Relieve GERD and Acid Reflux with Stretches and Exercises
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Looking for relief from GERD or acid reflux? Today we’re featuring an amazing video by Dr. Jo, packed with stretches and exercises designed to ease those symptoms.
Here’s a quick rundown, in case you don’t have time to watch the whole video.
If you’re not familiar with GERD, you can find our simple explanation of GERD here. Or, if you’re on the other end of the spectrum and want to do a deeper dive on the topic, we reviewed a great book on the topic).
1. Mobilize Your SEM Muscle
The sternocleidomastoid (SEM) muscle, if tight, can aggravate acid reflux. Dr. Jo shows how to gently mobilize this muscle by turning your head while holding the SEM in place. It’s simple but effective.
2. Portrait Pose Stretch
Stretch out that SEM with the Portrait Pose. Place your hand on your collarbone, turn your head away, side bend, and look up. Hold for 30 seconds. You’ll feel the tension melting away.
3. Seated Cat-Cow Motion
Open up your stomach area with this easy exercise. Sit down, roll your body forward, arch your back (Cow), then curl your spine and tuck your chin (Cat). Alternate for 30 seconds and feel the difference.
4. Quadruped Cat-Cow with Breathing
Similar to the seated cat-cow, the quadruped cat-cow focuses on flexing the lower spine whilst on all fours. Bonus tip: focus on deep belly breathing during the exercise. This helps improve digestion and ease reflux symptoms.
5. Exaggerated Pelvic Tilt
Lie on your back and tilt your pelvis back and forth. This loosens up the abdominal area and helps everything flow better.
6. Trunk Rotation
Lie down, bend your knees, and rotate them to one side. Hold for 30 seconds, then switch sides. It’s a great way to relax and stretch your abdominal muscles.
We know this is a quick overview (sorry if it seems rushed!), but if you have a few more minutes on your hand you can watch the whole video below.
Feel better soon! And if you have any favorite tips or videos to share, email us at 10almonds.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.

Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
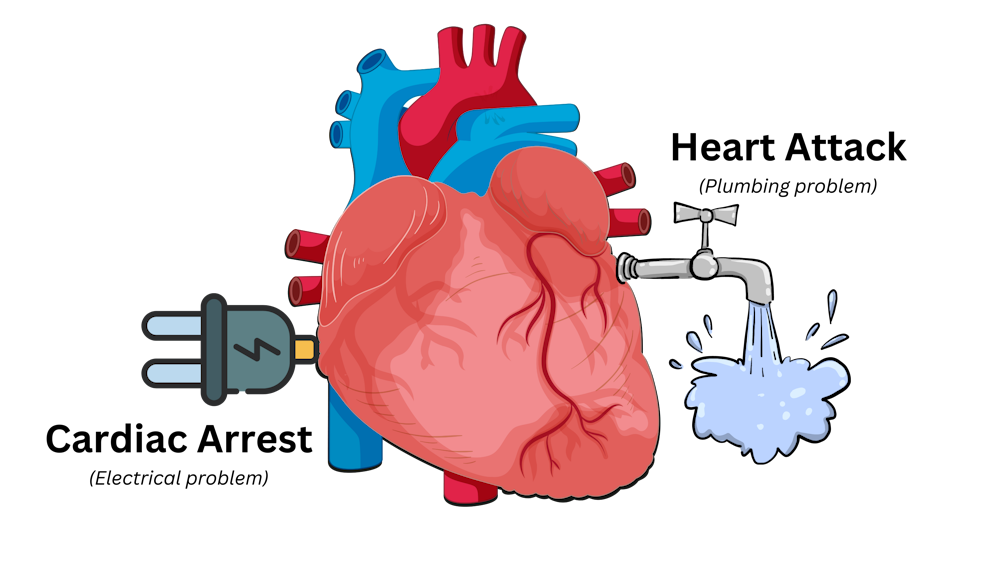
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-

Statins: His & Hers?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The Hidden Complexities of Statins and Cardiovascular Disease (CVD)

This is Dr. Barbara Roberts. She’s a cardiologist and the Director of the Women’s Cardiac Center at one of the Brown University Medical School teaching hospitals. She’s an Associate Clinical Professor of Medicine and takes care of patients, teaches medical students, and does clinical research. She specializes in gender-specific aspects of heart disease, and in heart disease prevention.
We previously reviewed Dr. Barbara Roberts’ excellent book “The Truth About Statins: Risks and Alternatives to Cholesterol-Lowering Drugs”. It prompted some requests to do a main feature about Statins, so we’re doing it today. It’s under the auspices of “Expert Insights” as we’ll be drawing almost entirely from Dr. Roberts’ work.
So, what are the risks of statins?
According to Dr. Roberts, one of the biggest risks is not just drug side-effects or anything like that, but rather, what they simply won’t treat. This is because statins will lower LDL (bad) cholesterol levels, without necessarily treating the underlying cause.
Imagine you got Covid, and it’s one of the earlier strains that’s more likely deadly than “merely” debilitating.
You’re coughing and your throat feels like you gargled glass.
Your doctor gives you a miracle cough medicine that stops your coughing and makes your throat feel much better.
(Then a few weeks later, you die, because this did absolutely nothing for the underlying problem)
You see the problem?
Are there problematic side-effects too, though?
There can be. But of course, all drugs can have side effects! So that’s not necessarily news, but what’s relevant here is the kind of track these side-effects can lead one down.
For example, Dr. Roberts cites a case in which a woman’s LDL levels were high and she was prescribed simvastatin (Zocor), 20mg/day. Here’s what happened, in sequence:
- She started getting panic attacks. So, her doctor prescribed her sertraline (Zoloft) (a very common SSRI antidepressant) and when that didn’t fix it, paroxetine (Paxil). This didn’t work either… because the problem was not actually her mental health. The panic attacks got worse…
- Then, while exercising, she started noticing progressive arm and leg weakness. Her doctor finally took her off the simvastatin, and temporarily switched to ezetimibe (Zetia), a less powerful nonstatin drug that blocks cholesterol absorption, which change eased her arm and leg problem.
- As the Zetia was a stopgap measure, the doctor put her on atorvastatin (Lipitor). Now she got episodes of severe chest pressure, and a skyrocketing heart rate. She also got tremors and lost her body temperature regulation.
- So the doctor stopped the atorvastatin and tried rosovastatin (Crestor), on which she now suffered exhaustion (we’re not surprised, by this point) and muscle pains in her arms and chest.
- So the doctor stopped the rosovastatin and tried lovastatin (Mevacor), and now she had the same symptoms as before, plus light-headedness.
- So the doctor stopped the lovastatin and tried fluvastatin (Lescol). Same thing happened.
- So he stopped the fluvastatin and tried pravastatin (Pravachol), without improvement.
- So finally he took her off all these statins because the high LDL was less deleterious to her life than all these things.
- She did her own research, and went back to the doctor to ask for cholestyramine (Questran), which is a bile acid sequestrent and nothing to do with statins. She also asked for a long-acting niacin. In high doses, niacin (one of the B-vitamins) raises HDL (good) cholesterol, lowers LDL, and lowers tryglycerides.
- Her own non-statin self-prescription (with her doctor’s signature) worked, and she went back to her life, her work, and took up running.
Quite a treatment journey! Want to know more about the option that actually worked?
Read: Bile Acid Resins or Sequestrants
What are the gender differences you/she mentioned?
Actually mostly sex differences, since this appears to be hormonal (which means that if your hormones change, so will your risk). A lot of this is still pending more research—basically it’s a similar problem in heart disease to one we’ve previously talked about with regard to diabetes. Diabetes disproportionately affects black people, while diabetes research disproportionately focuses on white people.
In this case, most heart disease research has focused on men, with women often not merely going unresearched, but also often undiagnosed and untreated until it’s too late. And the treatments, if prescribed? Assumed to be the same as for men.
Dr. Roberts tells of how medicine is taught:
❝When I was in medical school, my professors took the “bikini approach” to women’s health: women’s health meant breasts and reproductive organs. Otherwise the prototypical patient was presented as a man.❞
There has been some research done with statins and women, though! Just, still not a lot. But we do know for example that some statins can be especially useful for treating women’s atherosclerosis—with a 50% success rate, rather than 31% for men.
For lowering LDL itself, however, it can work but is generally not so hot in women.
Fun fact:
In men:
- High total cholesterol
- High non-HDL cholesterol
- High LDL cholesterol
- Low HDL cholesterol
…are all significantly associated with an increased risk of death from CVD.
In women:
…levels of LDL cholesterol even more than 190 were associated with only a small, statistically insignificant increased risk of dying from CVD.
So…
The fact that women derive less benefit from a medicine that mainly lowers LDL cholesterol, may be because elevated LDL cholesterol is less harmful to women than it is to men.
And also: Treatment and Response to Statins: Gender-related Differences
And for that matter: Women Versus Men: Is There Equal Benefit and Safety from Statins?*
Definitely a case where Betteridge’s Law of Headlines applies!
What should women do to avoid dying of CVD, then?
First, quick reminder of our general disclaimer: we can’t give medical advice and nothing here comprises such. However… One particularly relevant thing we found illuminating in Dr. Roberts’ work was this observation:
The metabolic syndrome is diagnosed if you have three (or more) out of five of the following:
- Abdominal obesity (waist >35″ if a woman or >40″ if a man)
- Fasting blood sugars of 100mg/dl or more
- Fasting triglycerides of 150mg/dl or more
- Blood pressure of 130/85 or higher
- HDL <50 if a woman or <40 if a man
And yet… because these things can be addressed with exercise and a healthy diet, which neither pharmaceutical companies nor insurance companies have a particular stake in, there’s a lot of focus instead on LDL levels (since there are a flock of statins that can be sold be lower them)… Which, Dr. Roberts says, is not nearly as critical for women.
So women end up getting prescribed statins that cause panic attacks and all those things we mentioned earlier… To lower our LDL, which isn’t nearly as big a factor as the other things.
In summary:
Statins do have their place, especially for men. They can, however, mask underlying problems that need treatment—which becomes counterproductive.
When it comes to women, statins are—in broad terms—statistically not as good. They are a little more likely to be helpful specifically in cases of atherosclerosis, whereby they have a 50/50 chance of helping.
For women in particular, it may be worthwhile looking into alternative non-statin drugs, and, for everyone: diet and exercise.
Further reading: How Can I Safely Come Off Statins?
Share This Post
-

We’re the ‘allergy capital of the world’. But we don’t know why food allergies are so common in Australian children
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Australia has often been called the “allergy capital of the world”.
An estimated one in ten Australian children develop a food allergy in their first 12 months of life. Research has previously suggested food allergies are more common in infants in Australia than infants living in Europe, the United States or Asia.
So why are food allergies so common in Australia? We don’t know exactly – but local researchers are making progress in understanding childhood allergies all the time.
Miljan Zivkovic/Shutterstock What causes food allergies?
There are many different types of reactions to foods. When we refer to food allergies in this article, we’re talking about something called IgE-mediated food allergy. This type of allergy is caused by an immune response to a particular food.
Reactions can occur within minutes of eating the food and may include swelling of the face, lips or eyes, “hives” or welts on the skin, and vomiting. Signs of a severe allergic reaction (anaphylaxis) include difficulty breathing, swelling of the tongue, swelling in the throat, wheeze or persistent cough, difficulty talking or a hoarse voice, and persistent dizziness or collapse.
Recent results from Australia’s large, long-running food allergy study, HealthNuts, show one in ten one-year-olds have a food allergy, while around six in 100 children have a food allergy at age ten.
A food allergy can present with skin reactions. comzeal images/Shutterstock In Australia, the most common allergy-causing foods include eggs, peanuts, cow’s milk, shellfish (for example, prawn and lobster), fish, tree nuts (for example, walnuts and cashews), soybeans and wheat.
Allergies to foods like eggs, peanuts and cow’s milk often present for the first time in infancy, while allergies to fish and shellfish may be more common later in life. While most children will outgrow their allergies to eggs and milk, allergy to peanuts is more likely to be lifelong.
Findings from HealthNuts showed around three in ten children grew out of their peanut allergy by age six, compared to nine in ten children with an allergy to egg.
Are food allergies becoming more common?
Food allergies seem to have become more common in many countries around the world over recent decades. The exact timing of this increase is not clear, because in most countries food allergies were not well measured 40 or 50 years ago.
We don’t know exactly why food allergies are so common in Australia, or why we’re seeing a rise around the world, despite extensive research.
But possible reasons for rising allergies around the world include changes in the diets of mothers and infants and increasing sanitisation, leading to fewer infections as well as less exposure to “good” bacteria. In Australia, factors such as increasing vitamin D deficiency among infants and high levels of migration to the country could play a role.
In several Australian studies, children born in Australia to parents who were born in Asia have higher rates of food allergies compared to non-Asian children. On the other hand, children who were born in Asia and later migrated to Australia appear to have a lower risk of nut allergies.
Meanwhile, studies have shown that having pet dogs and siblings as a young child may reduce the risk of food allergies. This might be because having pet dogs and siblings increases contact with a range of bacteria and other organisms.
This evidence suggests that both genetics and environment play a role in the development of food allergies.
We also know that infants with eczema are more likely to develop a food allergy, and trials are underway to see whether this link can be broken.
Can I do anything to prevent food allergies in my kids?
One of the questions we are asked most often by parents is “can we do anything to prevent food allergies?”.
We now know introducing peanuts and eggs from around six months of age makes it less likely that an infant will develop an allergy to these foods. The Australasian Society of Clinical Immunology and Allergy introduced guidelines recommending giving common allergy-causing foods including peanut and egg in the first year of life in 2016.
Our research has shown this advice had excellent uptake and may have slowed the rise in food allergies in Australia. There was no increase in peanut allergies between 2007–11 to 2018–19.
Introducing other common allergy-causing foods in the first year of life may also be helpful, although the evidence for this is not as strong compared with peanuts and eggs.
Giving kids peanuts early can reduce the risk of a peanut allergy. Madame-Moustache/Shutterstock What next?
Unfortunately, some infants will develop food allergies even when the relevant foods are introduced in the first year of life. Managing food allergies can be a significant burden for children and families.
Several Australian trials are currently underway testing new strategies to prevent food allergies. A large trial, soon to be completed, is testing whether vitamin D supplements in infants reduce the risk of food allergies.
Another trial is testing whether the amount of eggs and peanuts a mother eats during pregnancy and breastfeeding has an influence on whether or not her baby will develop food allergies.
For most people with food allergies, avoidance of their known allergens remains the standard of care. Oral immunotherapy, which involves gradually increasing amounts of food allergen given under medical supervision, is beginning to be offered in some facilities around Australia. However, current oral immunotherapy methods have potential side effects (including allergic reactions), can involve high time commitment and cost, and don’t cure food allergies.
There is hope on the horizon for new food allergy treatments. Multiple clinical trials are underway around Australia aiming to develop safer and more effective treatments for people with food allergies.
Jennifer Koplin, Group Leader, Childhood Allergy & Epidemiology, The University of Queensland and Desalegn Markos Shifti, Postdoctoral Research Fellow, Child Health Research Centre, Faculty of Medicine, The University of Queensland
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post





Related Posts
-
Anxiety Attack vs Panic Attack: Do You Know The Difference?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
The terms are sometimes used incorrectly, but have quite different meanings. Dr. Julie Smith, psychologist, explains in this short video:
Important distinctions
Anxiety attacks are not clinically recognized terms and lack a clear definition, often used to describe a build-up of anxiety before anticipated stressful events (e.g. social gatherings, medical appointments, etc, though of course what it is will vary from person to person—not everyone finds the same things stressful, or has the same kinds of anticipations around things).
Panic attacks, in contrast, are sudden surges of intense fear or discomfort that peak within minutes. They are characterized by symptoms including at least 4 of:
- palpitations
- sweating
- shortness of breath
- chest pain
- dizziness
- fear of losing control or dying
There’s a misconception that panic attacks never have identifiable triggers while anxiety attacks always do.
In reality, both can occur with or without a clear cause. Panic attacks can arise from various conditions, including trauma, OCD, or phobias, and don’t necessarily mean you have a panic disorder. They can also occur as a drug response, without any known underlying psychological condition.
You may also notice that that list of symptoms has quite a bit of overlap with the symptoms of a heart attack, which a) does not help people to calm down b) can, on the flipside, cause a heart attack to be misdiagnosed as a panic attack.
In terms of management:
- In the moment: breathing exercises, like extending your exhalation (a common example is the “7-11” method, inhaling for 7 seconds and exhaling for 11 seconds), can calm the body and reduce panic symptoms.
- More generally: to prevent panic attacks from becoming more frequent, avoid avoiding safe environments that triggered an attack, like supermarkets or social gatherings. Gradual exposure helps reduce anxiety over time, while avoidance can worsen it.
If panic attacks persist, Dr. Smith advises to seek help from a doctor or psychologist to understand their root causes and develop effective coping strategies.
For more on all of this, enjoy:
Click Here If The Embedded Video Doesn’t Load Automatically!
Want to learn more?
You might also like to read:
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

In This Oklahoma Town, Most Everyone Knows Someone Who’s Been Sued by the Hospital
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
McALESTER, Okla. — It took little more than an hour for Deborah Hackler to dispense with the tall stack of debt collection lawsuits that McAlester Regional Medical Center recently brought to small-claims court in this Oklahoma farm community.
Hackler, a lawyer who sues patients on behalf of the hospital, buzzed through 51 cases, all but a handful uncontested, as is often the case. She bantered with the judge as she secured nearly $40,000 in judgments, plus 10% in fees for herself, according to court records.
It’s a payday the hospital and Hackler have shared frequently over the past three decades, records show. The records indicate McAlester Regional Medical Center and an affiliated clinic have filed close to 5,000 debt collection cases since the early 1990s, most often represented by the father-daughter law firm of Hackler & Hackler.
Some of McAlester’s 18,000 residents have been taken to court multiple times. A deputy at the county jail and her adult son were each sued recently, court records show. New mothers said they compare stories of their legal run-ins with the medical center.
“There’s a lot that’s not right,” Sherry McKee, a dorm monitor at a tribal boarding school outside McAlester, said on the courthouse steps after the hearing. The hospital has sued her three times, most recently over a $3,375 bill for what she said turned out to be vertigo.
In recent years, major health systems in Virginia, North Carolina, and elsewhere have stopped suing patients following news reports about lawsuits. And several states, such as Maryland and New York, have restricted the legal actions hospitals can take against patients.
But with some 100 million people in the U.S. burdened by health care debt, medical collection cases still clog courtrooms across the country, researchers have found. In places like McAlester, a hospital’s debt collection machine can hum away quietly for years, helped along by powerful people in town. An effort to limit hospital lawsuits failed in the Oklahoma Legislature in 2021.
In McAlester, the lawsuits have provided business for some, such as the Adjustment Bureau, a local collection agency run out of a squat concrete building down the street from the courthouse, and for Hackler, a former president of the McAlester Area Chamber of Commerce. But for many patients and their families, the lawsuits can take a devastating toll, sapping wages, emptying retirement accounts, and upending lives.
McKee said she wasn’t sure how long it would take to pay off the recent judgment. Her $3,375 debt exceeds her monthly salary, she said.
“This affects a large number of people in a small community,” said Janet Roloff, an attorney who has spent years assisting low-income clients with legal issues such as evictions in and around McAlester. “The impact is great.”
Settled more than a century ago by fortune seekers who secured land from the Choctaw Nation to mine coal in the nearby hills, McAlester was once a boom town. Vestiges of that era remain, including a mammoth, 140-foot-tall Masonic temple that looms over the city.
Recent times have been tougher for McAlester, now home by one count to 12 marijuana dispensaries and the state’s death row. The downtown is pockmarked by empty storefronts, including the OKLA theater, which has been dark for decades. Nearly 1 in 5 residents in McAlester and the surrounding county live below the federal poverty line.
The hospital, operated by a public trust under the city’s authority, faces its own struggles. Paint is peeling off the front portico, and weeds poke up through the parking lots. The hospital has operated in the red for years, according to independent audit reports available on the state auditor’s website.
“I’m trying to find ways to get the entire community better care and more care,” said Shawn Howard, the hospital’s chief executive. Howard grew up in McAlester and proudly noted he started his career as a receptionist in the hospital’s physical therapy department. “This is my hometown,” he said. “I am not trying to keep people out of getting care.”
The hospital operates a clinic for low-income patients, whose webpage notes it has “limited appointments” at no cost for patients who are approved for aid. But data from the audits shows the hospital offers very little financial assistance, despite its purported mission to serve the community.
In the 2022 fiscal year, it provided just $114,000 in charity care, out of a total operating budget of more than $100 million, hospital records show. Charity care totaling $2 million or $3 million out of a $100 million budget would be more in line with other U.S. hospitals.
While audits show few McAlester patients get financial aid, many get taken to court.
Renee Montgomery, the city treasurer in an adjoining town and mother of a local police officer, said she dipped into savings she’d reserved for her children and grandchildren after the hospital sued her last year for more than $5,500. She’d gone to the emergency room for chest pain.
Dusty Powell, a truck driver, said he lost his pickup and motorcycle when his wages were garnished after the hospital sued him for almost $9,000. He’d gone to the emergency department for what turned out to be gastritis and didn’t have insurance, he said.
“Everyone in this town probably has a story about McAlester Regional,” said another former patient who spoke on the condition she not be named, fearful to publicly criticize the hospital in such a small city. “It’s not even a secret.”
The woman, who works at an Army munitions plant outside town, was sued twice over bills she incurred giving birth. Her sister-in-law has been sued as well.
“It’s a good-old-boy system,” said the woman, who lowered her voice when the mayor walked into the coffee shop where she was meeting with KFF Health News. Now, she said, she avoids the hospital if her children need care.
Nationwide, most people sued in debt collection cases never challenge them, a response experts say reflects widespread misunderstanding of the legal process and anxiety about coming to court.
At the center of the McAlester hospital’s collection efforts for decades has been Hackler & Hackler.
Donald Hackler was city attorney in McAlester for 13 years in the ’70s and ’80s and a longtime member of the local Lions Club and the Scottish Rite Freemasons.
Daughter Deborah Hackler, who joined the family firm 30 years ago, has been a deacon at the First Presbyterian Church of McAlester and served on the board of the local Girl Scouts chapter, according to the McAlester News-Capital newspaper, which named her “Woman of the Year” in 2007. Since 2001, she also has been a municipal judge in McAlester, hearing traffic cases, including some involving people she has sued on behalf of the hospital, municipal and county court records show.
For years, the Hacklers’ debt collection cases were often heard by Judge James Bland, who has retired from the bench and now sits on the hospital board. Bland didn’t respond to an inquiry for interview.
Hackler declined to speak with KFF Health News after her recent court appearance. “I’m not going to visit with you about a current client,” she said before leaving the courthouse.
Howard, the hospital CEO, said he couldn’t discuss the lawsuits either. He said he didn’t know the hospital took its patients to court. “I had to call and ask if we sue people,” he said.
Howard also said he didn’t know Deborah Hackler. “I never heard her name before,” he said.
Despite repeated public records requests from KFF Health News since September, the hospital did not provide detailed information about its financial arrangement with Hackler.
McAlester Mayor John Browne, who appoints the hospital’s board of trustees, said he, too, didn’t know about the lawsuits. “I hadn’t heard anything about them suing,” he said.
At the century-old courthouse in downtown McAlester, it’s not hard to find the lawsuits, though. Every month or two, another batch fills the docket in the small-claims court, now presided over by Judge Brian McLaughlin.
After court recently, McLaughlin, who is not from McAlester, shook his head at the stream of cases and patients who almost never show up to defend themselves, leaving him to issue judgment after judgment in the hospital’s favor.
“All I can do is follow the law,” said McLaughlin. “It doesn’t mean I like it.”
About This Project
“Diagnosis: Debt” is a reporting partnership between KFF Health News and NPR exploring the scale, impact, and causes of medical debt in America.
The series draws on original polling by KFF, court records, federal data on hospital finances, contracts obtained through public records requests, data on international health systems, and a yearlong investigation into the financial assistance and collection policies of more than 500 hospitals across the country.
Additional research was conducted by the Urban Institute, which analyzed credit bureau and other demographic data on poverty, race, and health status for KFF Health News to explore where medical debt is concentrated in the U.S. and what factors are associated with high debt levels.
The JPMorgan Chase Institute analyzed records from a sampling of Chase credit card holders to look at how customers’ balances may be affected by major medical expenses. And the CED Project, a Denver nonprofit, worked with KFF Health News on a survey of its clients to explore links between medical debt and housing instability.
KFF Health News journalists worked with KFF public opinion researchers to design and analyze the “KFF Health Care Debt Survey.” The survey was conducted Feb. 25 through March 20, 2022, online and via telephone, in English and Spanish, among a nationally representative sample of 2,375 U.S. adults, including 1,292 adults with current health care debt and 382 adults who had health care debt in the past five years. The margin of sampling error is plus or minus 3 percentage points for the full sample and 3 percentage points for those with current debt. For results based on subgroups, the margin of sampling error may be higher.
Reporters from KFF Health News and NPR also conducted hundreds of interviews with patients across the country; spoke with physicians, health industry leaders, consumer advocates, debt lawyers, and researchers; and reviewed scores of studies and surveys about medical debt.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Subscribe to KFF Health News’ free Morning Briefing.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What We Don’t Talk About When We Talk About Fat – by Aubrey Gordon
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
There are books aplenty to encourage and help you to lose weight. This isn’t one of those.
There are also books aplenty to encourage and help you to accept yourself and your body at the weight you are, and forge self-esteem. This isn’t one of those, either—in fact, it starts by assuming you already have that.
There are fair arguments for body neutrality, and fat acceptance. Very worthy also is the constant fight for bodily sovereignty.
These are worthy causes, but they’re for the most-part not what our author concerns herself with here. Instead, she cares for a different and very practical goal: fat justice.
In a world where you may be turned away from medical treatment if you are over a certain size, told to lose half your bodyweight before you can have something you need, she demands better. The battle extends further than healthcare though, and indeed to all areas of life.
Ultimately, she argues, any society that will disregard the needs of the few because they’re a marginal demographic, is a society that will absolutely fail you if you ever differ from the norm in some way.
All in all, an important (and for many, perhaps eye-opening) book to read if you are fat, care about fat people, are a person of any size, or care about people in general.
Pick Up Your Copy of “What We Don’t Talk About When We Talk About Fat”, on Amazon Today!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: