One Cause; Countless Aches
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
What Is The Cause?
Zac Cupples’ video (below) makes an appealing claim: 90% of movement issues and discomforts we experience daily come from one source: reduced joint space due to increased muscle tension.
For Cupples, this could be causing anything from knee pain to foot pain to ankle pain to hip pain to generalized joint pain to…pretty much any sort of pain.
So, why do we describe this as “appealing”?
Well, if there’s just one cause, that means there is only one thing to fix
Can This Be True?
Whilst we normally stray away from oversimplifications, we found Cupples’ example quite powerful.
Cupples defends his thesis by illustrating it with a simple wrist movement experiment: try moving your wrist in a circle with your palm open, and then do the same with your fist clenched.
Did you notice a difference?
When you clench your fist, movement (normally) becomes restricted and uncomfortable, illustrating how increased tension limits joint space.
It’s a powerful analogy for understanding our body’s mechanics.
So How Do We Fix It?
To combat issues with reduced joint space, Cupples proposes a three-step solution: reducing muscle tension, increasing range of motion in commonly limited areas, and enhancing movement efficiency. He delves into strategies for achieving these, including adopting certain positions and breathing techniques.
There are also some elements of strategic muscle engagement, but we’ll leave that to him to describe:
How was the video? If you’ve discovered any great videos yourself that you’d like to share with fellow 10almonds readers, then please do email them to us!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Recommended

Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

What’s the difference between a heart attack and cardiac arrest? One’s about plumbing, the other wiring

10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
In July 2023, rising US basketball star Bronny James collapsed on the court during practice and was sent to hospital. The 18-year-old athlete, son of famous LA Lakers’ veteran LeBron James, had experienced a cardiac arrest.
Many media outlets incorrectly referred to the event as a “heart attack” or used the terms interchangeably.
A cardiac arrest and a heart attack are distinct yet overlapping concepts associated with the heart.
With some background in how the heart works, we can see how they differ and how they’re related.

Explode/Shutterstock Understanding the heart
The heart is a muscle that contracts to work as a pump. When it contracts it pushes blood – containing oxygen and nutrients – to all the tissues of our body.
For the heart muscle to work effectively as a pump, it needs to be fed its own blood supply, delivered by the coronary arteries. If these arteries are blocked, the heart muscle doesn’t get the blood it needs.
This can cause the heart muscle to become injured or die, and results in the heart not pumping properly.
Heart attack or cardiac arrest?
Simply put, a heart attack, technically known as a myocardial infarction, describes injury to, or death of, the heart muscle.
A cardiac arrest, sometimes called a sudden cardiac arrest, is when the heart stops beating, or put another way, stops working as an effective pump.
In other words, both relate to the heart not working as it should, but for different reasons. As we’ll see later, one can lead to the other.
Why do they happen? Who’s at risk?
Heart attacks typically result from blockages in the coronary arteries. Sometimes this is called coronary artery disease, but in Australia, we tend to refer to it as ischaemic heart disease.
The underlying cause in about 75% of people is a process called atherosclerosis. This is where fatty and fibrous tissue build up in the walls of the coronary arteries, forming a plaque. The plaque can block the blood vessel or, in some instances, lead to the formation of a blood clot.
Atherosclerosis is a long-term, stealthy process, with a number of risk factors that can sneak up on anyone. High blood pressure, high cholesterol, diet, diabetes, stress, and your genes have all been implicated in this plaque-building process.
Other causes of heart attacks include spasms of the coronary arteries (causing them to constrict), chest trauma, or anything else that reduces blood flow to the heart muscle.
Regardless of the cause, blocking or reducing the flow of blood through these pipes can result in the heart muscle not receiving enough oxygen and nutrients. So cells in the heart muscle can be injured or die.
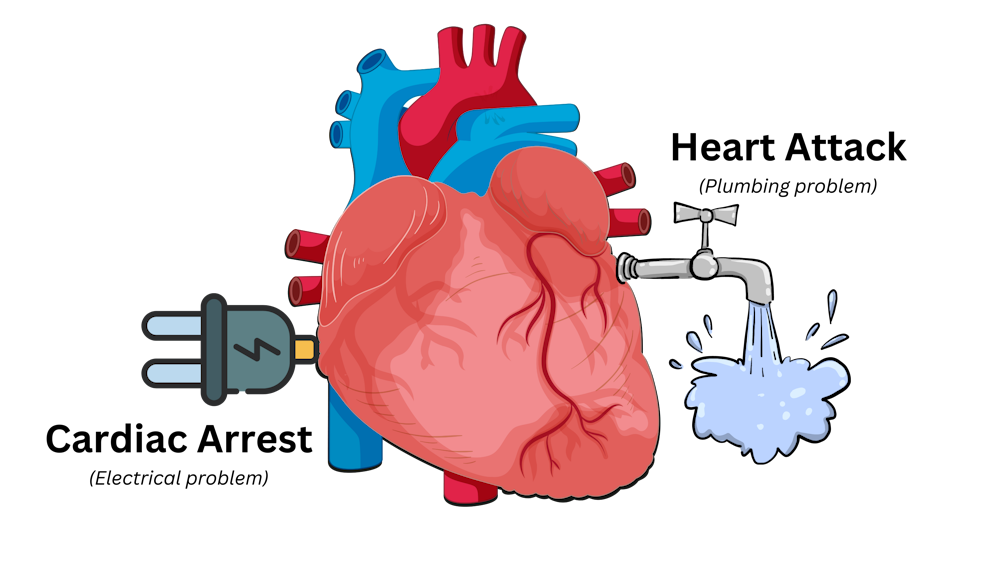
Here’s a simple way to remember the difference. Author provided But a cardiac arrest is the result of heartbeat irregularities, making it harder for the heart to pump blood effectively around the body. These heartbeat irregularities are generally due to electrical malfunctions in the heart. There are four distinct types:
- ventricular tachycardia: a rapid and abnormal heart rhythm in which the heartbeat is more than 100 beats per minute (normal adult, resting heart rate is generally 60-90 beats per minute). This fast heart rate prevents the heart from filling with blood and thus pumping adequately
- ventricular fibrillation: instead of regular beats, the heart quivers or “fibrillates”, resembling a bag of worms, resulting in an irregular heartbeat greater than 300 beats per minute
- pulseless electrical activity: arises when the heart muscle fails to generate sufficient pumping force after electrical stimulation, resulting in no pulse
- asystole: the classic flat-line heart rhythm you see in movies, indicating no electrical activity in the heart.
Remember this flat-line rhythm from the movies? It’s asystole, when there’s no electrical activity in the heart. Kateryna Kon/Shutterstock Cardiac arrest can arise from numerous underlying conditions, both heart-related and not, such as drowning, trauma, asphyxia, electrical shock and drug overdose. James’ cardiac arrest was attributed to a congenital heart defect, a heart condition he was born with.
But among the many causes of a cardiac arrest, ischaemic heart disease, such as a heart attack, stands out as the most common cause, accounting for 70% of all cases.
So how can a heart attack cause a cardiac arrest? You’ll remember that during a heart attack, heart muscle can be damaged or parts of it may die. This damaged or dead tissue can disrupt the heart’s ability to conduct electrical signals, increasing the risk of developing arrhythmias, possibly causing a cardiac arrest.
So while a heart attack is a common cause of cardiac arrest, a cardiac arrest generally does not cause a heart attack.
What do they look like?
Because a cardiac arrest results in the sudden loss of effective heart pumping, the most common signs and symptoms are a sudden loss of consciousness, absence of pulse or heartbeat, stopping of breathing, and pale or blue-tinged skin.
But the common signs and symptoms of a heart attack include chest pain or discomfort, which can show up in other regions of the body such as the arms, back, neck, jaw, or stomach. Also frequent are shortness of breath, nausea, light-headedness, looking pale, and sweating.
What’s the take-home message?
While both heart attack and cardiac arrest are disorders related to the heart, they differ in their mechanisms and outcomes.
A heart attack is like a blockage in the plumbing supplying water to a house. But a cardiac arrest is like an electrical malfunction in the house’s wiring.
Despite their different nature both conditions can have severe consequences and require immediate medical attention.
Michael Todorovic, Associate Professor of Medicine, Bond University and Matthew Barton, Senior lecturer, School of Nursing and Midwifery, Griffith University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Share This Post
-
Do We Need Sunscreen In Winter, Really?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I keep seeing advice that we shoudl wear sunscreen out in winter even if it’s not hot or sunny, but is there actually any real benefit to this?❞
Short answer: yes (but it’s indeed not as critical as it is during summer’s hot/sunny days)
Longer answer: first, let’s examine the physics of summer vs winter when it comes to the sun…
In summer (assuming we live far enough from the equator to have this kind of seasonal variation), the part of the planet where we live is tilted more towards the sun. This makes it closer, and more importantly, it’s more directly overhead during the day. The difference in distance through space isn’t as big a deal as the difference in distance through the atmosphere. When the sun is more directly overhead, its rays have a shorter path through our atmosphere, and thus less chance of being blocked by cloud cover / refracted elsewhere / bounced back off into space before it even gets that far.
In winter, the opposite of all that is true.
Morning/evening also somewhat replicate this compared to midday, because the sun being lower in the sky has a similar effect to seasonal variation causing it to be less directly overhead.
For this reason, even though visually the sun may be just as bright on a winter morning as it is on a summer midday, the rays have been filtered very differently by the time they get to us.
This is one reason why you’re much less likely to get sunburned in the winter, compared to the summer (others include the actual temperature difference, your likely better hydration, and your likely more modest attire protecting you).
However…
The reason it is advisable to wear sunscreen in winter is not generally about sunburn, and is rather more about long-term cumulative skin damage (ranging from accelerated aging to cancer) caused by the UV rays—specifically, mostly UVA rays, since UVB rays (with their higher energy but shorter wavelength) have nearly all been blocked by the atmosphere.
Here’s a good explainer of that from the American Cancer Society:
UV (Ultraviolet) Radiation and Cancer Risk
👆 this may seem like a no-brainer, but there’s a lot explained here that demystifies a lot of things, covering ionizing vs non-ionizing radiation, x-rays and gamma-rays, the very different kinds of cancer caused by different things, and what things are dangerous vs which there’s no need to worry about (so far as best current science can say, at least).
Consequently: yes, if you value your skin health and avoidance of cancer, wearing sunscreen when out even in the winter is a good idea. Especially if your phone’s weather app says the UV index is “moderate” or above, but even if it’s “low”, it doesn’t hurt to include it as part of your skincare routine.
But what if sunscreens are dangerous?
Firstly, not all sunscreens are created equal:
Learn more: Who Screens The Sunscreens?
Secondly: consider putting on a protective layer of moisturizer first, and then the sunscreen on top. Bear in mind, this is winter we’re talking about, so you’re probably not going out in a bikini, so this is likely a face-neck-hands job and you’re done.
What about vitamin D?
Humans evolved to have more or less melanin in our skin depending on where we lived, and white people evolved to wring the most vitamin D possible out of the meagre sun far from the equator. Black people’s greater melanin, on the other hand, offers some initial protection against the sun (but any resultant skin cancer is then more dangerous than it would be for white people if it does occur, so please do use sunscreen whatever your skintone).
Nowadays many people live in many places which may or may not be the places we evolved for, and so we have to take that into account when it comes to sun exposure.
Here’s a deeper dive into that, for those who want to learn:
Take care!
Share This Post
-

Anti-Cholesterol Cardamom & Pistachio Porridge
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
This tasty breakfast’s beta-glucan content binds to cholesterol and carries it out of the body; there are lots of other nutritional benefits too!
You will need
- 1 cup coconut milk
- ⅓ cup oats
- 4 tbsp crushed pistachios
- 6 cardamom pods, crushed
- 1 tsp rose water or 4 drops edible rose essential oil
- Optional sweetener: drizzle of honey or maple syrup
- Optional garnishes: rose petals, chopped nuts, dried fruit
Method
(we suggest you read everything at least once before doing anything)
1) Heat the coconut milk, adding the oats and crushed cardamom pods. Simmer for 5–10 minutes depending on how cooked you want the oats to be.
2) Stir in the crushed pistachio nuts, as well as the rose water.
3) Serve in a bowl, adding any optional toppings:
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- The Best Kind Of Fiber For Overall Health? ← it’s beta-glucan, which is fund abundantly in oats
- Pistachios vs Pecans – Which is Healthier? ← have a guess
- Can Saturated Fats Be Healthy? ← coconut can!
Take care!
Share This Post



Related Posts
-

What happens when I stop taking a drug like Ozempic or Mounjaro?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Hundreds of thousands of people worldwide are taking drugs like Ozempic to lose weight. But what do we actually know about them? This month, The Conversation’s experts explore their rise, impact and potential consequences.
Drugs like Ozempic are very effective at helping most people who take them lose weight. Semaglutide (sold as Wegovy and Ozempic) and tirzepatide (sold as Zepbound and Mounjaro) are the most well known in the class of drugs that mimic hormones to reduce feelings of hunger.
But does weight come back when you stop using it?
The short answer is yes. Stopping tirzepatide and semaglutide will result in weight regain in most people.
So are these medications simply another (expensive) form of yo-yo dieting? Let’s look at what the evidence shows so far.
It’s a long-term treatment, not a short course
If you have a bacterial infection, antibiotics will help your body fight off the germs causing your illness. You take the full course of medication, and the infection is gone.
For obesity, taking tirzepatide or semaglutide can help your body get rid of fat. However it doesn’t fix the reasons you gained weight in the first place because obesity is a chronic, complex condition. When you stop the medications, the weight returns.
Perhaps a more useful comparison is with high blood pressure, also known as hypertension. Treatment for hypertension is lifelong. It’s the same with obesity. Medications work, but only while you are taking them. (Though obesity is more complicated than hypertension, as many different factors both cause and perpetuate it.)
Obesity drugs only work while you’re taking them. KK Stock/Shutterstock Therefore, several concurrent approaches are needed; taking medication can be an important part of effective management but on its own, it’s often insufficient. And in an unwanted knock-on effect, stopping medication can undermine other strategies to lose weight, like eating less.
Why do people stop?
Research trials show anywhere from 6% to 13.5% of participants stop taking these drugs, primarily because of side effects.
But these studies don’t account for those forced to stop because of cost or widespread supply issues. We don’t know how many people have needed to stop this medication over the past few years for these reasons.
Understanding what stopping does to the body is therefore important.
So what happens when you stop?
When you stop using tirzepatide or semaglutide, it takes several days (or even a couple of weeks) to move out of your system. As it does, a number of things happen:
- you start feeling hungry again, because both your brain and your gut no longer have the medication working to make you feel full
When you stop taking it, you feel hungry again. Stock-Asso/Shutterstock - blood sugars increase, because the medication is no longer acting on the pancreas to help control this. If you have diabetes as well as obesity you may need to take other medications to keep these in an acceptable range. Whether you have diabetes or not, you may need to eat foods with a low glycemic index to stabilise your blood sugars
- over the longer term, most people experience a return to their previous blood pressure and cholesterol levels, as the weight comes back
- weight regain will mostly be in the form of fat, because it will be gained faster than skeletal muscle.
While you were on the medication, you will have lost proportionally less skeletal muscle than fat, muscle loss is inevitable when you lose weight, no matter whether you use medications or not. The problem is, when you stop the medication, your body preferentially puts on fat.
Is stopping and starting the medications a problem?
People whose weight fluctuates with tirzepatide or semaglutide may experience some of the downsides of yo-yo dieting.
When you keep going on and off diets, it’s like a rollercoaster ride for your body. Each time you regain weight, your body has to deal with spikes in blood pressure, heart rate, and how your body handles sugars and fats. This can stress your heart and overall cardiovascular system, as it has to respond to greater fluctuations than usual.
Interestingly, the risk to the body from weight fluctuations is greater for people who are not obese. This should be a caution to those who are not obese but still using tirzepatide or semaglutide to try to lose unwanted weight.
How can you avoid gaining weight when you stop?
Fear of regaining weight when stopping these medications is valid, and needs to be addressed directly. As obesity has many causes and perpetuating factors, many evidence-based approaches are needed to reduce weight regain. This might include:
- getting quality sleep
- exercising in a way that builds and maintains muscle. While on the medication, you will likely have lost muscle as well as fat, although this is not inevitable, especially if you exercise regularly while taking it
Prioritise building and maintaining muscle. EvMedvedeva/Shutterstock - addressing emotional and cultural aspects of life that contribute to over-eating and/or eating unhealthy foods, and how you view your body. Stigma and shame around body shape and size is not cured by taking this medication. Even if you have a healthy relationship with food, we live in a culture that is fat-phobic and discriminates against people in larger bodies
- eating in a healthy way, hopefully continuing with habits that were formed while on the medication. Eating meals that have high nutrition and fibre, for example, and lower overall portion sizes.
Many people will stop taking tirzepatide or semaglutide at some point, given it is expensive and in short supply. When you do, it is important to understand what will happen and what you can do to help avoid the consequences. Regular reviews with your GP are also important.
Read the other articles in The Conversation’s Ozempic series here.
Natasha Yates, General Practitioner, PhD Candidate, Bond University
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-

Loaded Mocha Chocolate Parfait
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
Packed with nutrients, including a healthy dose of protein and fiber, these parfait pots can be a healthy dessert, snack, or even breakfast!
You will need (for 4 servings)
For the mocha cream:
- ½ cup almond milk
- ½ cup raw cashews
- ⅓ cup espresso
- 2 tbsp maple syrup
- 1 tsp vanilla extract
For the chocolate sauce:
- 4 tbsp coconut oil, melted
- 2 tbsp unsweetened cocoa powder
- 1 tbsp maple syrup
- 1 tsp vanilla extract
For the other layers:
- 1 banana, sliced
- 1 cup granola, no added sugar
Garnish (optional): 3 coffee beans per serving
Note about the maple syrup: since its viscosity is similar to the overall viscosity of the mocha cream and chocolate sauce, you can adjust this per your tastes, without affecting the composition of the dish much besides sweetness (and sugar content). If you don’t like sweetness, the maple syrup be reduced or even omitted entirely (your writer here is known for her enjoyment of very strong bitter flavors and rarely wants anything sweeter than a banana); if you prefer more sweetness than the recipe called for, that’s your choice too.
Method
(we suggest you read everything at least once before doing anything)
1) Blend all the mocha cream ingredients. If you have time, doing this in advance and keeping it in the fridge for a few hours (or even up to a week) will make the flavor richer. But if you don’t have time, that’s fine too.
2) Stir all the chocolate sauce ingredients together in a small bowl, and set it aside. This one should definitely not be refrigerated, or else the coconut oil will solidify and separate itself.
3) Gently swirl the the mocha cream and chocolate sauce together. You want a marble effect, not a full mixing. Omit this step if you want clearer layers.
4) Assemble in dessert glasses, alternating layers of banana, mocha chocolate marble mixture (or the two parts, if you didn’t swirl them together), and granola.
5) Add the coffee-bean garnish, if using, and serve!
Enjoy!
Want to learn more?
For those interested in some of the science of what we have going on today:
- Enjoy Bitter Foods For Your Heart & Brain
- The Bitter Truth About Coffee (Or Is It?)
- Which Sugars Are Healthier, And Which Are Just The Same?
- Cashew Nuts vs Coconut – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails:
-
Does Eating Shellfish Contribute To Gout?
10almonds is reader-supported. We may, at no cost to you, receive a portion of sales if you purchase a product through a link in this article.
It’s Q&A Day at 10almonds!
Have a question or a request? We love to hear from you!
In cases where we’ve already covered something, we might link to what we wrote before, but will always be happy to revisit any of our topics again in the future too—there’s always more to say!
As ever: if the question/request can be answered briefly, we’ll do it here in our Q&A Thursday edition. If not, we’ll make a main feature of it shortly afterwards!
So, no question/request too big or small 😎
❝I have a question about seafood as healthy, doesn’t eating shellfish contribute to gout?❞
It can do! Gout (a kind of inflammatory arthritis characterized by the depositing of uric acid crystals in joints) has many risk factors, and diet is one component, albeit certainly the most talked-about one.
First, you may be wondering: isn’t all arthritis inflammatory? Since arthritis is by definition the inflammation of joints, this is a reasonable question, but when it comes to classifying the kinds, “inflammatory” arthritis is caused by inflammation, while “non-inflammatory” arthritis (a slightly confusing name) merely has inflammation as one of its symptoms (and is caused by physical wear-and-tear). For more information, see:
- Tips For Avoiding/Managing Rheumatoid Arthritis ←inflammatory
- Tips For Avoiding/Managing Osteoarthritis ← “non-inflammatory”
As for gout specifically, top risk factors include:
- Increasing age: risk increases with age
- Being male: women do get gout, but much less often
- Hypertension: all-cause hypertension is the biggest reasonably controllable factor
There’s not a lot we can do about age (but of course, looking after our general health will tend to slow biological aging, and after all, diseases only care about the state of our body, not what the date on the calendar is).
As for sex, this risk factor is hormones, and specifically has to do with estrogen and testosterone’s very different effects on the immune system (bearing in mind that chronic inflammation is a disorder of the immune system). However, few if any men would take up feminizing hormone therapy just to lower their gout risk!
That leaves hypertension, which happily is something that we can all (barring extreme personal circumstances) do quite a bit about. Here’s a good starting point:
Hypertension: Factors Far More Relevant Than Salt
…and for further pointers:
How To Lower Your Blood Pressure (Cardiologists Explain)
As for diet specifically (and yes, shellfish):
The largest study into this (and thus, one of the top ones cited in a lot of other literature) looked at 47,150 men with no history of gout at the baseline.
So, with the caveat that their findings could have been different for women, they found:
- Eating meat in general increased gout risk
- Narrowing down specific meats: beef, pork, and lamb were the worst offenders
- Eating seafood in general increased gout risk
- Narrowing down specific seafoods: all seafoods increased gout risk within a similar range
- As a specific quirk of seafoods: the risk was increased if the man had a BMI under 25
- Eating dairy in general was not associated with an increased risk of gout
- Narrowing down specific dairy foods: low-fat dairy products such as yogurt were associated with a decreased risk of gout
- Eating purine-rich vegetables in general was not associated with an increased risk of gout
- Narrowing down to specific purine-rich vegetables: no purine-rich vegetable was associated with an increase in the risk of gout
Dairy products were included in the study, as dairy products in general and non-fermented dairy products in particular are often associated with increased inflammation. However, the association was simply not found to exist when it came to gout risk.
Purine-rich vegetables were included in the study, as animal products highest in purines have typically been found to have the worst effect on gout. However, the association was simply not found to exist when it came to plants with purines.
You can read the full study here:
Purine-Rich Foods, Dairy and Protein Intake, and the Risk of Gout in Men
So, the short answer to your question of “doesn’t eating shellfish contribute to the risk of gout” is:
Yes, it can, but occasional consumption probably won’t result in gout unless you have other risk factors going against you.
If you’re a slim male 80-year-old alcoholic smoker with hypertension, then definitely do consider skipping the lobster, but honestly, there may be bigger issues to tackle there.
And similarly, obviously skip it if you have a shellfish allergy, and if you’re vegan or vegetarian or abstain from shellfish for religious reasons, then you can certainly live very healthily without ever having any.
See also: Do We Need Animal Products, To Be Healthy?
For most people most of the time, a moderate consumption of seafood, including shellfish if you so desire, is considered healthy.
As ever, do speak with your own doctor to know for sure, as your individual case may vary.
For reference, this question was surely prompted by the article:
Lobster vs Crab – Which is Healthier?
Take care!
Don’t Forget…
Did you arrive here from our newsletter? Don’t forget to return to the email to continue learning!
Learn to Age Gracefully
Join the 98k+ American women taking control of their health & aging with our 100% free (and fun!) daily emails: