It’s A Wrap
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
We hope all our readers have had a great and healthy week! Here are some selections from health news from around the world:
A lack of transparency
Thousands of chemicals blanket-approved for food contact in packaging, under the FDA’s “Generally Recognized As Safe” umbrella, have been found in humans.
This highlights a gap in the safeguarding system, because the GRAS classification is given when there’s no known significant association with disease—but in this case, a problem can occur when the build-up in the blood and brain cause problems much later.
Read in full: Thousands of toxins from food packaging found in humans – research
Learn more: We Are Such Stuff As Bottles Are Made Of (It’s Not Fantastic To Be Plastic)
Cafestol for weight loss?
Most coffee intervention studies use instant coffee. Which is understandable; they are scientists on a budget, not coffee shop baristas. But, instant coffee is low in some of coffee’s important compounds, such as cafestol—which as it turns out, can lower not only overall body fat, but also (importantly!) visceral fat.
Read in full: 12-week coffee compound study shows promising results for weight and fat reduction in at-risk individuals
Learn more: The Bitter Truth About Coffee (or is it?)
Doing something is better than doing nothing
While a lot of the bad news both locally and around the world can be infuriating and/or depressing, turning a blind eye may not be the best approach for dealing with it. This study was in teens, but it’s likely that the benefits are similar for other ages too:
Read in full: Racial justice activism, advocacy found to reduce depression, anxiety in some teens
Learn more: Make Social Media Work For Your Mental Health
A ray of hope!
Sometimes, the topic of sun and sunscreens can seem like “damned if you do; damned if you don’t”, with regard to the harmful effects of the sun, and in some cases, potentially harmful effects of some sunscreen chemicals. We’ve argued ultimately in favor of sunscreens in this tug-of-war, but it’s nice to see improvements being made, in this case, with lignin-based sunscreen (a plant-based by-product of the pulp industry).
Read in full: Researchers create high-performing, eco-friendly sunscreen
Learn more: Who Screens The Sunscreens?
All about the pores
Researchers have identified a protein, and from that, a stack of protein fragments, that are involved in the formation of large pores. This is important, as it’s pointing to a means of relief for a lot of inflammatory diseases.
Read in full: Scientists unravel the process of pore formation in cells
Learn more: Why Do We Have Pores, And Could We Not?
Getting to the bottom of Crohn’s
If you have Crohn’s, or perhaps someone close to you has it, then you’ll be familiar with the common medical refrain of “we don’t know”. While this honesty is laudable, it’s not reassuring. So, it’s good that researchers are making progress in understanding why many people with Crohn’s may respond differently not only to lifestyle interventions, but also to various relevant drugs—allowing doctors to prescribe the right treatment for the right person.
Read in full: Patient-derived gut organoids reveal new insights into Crohn’s disease subtypes
Learn more: Diet Tips for Crohn’s Disease
Another carotenoid that holds back Alzheimer’s
Phytoene is a carotenoid that is found in many red, orange, or yellow foods, including tomatoes, carrots, apricots, red peppers, oranges, mandarins and passion fruit, among others. Researchers have found that it slows the onset of symptoms associated with the formation of amyloid plaques, by 30–40%, and increases longevity by 10–19%:
Read in full: Carotenoid phytoene shows potential in slowing Alzheimer’s plaque formation and increasing lifespan
Learn more: Brain Food? The Eyes Have It! ← this is about a different carotenoid, lutein, found mostly in dark green leafy vegetables, but it’s best to enjoy both 😎
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Psychology Sunday: Family Estrangement & How To Fix It

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Estrangement, And How To Heal It
We’ve written before about how deleterious to the health loneliness and isolation can be, and what things can be done about it. Today, we’re tackling a related but different topic.
We recently had a request to write about…
❝Reconciliation of relationships in particular estrangement mother adult daughter❞
And, this is not only an interesting topic, but a very specific one that affects more people than is commonly realized!
In fact, a recent 800-person study found that more than 43% of people experienced family estrangement of one sort or another, and a more specific study of more than 2,000 mother-child pairs found that more than 11% of mothers were estranged from at least one adult child.
So, if you think of the ten or so houses nearest to you, probably at least one of them contains a parent estranged from at least one adult child. Maybe it’s yours. Either way, we hope this article will give you some pause for thought.
Which way around?
It makes a difference to the usefulness of this article whether any given reader experiencing estrangement is the parent or the adult child. We’re going to assume the reader is the parent. It also makes a difference who did the estranging. That’s usually the adult child.
So, we’re broadly going to write with that expectation.
Why does it happen?
When our kids are small, we as parents hold all the cards. It may not always feel that way, but we do. We control our kids’ environment, we influence their learning, we buy the food they eat and the clothes they wear. If they want to go somewhere, we probably have to take them. We can even set and enforce rules on a whim.
As they grow, so too does their independence, and it can be difficult for us as parents to relinquish control, but we’re going to have to at some point. Assuming we are good parents, we just hope we’ve prepared them well enough for the world.
Once they’ve flown the nest and are living their own adult lives, there’s an element of inversion. They used to be dependent on us; now, not only do they not need us (this is a feature not a bug! If we have been good parents, they will be strong without us, and in all likelihood one day, they’re going to have to be), but also…
We’re more likely to need them, now. Not just in the “oh if we have kids they can look after us when we’re old” sense, but in that their social lives are growing as ours are often shrinking, their family growing, while ours, well, it’s the same family but they’re the gatekeepers to that now.
If we have a good relationship, this goes fine. However, it might only take one big argument, one big transgression, or one “final straw”, when the adult child decides the parent is more trouble than they’re worth.
And, obviously, that’s going to hurt. But it’s pretty much how it pans out, according to studies:
Here be science: Tensions in the Parent and Adult Child Relationship: Links to Solidarity and Ambivalence
How to fix it, step one
First, figure out what went wrong.
Resist any urge to protect your own feelings with a defensive knee-jerk “I don’t know; I was a good, loving parent”. That’s a very natural and reasonable urge and you’re quite possibly correct, but it won’t help you here.
Something pushed them away. And, it will almost certainly have been a push factor from you, not a pull factor from whoever is in their life now. It’s easy to put the blame externally, but that won’t fix anything.
And, be honest with yourself; this isn’t a job interview where we have to present a strength dressed up as a “greatest weakness” for show.
You can start there, though! If you think “I was too loving”, then ok, how did you show that love? Could it have felt stifling to them? Controlling? Were you critical of their decisions?
It doesn’t matter who was right or wrong, or even whether or not their response was reasonable. It matters that you know what pushed them away.
How to fix it, step two
Take responsibility, and apologize. We’re going to assume that your estrangement is such that you can, at least, still get a letter to them, for example. Resist the urge to argue your case.
Here’s a very good format for an apology; please consider using this template:
The 10-step (!) apology that’s so good, you’ll want to make a note of it
You may have to do some soul-searching to find how you will avoid making the same mistake in the future, that you did in the past.
If you feel it’s something you “can’t change”, then you must decide what is more important to you. Only you can make that choice, but you cannot expect them to meet you halfway. They already made their choice. In the category of negotiation, they hold all the cards now.
How to fix it, step three
Now, just wait.
Maybe they will reply, forgiving you. If they do, celebrate!
Just be aware that once you reconnect is not the time to now get around to arguing your case from before. It will never be the time to get around to arguing your case from before. Let it go.
Nor should you try to exact any sort of apology from them for estranging you, or they will at best feel resentful, wonder if they made a mistake in reconnecting, and withdraw.
Instead, just enjoy what you have. Many people don’t get that.
If they reply with anger, maybe it will be a chance to reopen a dialogue. If so, family therapy could be an approach useful for all concerned, if they are willing. Chances are, you all have things that you’d all benefit from talking about in a calm, professional, moderated, neutral environment.
You might also benefit from a book we reviewed previously, “Parent Effectiveness Training”. This may seem like “shutting the stable door after the horse has bolted”, but in fact it’s a very good guide to relationship dynamics in general, and extensively covers relations between parents and adult children.
If they don’t reply, then, you did your part. Take solace in knowing that much.
Some final thoughts:
At the end of the day, as parents, our kids living well is (hopefully) testament to that we prepared them well for life, and sometimes, being a parent is a thankless task.
But, we (hopefully) didn’t become parents for the plaudits, after all.
Share This Post
-

Benefits of Different Tropical Fruits
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? You can always hit “reply” to any of our emails, or use the feedback widget at the bottom!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small
❝Would very much like your views of the benefits of different tropical fruits. I do find papaya is excellent for settling the digestion – but keen to know if others have remarkable qualities.❞
Definitely one for a main feature sometime soon! As a bonus while you wait, pineapple has some unique and powerful properties:
❝Its properties include: (1) interference with growth of malignant cells; (2) inhibition of platelet aggregation*; (3) fibrinolytic activity; (4) anti-inflammatory action; (5) skin debridement properties. These biological functions of bromelain, a non-toxic compound, have therapeutic values in modulating: (a) tumor growth; (b) blood coagulation; (c) inflammatory changes; (d) debridement of third degree burns; (e) enhancement of absorption of drugs.❞
*so do be aware of this if you are on blood thinners or otherwise have a bleeding disorder, as you might want to skip the pineapple in those cases!
Source: Bromelain, the enzyme complex of pineapple (Ananas comosus) and its clinical application. An update
Enjoy!
Share This Post
-

Are You A Calorie-Burning Machine?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Burn, Calorie, Burn

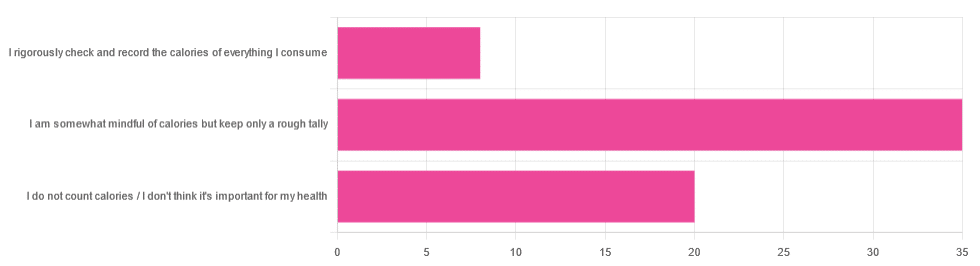
In Tuesday’s newsletter, we asked you whether you count calories, and got the above-depicted, below-described set of answers:
- About 56% said “I am somewhat mindful of calories but keep only a rough tally”
- About 32% said “I do not count calories / I don’t think it’s important for my health”
- About 13% said “I rigorously check and record the calories of everything I consume”
So what does the science say, about the merits of all these positions?
A food’s calorie count is a good measure of how much energy we will, upon consuming the food, have to use or store: True or False?
False, broadly. It can be, at best, a rough guideline. Do you know what a calorie actually is, by the way? Most people don’t.
One thing to know before we get to that: there’s “cal” vs “kcal”. The latter is generally used when it comes to foodstuffs, and it’s what we’ll be meaning whenever we say “calorie” here. 1cal is 1/1000th of a kcal, that’s all.
Now, for what a calorie actually is:
A calorie is the amount of energy needed to raise the temperature of 1 liter of water by 1℃
Question: so, how to we measure how much food is needed to do that?
Answer: by using a bomb calorimeter! Which is the exciting name for the apparatus used to literally burn food and capture the heat produced to indeed raise the temperature of 1 liter of water by 1℃.
If you’re having trouble imagining such equipment, here it is:
Bomb Calorimeter: Definition, Construction, & Operation (with diagram and FAQs)
The unfortunate implication of the above information
A kilogram of sawdust contains about a 1000 kcal, give or take what wood was used and various other conditions.
However, that does not mean you can usefully eat the sawdust. In other words:
Calorie count tells us only how good something is at raising the temperature of water if physically burned.
Now do you see why oils and sugars have such comparably high calorie counts?
And while we may talk about “burning calories” as a metaphor, we do not, in fact, have a little wood stove inside us burning the food we eat.
A calorie is a calorie: True or False?
Definitely False! Building on from the above… We will get very little energy from sawdust; it’s not just that we can’t use it; we can’t store it either; it’ll mostly pass through as fiber.
(however, please do not use sawdust to get your daily dose of fiber either, as it is not safe for human consumption and may give you diseases, depending on what is lurking in it)
But let’s look at oil and sugar, two very high-calorie categories of food, because they’re really easy to physically burn and they give off a good flame.
A bomb calorimeter may treat them quite equally, but to our body, they are metabolically very different indeed.
For a start, most sugars will get absorbed and processed much more quickly than most oils, and that can overwhelm the liver (responsible for glycogen management), and lead to non-alcoholic fatty liver disease, diabetes, and more. Metabolic syndrome in general, and if you keep it up too much and you may find it’s now a lottery between dying of NAFLD, diabetes, or heart disease (it’ll usually be the heart disease that kills).
See also:
- Which Sugars Are Healthier, And Which Are Just The Same?
- 10 Ways To Balance Blood Sugars
- How To Unfatty A Fatty Liver
Meanwhile, we know all about the different kinds of nutritional profiles that oils can have, and some can promote having high energy without putting on fat, while others can strain the heart. Not even “a fat is a fat”, so “a calorie is a calorie” doesn’t get much mileage outside of a bomb calorimeter!
See also:
A calorie-controlled / calorie-restricted diet is an effective weight loss strategy: True or False?
True, usually! Surprise!
- On the one hand: calories are a wildly imprecise way to reckon the value of food, and using them as a guide to health can be dangerously misleading
- On the other hand: the very activity of calorie-counting itself promotes mindful eating, which is very good for the health
There is a strong difference between the mind of somebody who is carefully logging their pre-bedtime piece of chocolate and reflecting on its nutritional value, vs someone who isn’t sure whether this is their second or third glass of wine, nor how much the glass contained.
So if you want to get most of the benefits of a calorie-controlled diet without counting calories, you may try taking a “mindful eating” approach to diet.
However! If you want to do this for weight loss, be aware, that you will have to practice it all the time, not just for one meal here and there.
You can read more on how to do “mindful eating” here:
Dr. Rupy Aujla: The Kitchen Doctor | Mindful Eating & Interoception
Take care!
Share This Post


Related Posts
-

The Philosophy Gym – by Dr. Stephen Law
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
If you’d like to give those “little gray cells” an extra workout, this book is a great starting place.
Dr. Stephen Law is Director of Philosophy at the Department of Continuing Education, University of Oxford. As such, he’s no stranger to providing education that’s both attainable and yet challenging. Here, he lays out important philosophical questions, and challenges the reader to get to grips with them in a systematic fashion.
Each of the 25 questions/problems has a chapter devoted to it, and is ranked:
- Warm-up
- Moderate
- More Challenging
But, he doesn’t leave us to our own devices, nor does he do like a caricature of a philosopher and ask us endless rhetorical questions. Instead, he looks at various approaches taken by other philosophers over time, and invites the reader to try out those methods.
The real gain of this book is not the mere enjoyment of reading, but rather in taking those thinking skills and applying them in life… because most if not all of them do have real-world applications and/or implications too.
The book’s strongest point? That it doesn’t assume prior knowledge (and yet also doesn’t patronize the reader). Philosophy can be difficult to dip one’s toes into without a guide, because philosophers writing about philosophy can at first be like finding yourself at a party where you know nobody, but they all know each other.
In contrast, Law excels at giving quick, to-the-point ground-up summaries of key ideas and their progenitors.
In short: a wonderful way to get your brain doing things it might not have tried before!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Early Bird Or Night Owl? Genes vs Environment
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
A Sliding Slope?

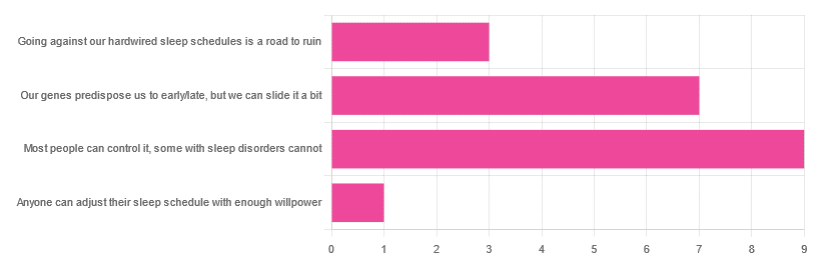
In Tuesday’s newsletter, we asked you how much control you believe we have over our sleep schedule, and got the above-depicted, below-described, set of responses:
- 45% said “most people can control it; some people with sleep disorders cannot
- 35% said “our genes predispose us to early/late, but we can slide it a bit
- 15% said: “going against our hardwired sleep schedules is a road to ruin”
- 5% said “anyone can adjust their sleep schedule with enough willpower”
You may be wondering: what’s with those single-digit numbers in the graph there? And the answer is: Tuesday’s email didn’t go out at the usual time due to a scheduling mistake (sorry!), which is probably what affected the number of responses (poll response levels vary, but are usually a lot higher than this).
Note: yes, this does mean most people who read our newsletter don’t vote. So, not to sound like a politician on the campaign trail, but… Your vote counts! We always love reading your comments when you add those, too—often they provide context that allow us to tailor what we focus on in our articles
However, those are the responses we got, so here we are!
What does the science say?
Anyone can adjust their sleep with enough willpower: True or False?
False, simply. It’s difficult for most people, but for many people with sleep disorders, it is outright impossible.
In a battle of narcolepsy vs willpower, for example, no amount of willpower will stop the brain from switching to sleep mode when it thinks it’s time to sleep:
❝Narcolepsy is the most common neurological cause of chronic sleepiness. The discovery about 20 years ago that narcolepsy is caused by selective loss of the neurons producing orexins sparked great advances in the field
[There is also] developing evidence that narcolepsy is an autoimmune disorder that may be caused by a T cell-mediated attack on the orexin neurons and explain how these new perspectives can inform better therapeutic approaches.❞
~ Dr. Carrie Mahoney et al. (lightly edited for brevity)
Source: The neurobiological basis of narcolepsy
For further reading, especially if this applies to you or a loved one:
Our genes predispose us to early/late, but we can slide it a bit: True or False?
True! First, about our genes predisposing us:
…and also:
Gene distinguishes early birds from night owls and helps predict time of death
Now, as for the “can slide it a bit”, this is really just a function of the general categories of “early bird” and “night owl” spanning periods of time that allow for a few hours’ wiggle-room at either side.
However, it is recommended to make any actual changes more gradually, with the Sleep Foundation going so far as to recommend 30 minutes, or even just 15 minutes, of change per day:
Sleep Foundation | How to Fix Your Sleep Schedule
Going against our hardwired sleep schedule is a road to ruin: True or False?
False, contextually. By this we mean: our “hardwired” sleep schedule is (for most of us), genetically predisposed but not predetermined.
Also, genetic predispositions are not necessarily always good for us; one would not argue, for example, for avoiding going against a genetic predisposition to addiction.
Some genetic predispositions are just plain bad for us, and genes can be a bit of a lottery.
That said, we do recommend getting some insider knowledge (literally), by getting personal genomics tests done, if that’s a viable option for you, so you know what’s really a genetic trait (and what to do with that information) and what’s probably caused by something else (and what to do with that information):
Genetic Testing: Health Benefits & Methods
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Sunflower Oil vs Canola Oil – Which is Healthier?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Our Verdict
When comparing sunflower oil to canola oil, we picked the sunflower oil.
Why?
They’re both terrible! But canola oil is worse. Sunflower oil is marketed as being higher in polyunsaturated fats, which it is, albeit not by much.
Canola oil is very bad for the heart, and sunflower oil is only moderately bad for the heart, to the point that it can be heart-neutral if used sparingly.
As seed oils, they are both sources of vitamin E, but you’d need to drink a cup of oil to get your daily dose, so please just eat some seeds (or nuts, or fruit, or something) instead. It can even be sunflower seeds if you like! Rapeseed* itself (the seed that canola oil is made from) isn’t really sold as a foodstuff, so that one’s less of an option.
*Fun fact: if you’re N. American and wondering what this “rapeseed” is, know that most of the rest of the Anglosphere calls canola oil “rapeseed oil”, as it’s made from rapeseed, which comes from a plant called rape, whose name is unrelated to the crime of the same name, and comes from rāpa, the Latin word for turnip. Anyway, “canola” is a portmanteau of “Canadian” and “Ola” meaning oil, and is a trademark that has made its way into generic use throughout N. America, as a less alarming name.
Back to health matters: while sunflower seeds are healthy in moderation, the ultraprocessed and refined sunflower and canola oils are not.
Canola oil has also been found to be implicated in age-related cognitive decline, whereas sunflower oil has had mixed results in that regard.
In summary
Sunflower oil is relatively, and we stress relatively, healthier than canola oil. Please use a healthier oil than either if you can. Olive oil is good for most things, and if you need something with a higher smoke point (and/or less distinctive flavor), consider avocado oil, which is also very healthy and whose smoke point is even higher than the seed oils we’ve been discussing today.
Want to know more?
Check out:
Avocado Oil vs Olive Oil – Which is Healthier?
Enjoy!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: