and found potentially helpful for managing:
- Depression, inflammation, and heart disease
- Diabetes and glycemic issues in general
- Multiple sclerosis and autoimmune disease in general
- Alzheimer’s disease and dementia in general
- Rheumatoid arthritis (we already mentioned inflammation and autoimmune diseases, but this is an interesting paper so we included it)
All this is particularly important as we get older, because vagal response reduces with age, and vagus nerve stimulation, which improves vagal tone, makes it easier not just to manage the aforementioned maladies, but also simply to relax more easily and more deeply.
See: Influence of age and gender on autonomic regulation of heart
We promised a video for the massage, so here it is:
! Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Is Cutting Calories The Key To Healthy Long Life?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Caloric Restriction with Optimal Nutrition

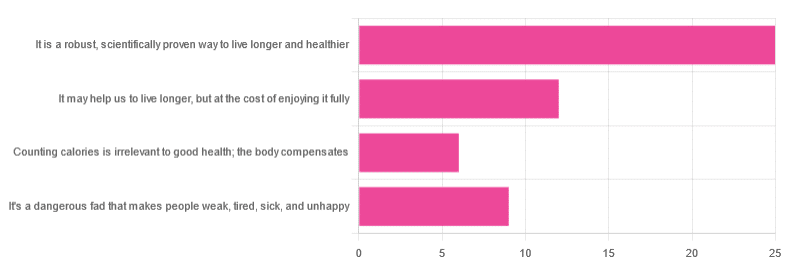
Yesterday, we asked you “What is your opinion of caloric restriction as a health practice?” and got the above-depicted, below-described spread of responses:
- 48% said “It is a robust, scientifically proven way to live longer and healthier”
- 23% said “It may help us to live longer, but at the cost of enjoying it fully”
- 17% said “It’s a dangerous fad that makes people weak, tired, sick, and unhealthy”
- 12% said “Counting calories is irrelevant to good health; the body compensates”
So… What does the science say?
A note on terms, first
“Caloric restriction” (henceforth: CR), as a term, sees scientific use to mean anything from a 25% reduction to a 50% reduction, compared to metabolic base rate.
This can also be expressed the other way around, “dropping to 60% of the metabolic base rate” (i.e., a 40% reduction).
Here we don’t have the space to go into much depth, so our policy will be: if research papers consider it CR, then so will we.
A quick spoiler, first
The above statements about CR are all to at least some degree True in one way or another.
However, there are very important distinctions, so let’s press on…
CR is a robust, scientifically proven way to live longer and healthier: True or False?
True! This has been well-studied and well-documented. There’s more science for this than we could possibly list here, but here’s a good starting point:
❝Calorie restriction (CR), a nutritional intervention of reduced energy intake but with adequate nutrition, has been shown to extend healthspan and lifespan in rodent and primate models.
Accumulating data from observational and randomized clinical trials indicate that CR in humans results in some of the same metabolic and molecular adaptations that have been shown to improve health and retard the accumulation of molecular damage in animal models of longevity.
In particular, moderate CR in humans ameliorates multiple metabolic and hormonal factors that are implicated in the pathogenesis of type 2 diabetes, cardiovascular diseases, and cancer, the leading causes of morbidity, disability and mortality❞
Source: Ageing Research Reviews | Calorie restriction in humans: an update
See also: Caloric restriction in humans reveals immunometabolic regulators of health span
We could devote a whole article (or a whole book, really) to this, but the super-short version is that it lowers the metabolic “tax” on the body and allows the body to function better for longer.
CR may help us to live longer, but at the cost of enjoying it fully: True or False?
True or False, contingently, depending on what’s important to you. And that depends on psychology as much as physiology, but it’s worth noting that there is often a selection bias in the research papers; people ill-suited to CR drop out of the studies and are not counted in the final data.
Also, relevant for a lot of our readers, most (human-based) studies recruit people over 18 and under 60. So while it is reasonable to assume the same benefits will be carried over that age, there is not nearly as much data for it.
Studies into CR and Health-Related Quality of Life (HRQoL) have been promising, and/but have caveats:
❝In non-obese adults, CR had some positive effects and no negative effects on HRQoL.❞
❝We do not know what degree of CR is needed to achieve improvements in HRQoL, but we do know it requires an extraordinary amount of support.
Therefore, the incentive to offer this intervention to a low-risk, normal or overweight individual is lacking and likely not sustainable in practice.❞
CR a dangerous fad that makes people weak, tired, sick, and unhealthy: True or False?
True if it is undertaken improperly, and/or without sufficient support. Many people will try CR and forget that the idea is to reduce metabolic load while still getting good nutrition, and focus solely on the calorie-counting.
So for example, if a person “saves” their calories for the day to have a night out in a bar where they drink their calories as alcohol, then this is going to be abysmal for their health.
That’s an extreme example, but lesser versions are seen a lot. If you save your calories for a pizza instead of a night of alcoholic drinks, then it’s not quite so woeful, but for example the nutrition-to-calorie ratio of pizza is typically not great. Multiply that by doing it as often as not, and yes, someone’s health is going to be in ruins quite soon.
Counting calories is irrelevant to good health; the body compensates: True or False?
True if by “good health” you mean weight loss—which is rarely, if ever, what we mean by “good health” here at 10almonds (unless we clarify such), but it’s a very common association and indeed, for some people it’s a health goal. You cannot sustainably and healthily lose weight by CR alone, especially if you’re not getting optimal nutrition.
Your body will notice that you are starving, and try to save you by storing as much fat as it can, amongst other measures that will similarly backfire (cortisol running high, energy running low, etc).
For short term weight loss though, yes, it’ll work. At a cost. That we don’t recommend.
❝By itself, decreasing calorie intake will have a limited short-term influence.❞
Source: Reducing Calorie Intake May Not Help You Lose Body Weight
See also…
❝Caloric restriction is a commonly recommended weight-loss method, yet it may result in short-term weight loss and subsequent weight regain, known as “weight cycling”, which has recently been shown to be associated with both poor sleep and worse cardiovascular health❞
Source: Dieting Behavior Characterized by Caloric Restriction
In summary…
Caloric restriction is a well-studied area of health science. We know:
- Practised well, it can extend not only lifespan, but also healthspan
- Practised well, it can improve mood, energy, sexual function, and the other things people fear losing
- Practised badly, it can be ruinous to the health—it is critical to practise caloric restriction with optimal nutrition.
- Practised badly, it can lead to unhealthy weight loss and weight regain
One final note…
If you’ve tried CR and hated it, and you practised it well (e.g., with optimal nutrition), then we recommend just not doing it.
You could also try intermittent fasting instead, for similar potential benefits. If that doesn’t work out either, then don’t do that either!
Sometimes, we’re just weird. It can often be because of a genetic or epigenetic quirk. There are usually workarounds, and/but not everything that’s right for most people will be right for all of us.
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Remember – by Dr. Lisa Genova
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Memory is often viewed as one thing—either you have a good memory, or you don’t. At best, a lot of people have a vague idea of selective memory. But, the reality is much more complex—and much more interesting.
Dr. Genova lays out clearly and simply the various different kinds of memory, how they work, and how they fail. Some of these kinds of memory operate on completely different principles than others, and/or in different parts of the brain. And, it’s not just “a memory for faces” or a “memory for names”, nor even “short term vs long term”. There’s working memory, explicit and implicit memory, semantic memory, episodic memory, muscle memory, and more.
However, this is not just an interesting book—it’s also a useful one. Dr. Genova also looks at how we can guard against failing memory in later years, and how we can expand and grow the kinds of memory that are most important to us.
The style of the book is very conversational, and not at all textbook-like. It’s certainly very accessible, and pleasant to read too.
Bottom line: memory is a weird and wonderful thing, and this book shines a clear light on many aspects of it—including how to improve the various different kinds of memory.
Click here to check out Remember (we recommend to do it now before you forget!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: